| CHAPTER XVII.
ANOMALOUS NERVOUS AND MENTAL DISEASES. Anomalies and Curiosities of Medicine | ||
17. CHAPTER XVII.
ANOMALOUS NERVOUS AND MENTAL DISEASES.
Epilepsy has been professionally recognized as a distinct type of disease since the time of Hippocrates, but in earlier times, and popularly throughout later times, it was illy defined. The knowledge of the clinical symptoms has become definite only since the era of cerebral local anatomy and localization. Examination of the older records of epilepsy shows curious forms recorded. The Ephemerides speaks of epilepsy manifested only on the birthday. Testa *[758] mentions epilepsy recurring at the festival of St. John, and Bartholinus *[190] reports a case in which the convulsions corresponded with the moon's phases. Paullini *[620] describes epilepsy which occurred during the blowing of wind from the south, and also speaks of epilepsy during the paroxysms of which the individual barked. Fabricius *[332] and the Ephemerides record dancing epilepsy. Bartholinus and Hagendorn mention cases during which various splendors appeared before the eyes during the paroxysm. Godart [17.1] Portius, and Salmuth *[706] speak of visions occurring before and after epileptic paroxysms. The Ephemerides contains records of epilepsy in which blindness preceded the paroxysm, in which there was singing during it, and a case in which the paroxysm was attended with singultus. Various older writers mention cases of epilepsy in which curious spots appeared on the face; and the kinds of aura mentioned are too numerous to transcribe.
Baly [17.2] mentions a case of epilepsy occasioned by irritation in the socket of a tooth. Webber [17.3] reports a case of epilepsy due to phimosis and to irritation from a tooth. Beardsley [17.4] speaks of an attempt at strangulation that produced epilepsy. Brown-Séquard [17.5] records an instance produced by injury to the sciatic nerve. Doyle [17.6] gives an account of the production of epilepsy from protracted bathing in a pond. Duncan [17.7] cites an instance of epilepsy connected with vesical calculus that was cured by lithotomy. Museroft mentions an analogous case. Greenhow [17.8] speaks of epilepsy arising from an injury to the thumb. Garmannus, early in the eighteenth century, describes epilepsy arising from fright and terror. Bristowe in 1880, and Farre [17.9] speak of similar instances. In Farre's case the disease was temporarily cured by
There is a peculiar case of running epilepsy recorded. [17.10] The patient was a workman who would be suddenly seized with a paroxysm, and unconsciously run some distance at full speed. On one occasion he ran from Peterborough to Whittlesey, where he was stopped and brought back. Once he ran into a pit containing six feet of water, from which he was rescued. Yeo [17.11] says that sexual intercourse occasionally induces epilepsy, and relates a case in which a severe epileptic fit terminated fatally three days after the seizure, which occurred on the nuptial night.
Drake [17.12] reports the case of a man who was wounded in the War of 1812, near Baltimore, the ball passing along the left ear and temple so close as to graze the skin. Eighteen years after the accident he suffered with pain in the left ear and temple, accompanied by epileptic fits and partial amnesia, together with an entire loss of power of remembering proper names and applying them to the objects to which they belonged. He would, for instance, invariably write Kentucky for Louisville. Beirne [17.13] records the case of a dangerous lunatic, an epileptic, who was attacked by a fellow-inmate and sustained an extensive fracture of the right parietal bone, with great hemorrhage, followed by coma. Strange to say, after the accident he recovered his intellect, and was cured of his epileptic attacks, but for six years he was a paralytic from the hips down.
The Dancing Mania.—Chorea has appeared in various epidemic forms under the names of St. Vitus's dance, St. Guy's dance, St. Anthony's dance, choromania, tanzplage, orchestromania, dance of St. Modesti or St. John, the dancing mania, etc.; although these various functional phenomena of the nervous system have been called chorea, they bear very little resemblance to what, at the present day, is called by this name. The epidemic form appeared about 1374, although Hecker *[408] claims that, at that time, it was no new thing. Assemblages of men and women were seen at Aix-la-Chapelle who, impelled by a common delusion, would form circles, hand in hand, and dance in wild delirium until they fell to the ground exhausted, somewhat after the manner of the Ghost-Dance or Messiah-Dance of our North American Indians. In their Bacchantic leaps they were apparently haunted by visions and hallucinations, the fancy conjuring up spirits whose names they shrieked out. Some of them afterward stated that they appeared to be immersed in a stream of blood which obliged them to leap so high. Others saw the
Paracelsus called this malady (Chorus sancti viti) the lascivious dance, and says that persons stricken with it were helpless until relieved by either recovery or death. The malady spread rapidly through France and Holland, and before the close of the century was introduced into England. In his "Anatomy of Melancholy'' Burton refers to it, and speaks of the idiosyncrasies of the individuals afflicted. It is said they could not abide one in red clothes, and that they loved music above all things, and also that the magistrates in Germany hired musicians to give them music, and provided them with sturdy companions to dance with. Their endurance was marvelous. Plater speaks of a woman in Basle whom he saw, that danced for a month. In Strasburg many of them ate nothing for days and nights until their mania subsided. Paracelsus, in the beginning of the sixteenth century, was the first to make a study of this disease. He outlined the severest treatment for it, and boasted that he cured many of the victims. Hecker conjectures that probably the wild revels of St. John's day, 1374, gave rise to this mental plague, which thenceforth visited so many thousands with incurable aberrations of mind and disgusting distortions of the body. Almost simultaneous with the dance of "St. With,'' there appeared in Italy and Arabia a mania very similar in character which was called "tarantism,'' which was supposed to originate in the bite of the tarantula. The only effective remedy was music in some form. In the Tigrè country, Abyssinia, this disease appeared under the name of "Tigretier.'' The disease, fortunately, rapidly declined, and very little of it seems to have been known in the sixteenth century, but in the early part of the eighteenth century a peculiar sect called the "Convulsionnaires'' arose in France; and throughout England among the Methodist sect, insane convulsions of this nature were witnessed; and even to the present
Paracelsus divided the sufferers of St. Vitus's dance into three classes .—
(1) Those in which the affliction arose from imagination (chorea imaginativa).
(2) Those which had their origin in sexual desires depending on the will.
(3) Those arising from corporeal causes (chorea naturalis). This last case, according to a strange notion of his own he explained by maintaining that in certain vessels which are susceptible of an internal pruriency, and thence produced laughter, the blood is set into commotion in consequence of an alteration in the vital spirits, whereby are occasioned involuntary fits of intoxicating joy, and a propensity to dance. The great physician Sydenham gave the first accurate description of what is to-day called chorea, and hence the disease has been named "Sydenham's chorea.'' So true to life was his portrayal of the disease that it has never been surpassed by modern observers.
The disease variously named palmus, the jumpers, the twitchers, lata, miryachit, or, as it is sometimes called, the emeryaki of Siberia, and the tic-convulsif of La Tourette, has been very well described by Gray [17.14] who says that the French authors had their attention directed to the subject by the descriptions of two American authors—those of Beard upon "The Jumpers of Maine,'' published in 1880, and that of Hammond upon "Miryachit,'' a similar disease of the far Orient. Beard found that the jumpers of Maine did unhesitatingly whatever they were told to do. Thus, one who was sitting in a chair was told to throw a knife that he had in his hand, and he obeyed so quickly that the weapon stuck in a house opposite; at the same time he repeated the command given him, with a cry of alarm not unlike that of hysteria or epilepsy. When he was suddenly clapped upon the shoulder he threw away his pipe, which he had been filling with tobacco. The first parts of Virgil's æneid and Homer's Iliad were recited to one of these illiterate jumpers, and he repeated the words as they came to him in a sharp voice, at the same time jumping or throwing whatever he had in his hand, or raising his shoulder, or making some other violent motion. It is related by O'Brien, an Irishman serving on an English naval vessel, that an elderly and respectable Malay woman, with whom he was conversing in an entirely unsuspecting manner, suddenly began to undress herself, and showed a most ominous and determined intention of stripping herself completely, and all because a by-standing friend had suddenly taken off his coat; at the same time she manifested the most violent anger at what she deemed this outrage to her sex, calling the astonished friend an abandoned hog, and begging O'Brien to kill him. O'Brien, furthermore, tells of a cook who was carrying his child in his arms over the bridge of a river, while at the same time a sailor carried a log of wood in like manner; the sailor threw his log
Gray has seen only one case of acute palmus, and records it as follows: "It was in a boy of six, whose heredity, so far as I could ascertain from the statements of his mother, was not neurotic. He had had trouble some six months before coming to me. He had been labeled with a number of interesting diagnoses, such as chorea, epilepsy, myotonia, hysteria, and neurasthenia. His palmodic movements were very curious. When standing near a table looking at something, the chin would suddenly come down with a thump that would leave a black-and-blue mark, or his head would be thrown violently to one side, perhaps coming in contact with some adjacent hard object with equal force, or, while standing quietly, his legs would give a sudden twitch, and he would be thrown violently to the ground, and this even happened several times when he was seated on the edge of a stool. The child was under my care for two weeks, and, probably because of an intercurrent attack of diarrhea, grew steadily worse during that time, in spite of the full doses of arsenic which were administered to him. He was literally covered with bruises from the sudden and violent contacts with articles of furniture, the floor, and the walls. At last, in despair at his condition, I ordered him to be undressed and put to bed, and steadily pushed the Fowler's solution of arsenic until he was taking ten drops three times a day, when, to my great surprise, he began to improve rapidly, and at the end of six weeks was perfectly well. Keeping him under observation for two weeks longer I finally sent him to his home in the West, and am informed that he has since remained perfectly well. It has seemed to me that many of the cases recorded as paramyoclonus multiples have been really acute palmus.''
Gray mentions two cases of general palmus with pseudomelancholia, and describes them in the following words:—
"The muscular movements are of the usual sudden, shock-like type, and of the same extent as in what I have ventured to call the general form. With them, however, there is associated a curious pseudomelancholia, consisting of certain fixed melancholy suspicious delusions, without, however, any of the suicidal tendencies and abnormal sensations up and down the back of the head, neck, or spine, or the sleeplessness, which are characteristic of most cases of true melancholia. In both of my cases the palmus had existed for a long period, the exact limits of which, however, I could not determine, because the patient scouted the idea that he had had any trouble of the kind, but which the testimony of friends and relatives seemed to vouch for. They were
Athetosis was first described by Hammond in 1871, who gave it the name because it was mainly characterized by an inability to retain the fingers and toes in any position in which they might be planed, as well as by their continuous motion. According to Drewry [17.16] "athetosis is a cerebral affection, presenting a combination of symptoms characterized chiefly by a more or less constant mobility of the extremities and an inability to retain them in any fixed position. These morbid, grotesque, involuntary movements are slow and wavy, somewhat regular and rigid, are not jerky, spasmodic, nor tremulous. The movements of the digits are quite different from those attending any other disease, impossible to imitate even by the most skilful malingerer, and, if once seen, are not likely to be forgotten. In an athetoid hand, says Starr, the interossei and lumbricales, which flex the metacarpo-phalangeal and extend the phalangeal joints, are affected; rarely are the long extensors and the long flexors affected. Therefore the hand is usually in the so-called interosseal position, with flexion of the proximal and extension of the middle and distal phalanges. The athetoid movements of the toes correspond to those of the fingers in point of action. In a great majority of cases the disease is confined to one side (hemiathetosis), and is a sequel of hemiplegia. The differential diagnosis of athetosis is generally easily made. The only nervous affections with which it could possibly be confounded are chorea and paralysis agitans. Attention to the twitching, spasmodic, fibrillary movements, having a quick beginning and a quick ending, which is characteristic in Sydenham's chorea, would at once exclude that disease. These jerky movements peculiar to St. Vitus's dance may be easily detected in a few or many muscles, if moderate care and patience be exercised on the part of the examiner. This form of chorea is almost always a disease of childhood. So-called post-hemiplegic chorea is, in the opinion of both Hammond and Gray, simply athetosis. The silly, dancing, posturing, wiry movements, and the facial distortion observed in Huntington's chorea would hardly be mistaken by a careful observer for athetosis. The two diseases, however, are somewhat alike. Paralysis agitans (shaking palsy), with its coarse tremor, peculiar facies, immobility, shuffling gait, the `bread-crumbling' attitude of the fingers, and deliberate speech, would be readily eliminated even by a novice. It is, too, a disease of advanced
The following is the report of a case by Drewry, of double (or, more strictly speaking, quadruple) athetosis, associated with epilepsy and insanity: "The patient was a negro woman, twenty-six years old when she was admitted into this, the Central State (Va.) Hospital, in April, 1886. She had had epilepsy of the grand mal type for a number of years, was the mother of one child, and earned her living as a domestic. A careful physical examination revealed nothing of importance as an etiologic factor. Following in the footsteps of many of those unfortunates afflicted with epilepsy, she degenerated into a state of almost absolute imbecility.
"Some degree of mental deficiency seems usually to accompany athetosis, even when uncomplicated by any other degenerating neurosis. Athetoid symptoms of an aggravated character, involving both upper and both lower extremities, had developed previous to her admission into this hospital, but it was impossible to find out when and how they began. She had never had, to the knowledge of her friends, an attack of `apoplexy,' nor of paralysis. The head was symmetric, and without scars thereon. The pedal extremities involuntarily assumed various distorted positions and were constantly in motion. The toes were usually in a state of tonic spasm,—contracted, and drawn downward or extended, pointing upward, and slightly separated. Irregular alternate extension and flexion of the toes were marked. The feet were moved upon the ankles in a stiff and awkward manner. During these `complex involuntary movements,' the muscles of the calf became hard and rigid. The act of walking was accomplished with considerable difficulty, on account of contractures, and because the feet were not exactly under the control of the will. The unnatural movements of the hands corresponded to those of the lower extremities, though they were more constant and active. The fingers, including the thumbs, were usually widely separated and extended, though they were sometimes slightly flexed. The hands were continually in slow, methodic, quasi-rhythmic motion, never remaining long in the same attitude. In grasping an object the palm of the hand was used, it being difficult to approximate the digits. The wrist-joints were also implicated, there being alternate flexion and extension. In fact these odd contortions affected the entire limb from the shoulder to the digital extremities. When standing or walking the arms were held out horizontally, as if to maintain the equilibrium of the body. The patient's general physical health was fairly good. She frequently complained of headache, and when she was exceedingly irritable and violent all the athetoid movements would be intensified. Speech was jerky and disordered, which gave it a distinctive character. The special senses seemed to be unimpaired, and the pupils were normal, except when an epileptic attack came on. Death occurred in January, 1895, after an obstinate attack of status epilepticus.''
Saltatoric spasm is an extremely rare condition, first observed by Bamberger in 1859. The calf, hip, knee, and back-muscles are affected by clonic spasm, causing springing or jumping movements when the patient attempts to stand. The disease is transient, and there are no mental symptoms.
Progressive muscular atrophy has been observed as far back as Hippocrates, but it is only in recent times that we have had any definite knowledge
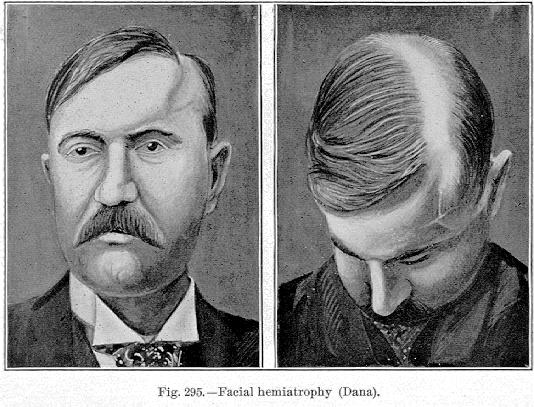
Fig. 295.—Facial hemiatrophy (Dana).
[Description: Two drawings of man with facial hemiatrophy]
of the subject. It is divided into four types, the hand type (causing the griffin-or claw-hand, or the ape-hand); the juvenile type (generally in the muscles of the shoulder and arm); the facial type; and the peroneal type. Generalized progressive atrophy leads to a condition that simulates the appearance of a "living skeleton.''
Facial hemiatrophy is an incurable disease, as yet of unknown pathology. It consists of wasting of the bones, subcutaneous tissues, and muscles of one-half of the face or head, the muscles suffering but slightly. The accompanying illustration (Fig. 295) shows a case in which there was osseous depression of the cranium and a localized alopecia. The disease is very rare, only about 100 cases having been reported. Of five cases seen by Dana, three were in females and two in males; in all the cases that could be found the origin was between the tenth and twentieth years. It is a chronic
Burr [17.17] contributes an exhaustive paper on hemiatrophy of the tongue with report of a case as follows: "L. B., female, mulatto, thirty-one years old, married, came to the Medico-Chirurgical Hospital, Philadelphia, September 23, 1895, complaining that her `tongue was crooked.' Save that she had had syphilis, her personal history is negative. In February, 1895, she began to suffer from headache, usually behind the left ear, and often preventing sleep. At times there is quite severe vertigo. Several weeks after the onset, headache persisting, she awoke in the night and found the left side of the tongue swollen, black, and painless. For some hours she could neither speak nor chew, but breathing was not interfered with. After a few days all symptoms passed away except headache, and she thought no more of the matter until recently, as stated above, she noticed by accident that her tongue was deformed. She is a spare, poorly-fed, muddy-skinned mulatto girl. The left half of the tongue is only about one-half as large as the right. The upper surface is irregularly depressed and elevated. There are no scars. When protruded it turns sharply to the left. Fibrillary twitching is not present. The mucous membrane is normal. Common sensation and taste are preserved. The pharyngeal reflex is present. The palate moves well. There is no palsy or wasting of the face. The pupils are of normal size and react well to light and with accommodation. Station and gait are normal. There is no incoordination of movement in the arms or legs. The knee-jerks are much increased. There is an attempt at, but no true, clonus; that is, passive flexion of the foot causes two or three jerky movements. There is no glandular swelling or tumor about the jaw or in the neck. Touch and pain-sense are normal in the face and hands, but she complains of numbness in the hands as if she had on tight gloves. There is no trouble in speaking, chewing, or swallowing. There is no pain or rigidity in the neck muscles. Examination of the pharynx reveals no disease of the bones. Under specific treatment the patient improved.''
Astasia-abasia was named by Blocq, who collected 11 cases. According to Knapp, four cases have been reported in America. The disease consists in an inability to stand erect or walk normally, although there is no impairment of sensation, of muscular strength, or of the coordination of other muscles in walking than the lower extremities. In attempting to walk the legs become spasmodic; there are rapid flexions and extensions of the legs on the thighs, and of the thighs on the pelvis. The steps are short, and the feet drag; the body may make great oscillations if the patient stands, walks, or sits, and the head and arms make rhythmical movements; walking
Ménière's disease is a disease probably of the semicircular canals, characterized by nausea, vomiting, vertigo, deafness, tinnitus aurium, and various other phenomena. It is also called aural or auditory vertigo. The salient symptom is vertigo, and this varies somewhat in degree according to the portions of the ear affected. If the disease is in the labyrinth, the patient is supposed to stagger to one side, and the vertigo is paroxysmal, varying to such a degree as to cause simple reeling, or falling as if shot. Gray [17.18] reports the history of a patient with this sensational record: He had been a peasant in Ireland, and one day crossing one of the wide moors in a dog-cart, he was suddenly, as he thought, struck a violent blow from behind, so that he believed that he lost consciousness for some time. At all events, when he was able to get up he found his horse and cart some distance off, and, of course, not a soul in sight. Under the belief that he had been struck by some enemy he went quietly home and said nothing about it. Some time afterward, however, in crossing another lonely place he had a similar experience, and as he came to the conclusion that nobody could have been near him, he made up his mind that it was some malevolent stroke of the devil and he consulted a priest who agreed with him in his belief, and gave him an amulet to wear. A series of similar attacks occurred and puzzled as to whether there was some diabolical agency at work, or whether he was the victim of some conspiracy, he emigrated to America; for several months he had no attacks. A new paroxysm occurring he consulted Gray, who found indubitable evidence of labyrinthine disease. The paroxysms of this disease are usually accompanied by nausea and vomiting, and on account of the paleness of the face, and the cold, clammy perspiration, attacks have frequently been mistaken for apoplexy. In disease of the middle ear the attacks are continuous rather than paroxysmal. If the disease is in the middle or internal ears, loud noises are generally heard, but if the disease is in the external ear, the noises are generally absent, and the vertigo of less degree but continuous. The prognosis varies with the location of the disease, but is always serious.
In a recent discussion before the American Neurological Association Hammond defined merycism as the functions of remastication and rumination in the human subject. He referred to several cases, among them that of the distinguished physiologist, Brown-Séquard, who acquired the habit as a result of experiments performed upon himself. Hammond reported a case of a young man who was the subject of merycism, and whose mental condition was also impaired. No special treatment was undertaken, but the patient was trephined, with the purpose of improving his mental condition. There were no unusual features connected with the operation, but it was noticed that there were no ruminations with the meals he took until the fifth day, when a slight rumination occurred. Eight days later a similar button was removed from the corresponding side of the left skull, and from that time (about six months) to the time of report, there had been no regurgitation. Whether the cure of the merycism in this case was directly due to the operations on the cranium, or the result of the mental improvement, is a question for discussion. Hammond added that, when acquired, merycism was almost invariably the result of over-eating and loading the esophagus, or the result of fast eating.
In remarks upon Hammond's paper Knapp said that two cases had come to his knowledge, both in physicians, but one of them he knew of only by hearsay. The other man, now over thirty, had regurgitated his food from early childhood, and he did not know that he had anything very unusual the matter with him until he began some investigations upon the functions and diseases of the stomach. This man was not nervous, and was certainly not an idiot. He had done active work as a physician, and called himself in perfect health. He was something of an epicure, and never suffered from indigestion. After a hearty meal the regurgitation was more marked. Food had been regurgitated, tasting as good as when first eaten, several hours after the eating. If he attempted to check the regurgitation he sometimes had a slight feeling of
Runge [17.21] discusses three cases of hereditary rumination. These patients belonged to three generations in the male line. The author subjected the contents of the stomach of one patient to quite an extensive analysis, without finding any abnormality of secretion.
Wakefulness.—Generally speaking, the length of time a person can go without sleep is the same as that during which he can survive without food. Persons, particularly those of an hysteric nature, are prone to make statements that they have not slept for many days, or that they never sleep at all, but a careful examination and watch during the night over these patients show that they have at least been in a drowsy, somnolent condition, which is in a measure physiologically equivalent to sleep. Accounts of long periods of wakefulness arise from time to time, but a careful examination would doubtless disprove them. As typical of these accounts, we quote one from Anderson, Indiana, December 11, 1895:—
"David Jones of this city, who attracted the attention of the entire medical profession two years ago by a sleepless spell of ninety-three days, and last year by another spell which extended over one hundred and thirty-one days, is beginning on another which he fears will be more serious than the preceding ones. He was put on the circuit jury three weeks ago, and counting to-day has not slept for twenty days and nights. He eats and talks as well as usual, and is full of business and activity. He does not experience any bad effects whatever from the spell, nor did he during his one hundred and thirty-one days. During that spell he attended to all of his farm business. He says now that he feels as though he never will sleep again. He does not seem to bother himself about the prospects of a long and tedious wake. He cannot attribute it to any one thing, but thinks that it was probably superinduced by his use of tobacco while young.''
Somnambulism, or, as it has been called, noctambulation, is a curious phase of nocturnal cerebration analogous to the hypnotic state, or double consciousness occasionally observed in epileptics. Both Hippocrates and Aristotle discuss somnambulism, and it is said that the physician Galen was a victim
The state of the eyes during somnambulism varies considerably. They are sometimes closed, sometimes half-closed, and frequently quite open; the pupil is sometimes widely dilated, sometimes contracted, sometimes natural, and for the most part insensible to light.
Somnambulism seems to be hereditary. Willis cites an example in which the father and the children were somnambulists, and in other cases several individuals in the same family have been afflicted. Horstius gives a history of three young brothers who became somnambulistic at the same epoch. A remarkable instance of somnambulism [17.22] was the case of a lad of sixteen and a half years who, in an attack of somnambulism, went to the stable, saddled his horse, asked for his whip, and disputed with the toll-keeper about his fare, and when he awoke had no recollection whatever of his acts, having been altogether an hour in his trance.
Marville [17.23] quotes the case of an Italian of thirty, melancholic, and a deep thinker, who was observed one evening in his bed. It was seen that he slept with his eyes open but fixed and immovable. His hands were cold, and his pulse extremely slow. At midnight he brusquely tore the curtains of his bed aside, dressed himself, went to his stable, and mounted a horse. Finding the gate of the court yard closed he opened it with the aid of a large stone. Soon he dismounted, went to a billiard room, and simulated all the movements of one playing. In another room he struck with his empty hands a harpsichord, and finally returned to his bed. He appeared to be irritated when anybody made a noise, but a light placed under his nose was apparently unnoticed. He awoke if his feet were tickled, or if a horn was blown in his ear. Tissot transmits to us the example of a medical student who arose in the night, pursued his studies, and returned to bed without awaking; and there is another record of an ecclesiastic who finished his sermon in his sleep.
Negretti, a sleep-walker, sometimes carried a candle about with him as if to furnish him light in his employment, but when a bottle was substituted he carried it, fancying that he had the candle. Another somnambulist, Castelli, was found by Dr. Sloane translating Italian and French and looking out words in his dictionary. His candle was purposely extinguished, whereupon he immediately began groping about, as if in the dark, and, although other lighted candles were in the room, he did not resume his occupation until he had relighted his candle at the fire. He was insensible to the light of every candle excepting the one upon which his attention was fixed.
Tuke tells of a school-boy who being unable to master a school-problem in geometry retired to bed still thinking of the subject; he was found late at night by his instructor on his knees pointing from spot to spot as though he were at the blackboard. He was so absorbed that he paid no attention to the light of the candle, nor to the speech addressed to him. The next morning the teacher asked him if he had finished his problem, and he replied that he had, having dreamt it and remembered the dream. There are many such stories on record. Quoted by Gray, Mesnet speaks of a suicidal attempt made in his presence by a somnambulistic woman. She made a noose of her apron, fastened one end to a chair and the other to the top of a window. She then kneeled down in prayer, made the sign of the cross, mounted a stool, and tried to hang herself. Mesnet, scientific to the utmost, allowed her to hang as long as he dared, and then stopped the performance. At another time she attempted to kill herself by violently throwing herself on the floor after having failed to fling herself out of the window. At still another time she tried poison, filling a glass with water, putting several coins into it, and hiding it after bidding farewell to her family in writing; the next night, when she was again somnambulistic, she changed her mind once more, writing to her family explaining her change of purpose. Mesnet relates some interesting experiments made upon a French sergeant in a condition of somnambulism, demonstrating the excitation of ideas in the mind through the sense of touch in the extremities. This soldier touched a table, passed his hands over it, and finding nothing on it, opened the drawer, took out a pen, found paper
Yellowlees [17.25] speaks of homicide by a somnambulist. According to a prominent New York paper, one of the most singular and at the same time sad cases of somnambulism occurred a few years ago near Bakersville, N. C. A young man there named Garland had been in the habit of walking in his sleep since childhood. Like most other sleep-walkers when unmolested, his ramblings had been without harm to himself or others. Consequently his wife paid little attention to them. But finally he began to stay away from the house longer than usual and always returned soaking wet. His wife followed
Dreams, nightmare, and night terrors form too extensive a subject and one too well known to be discussed at length here, but it might be well to mention that sometimes dreams are said to be pathognomonic or prodromal of approaching disease. Cerebral hemorrhage has often been preceded by dreams of frightful calamities, and intermittent fever is often announced by persistent and terrifying dreams. Hammond has collected a large number of these prodromic dreams, seeming to indicate that before the recognizable symptoms of disease present themselves a variety of morbid dreams may occur. According to Dana, Albers says: "Frightful dreams are signs of cerebral congestion. Dreams about fire are, in women, signs of impending hemorrhage. Dreams about blood and red objects are signs of inflammatory conditions. Dreams of distorted forms are frequently a sign of abdominal obstruction and diseases of the liver.''
Catalepsy, trance, and lethargy, lasting for days or weeks, are really examples of spontaneously developed mesmeric sleep in hysteric patients or subjects of incipient insanity. If the phenomenon in these cases takes the form of catalepsy there is a waxy-like rigidity of the muscles which will allow the limbs to be placed in various positions, and maintain them so for minutes or even hours. In lethargy or trance-states the patient may be plunged into a deep and prolonged unconsciousness lasting from a few hours to several years. It is in this condition that the lay journals find argument for their stories of premature burial, and from the same source the fabulous "sleeping girls'' of the newspapers arise. Dana says that some persons are in the habit of going into a mesmeric sleep spontaneously. In these states there may be a lowering of bodily temperature, a retarding of the respiration and heart-action, and excessive sluggishness of the action of the bowels. The patients can hear and may respond to suggestions, though apparently insensible to painful impressions, and do not appear to smell, taste, or see; the eyes are closed, turned upward, and the pupils contracted as in normal sleep.
This subject has been investigated by such authorities as Weir Mitchell
Weir Mitchell [17.31] collected 18 cases of protracted sleep, the longest continuing uninterruptedly for six months. Chilton's case lasted seventeen weeks. Six of the 18 cases passed a large part of each day in sleep, one case twenty-one hours, and another twenty-three hours. The patients were below middle life; ten were females, seven males, and one was a child whose sex was not given. Eight of the 18 recovered easily and completely, two recovered with loss of intellect, one fell a victim to apoplexy four months after awakening, one recovered with insomnia as a sequel, and four died in sleep. One recovered suddenly after six months' sleep and began to talk, resuming the train of thought where it had been interrupted by slumber. Mitchell reports a case in an unmarried woman of forty-five. She was a seamstress of dark complexion and never had any previous symptoms. On July 20, 1865, she became seasick in a gale of wind on the Hudson, and this was followed by an occasional loss of sight and by giddiness. Finally, in November she slept from Wednesday night to Monday at noon, and died a few days later. Jones of New Orleans [17.32] relates the case of a girl of twenty-seven who had been asleep for the last eighteen years, only waking at certain intervals, and then remaining awake from seven to ten minutes. The sleep commenced at the age of nine, after repeated large doses of quinin and morphin. Periods of consciousness were regular, waking at 6 A. M. and every hour thereafter until noon, then at 3 P. M., again at sunset, and at 9 P. M., and once or twice before morning. The sleep was deep, and nothing seemed to arouse her. Gairdner [17.33] mentions the case of a woman who, for one hundred and sixty days, remained in a lethargic stupor, being only a mindless automaton. Her life was maintained by means of the stomach tube. The Revue d'Hypnotisme contains the report of a young woman of twenty-five, who was completing the fourth year of an uninterrupted trance. She began May 30, 1883, after a fright, and on the same day, after several convulsive attacks, she fell into a profound sleep, during which she was kept alive by small quantities of liquid food, which she swallowed automatically. The excretions were greatly diminished, and menstruation was suppressed. There is a case reported [17.34] of a Spanish soldier of twenty-two, confined in the Military
Hypnotism.—The phenomenon of hypnotism was doubtless known to the Oriental nations, and even to the Greeks, Romans, and Egyptians, as well as to other nations since the downfall of the Roman Empire. "The fakirs of India, the musicians of Persia, the oracles of Greece, the seers of Rome, the priests and priestesses of Egypt, the monastic recluses of the Middle Ages, the ecstatics of the seventeenth and early part of the eighteenth century exhibited many symptoms that were, and are still, attributed by religious enthusiasts to supernatural agencies, but which are explainable by what we know of hypnotism. The Hesychasts of Mount Athos who remained motionless for days with their gaze directed steadily to the navel; the Taskodrugites who remained statuesque for a long period with the finger applied to the nose; the Jogins who could hibernate at will; the Dandins of India who became cataleptoid by 12,000 repetitions of the sacred word Om;' St. Simeon Stylites who, perched on a lofty pillar, preserved an attitude of saint-like withdrawal from earthly things for days; and even Socrates, of whom it was said that he would stand for hours motionless and wordless—all these are probable instances of autohypnotism.'' (Gray.)
Hypnotism is spoken of as a morbid mental state artificially produced, and characterized by perversion or suspension of consciousness, and abeyance of volition; a condition of suggestibility leads the patient to yield
Hypnosis is spoken of by Huc and Hellwald of the Buddhist convents in Thibet; and Sperling, who has had a particularly wide experience in the field of hypnotism, and whose opinion is of particular value, says that he has seen dervishes in Constantinople who, from the expression of their eyes and their whole appearance, as well as from peculiar postures they maintain for a long time, impressed him as being in a hypnotic state. The state may have been induced by singing and uniform whirling motions. Hildebrandt, Jacolliot, Fischer, Hellwald, and other trustworthy witnesses and authors tell us strange things about the fakirs of India, which set any attempt at explanation on the basis of our present scientific knowledge at defiance—that is, if we decline to accept them as mere juggler's tricks. Hypnotism seems to be the only explanation. It is a well known fact that both wild and domestic beasts can be hypnotized and the success of some of the animal-tamers is due to this fact. In hypnotism we see a probable explanation for the faith-cures which have extended over many centuries, and have their analogy in the supposed therapeutic powers of the Saints.
As to the therapeutic value of hypnotism, with the exception of some minor benefits in hysteric cases and in insomnia, the authors must confess that its use in Medicine seems very limited.
African sleep-sickness is a peculiar disorder, apparently infectious in character, which occurs among the negroes of the western coast of Africa. It has been transported to other regions but is endemic in Africa. According to Dana it begins gradually with malaise and headache. Soon there is drowsiness after meals which increases until the patient is nearly all the time in a stupor. When awake he is dull and apathetic. There is no fever; the temperature may be subnormal. The pulse, too, is not rapid, the skin is dry, the tongue moist but coated, the bowels regular. The eyes become congested and prominent. The cervical glands enlarge. The disease ends in coma and death. Recovery rarely occurs. Sometimes the disease is more violent, and toward the end there are epileptic convulsions and muscular tremors. Autopsies have revealed no pathologic changes.
Recently Forbes [17.35] contributes an interesting paper on the sleeping sickness of Africa. The disease may occur in either sex and at any age, though it is most frequent from the twelfth to the twentieth years, and in the male sex. It begins with enlargement of the cervical glands, and drowsiness and sleep at unusual hours. At first the patient may be aroused, but later sinks into a heavy stupor or coma. Death occurs in from three to twelve months, and is due to starvation. Forbes reports 11 fatal cases, and two that passed from observation. At the autopsy are found hyperemia of the arachnoid, and slight chronic leptomeningitis and pachymeningitis. There is also anemia of the brain-substance. In one of his cases the spleen was enlarged. He was inclined to regard the disease as a neurosis.
Aphasia is a disease of the faculty of language, that is, a disturbance of the processes by which we see, hear, and at the same time appreciate the meaning of symbols. It includes also the faculty of expressing our ideas to others by means of the voice, gesture, writing, etc. The trouble may be central or in the conducting media. The varieties of aphasia are:—
(1) Amnesia of speech.
(2) Amnesia of speech and written language.
(3) Amnesia of speech, written language, and gesture.
In most cases there is no paralysis of the tongue or speech-forming organs. As a rule the intellect is unaffected, the patient has the ideas, but lacks the
What was probably a case of incomplete aphasia is mentioned by Pliny, that of Messala Corvinus who was unable to tell his own name; and many instances of persons forgetting their names are really nothing but cases of temporary or incomplete aphasia. In some cases of incomplete and in nearly all cases of complete aphasia, involuntary sentences are ejaculated. According to Seguin [17.36] a reverend old gentleman affected with amnesia of words was forced to utter after the sentence, "Our Father who art in heaven,'' the words "let Him stay there.'' A lady seen by Trousseau would rise on the coming of a visitor to receive him with a pleased and amiable expression of countenance, and show him to a chair, at the same time addressing to him the words, "cochon, animal, fichue bête,'' French words hardly allowable in drawing-room usage. She was totally aphasic but not paralyzed. Women often use semi-religious expressions like "Oh dear,'' or "Oh Lord.'' Men of the lower classes retain their favorite oaths remarkably. Sometimes the phrases ejaculated are meaningless, as in Broca's celebrated case.
Aphasia may he the result of sudden strong emotions, in such cases being usually temporary; it may be traumatic; it may be the result of either primary or secondary malnutrition or degeneration.
There are some cases on record in which the sudden loss and the sudden return of the voice are quite marvelous.
Habershon [17.37] reports the case of a woman who on seeing one of her children scalded fell unconscious and motionless, and remained without food for three days. It was then found that she suffered from complete aphasia. Five weeks after the incident she could articulate only in a very limited vocabulary.
In the Philosophical Transactions Archdeacon Squire tells of the case of Henry Axford, who lost the power of articulation for four years; after a horrible dream following a debauch he immediately regained his voice, and thereafter he was able to articulate without difficulty.
Ball [17.38] records a curious case of what he calls hysteric aphonia. The patient was a young lady who for several months could neither sing nor speak, but on hearing her sister sing a favorite song, she began to sing herself; but, although she could sing, speech did not return for several weeks. Ball remarks that during sleep such patients may cry out loudly in the natural voice.
Wadham [17.39] reports the case of a boy of eighteen who was admitted to his ward suffering with hemiplegia of the left side. Aphasia developed several days after admission and continued complete for three months. The boy
Ogle [17.42] quotes six cases of loss of speech after bites of venomous snakes. Two of the patients recovered. According to Russ [17.43] this strange symptom is sometimes instantaneous and in other instances it only appears after an interval of several hours. In those who survive the effects of the venom it lasts for an indefinite period. One man seen by Russ had not only lost his speech in consequence of the bite of a fer-de-lance snake, but had become, and still remained, hemiplegic. In the rest of Russ's cases speech alone was abolished. Russ remarks that the intelligence was altogether intact, and sensibility and power of motion were unaffected. One woman who had been thus condemned to silence, suddenly under the influence of a strong excitement recovered her speech, but when the emotion passed away speech again left her. Ogle accounts for this peculiar manifestation of aphasia by supposing that the poison produces spasm of the middle cerebral arteries, and when the symptom remains a permanent defect the continuance of the aphasia is probably due to thrombosis of arteries above the temporary constriction.
Anosmia, or loss of smell, is the most common disorder of olfaction; it may be caused by cortical lesions, olfactory nerve-changes, congenital absence, or over-stimulation of the nerves, or it may be a symptom of hysteria.
Ogle, [17.44] after mentioning several cases of traumatic anosmia, suggests that a blow on the occiput is generally the cause. Legg [17.45] reports a confirmatory case, but of six cases mentioned by Notta [17.46] two were caused by a blow on the crown of the head, and two on the right ear. The prognosis in traumatic anosmia is generally bad, although there is a record [17.47] of a man who fell while working on a wharf, striking his head and producing anosmia with partial loss of hearing and sight, and who for several weeks neither smelt nor tasted, but gradually recovered.
Anosmia has been noticed in leukoderma and allied disturbances of pigmentation. Ogle [17.49] mentions a negro boy in Kentucky whose sense of smell decreased as the leukoderma extended. Influenza, causing adhesions of the posterior pillars of the fauces, has given rise to anosmia.
Occasionally overstimulation of the olfactory system may lead to anosmia. Graves [17.50] mentions a captain of the yeomanry corps who while investigating the report that 500 pikes were concealed at the bottom of a cesspool in one of the city markets superintended the emptying of the cesspool, at the bottom of which the arms were found. He suffered greatly from the abominable effluvia, and for thirty-six years afterward he remained completely deprived of the sense of smell.
In a discussion upon anosmia before the Medico-Chirurgical Association of London, January 25, 1870, there was an anosmic patient mentioned who was very fond of the bouquet of moselle, and Carter mentioned that he knew a man who had lost both the senses of taste and smell, but who claimed that he enjoyed putrescent meat. Leared spoke of a case in an epileptic affected with loss of taste and smell, and whose paroxysms were always preceded by an odor of peach-blossoms.
Hyperosmia is an increase in the perception of smell, which rarely occurs in persons other than the hysteric and insane. It may be cultivated as a compensatory process, as in the blind, or those engaged in particular pursuits, such as tea-tasting. Parosmia is a rare condition, most often a symptom of hysteria or neurasthenia, in which everything smells of a similar, peculiar, offensive odor. Hallucinations of odor are sometimes noticed in the insane. They form most obstinate cases, when the hallucination gives rise to imaginary disagreeable, personal odors.
Perversion of the tactile sense, or wrong reference to the sensation of pain, has occasionally been noticed. The Ephemerides records a case in which there was the sense of two objects from a single touch on the hypochondrium. Weir Mitchell [17.51] remarks that soldiers often misplace the location of pain after injuries in battle. He also mentions several cases of wrong reference of the sensation of pain. These instances cannot be called reflex disturbances, and are most interesting. In one case the patient felt the pain from a urethral injection in gonorrhea, on the top of the head. In another an individual let an omnibus-window fall on his finger, causing but brief pain in the finger, but violent pains in the face and neck of that side. Mitchell
Nostalgia is the name generally given to that variety of melancholia in which there is an intense longing for home or country. This subject has apparently been overlooked in recent years, but in the olden times it was extensively discussed. Swinger, Harderus, Tackius, Guerbois, Hueber, Therrin, Castellanau, Pauquet, and others have written extensively upon this theme. It is said that the inhabitants of cold countries, such as the Laplanders and the Danes, are the most susceptible to this malady. For a long time many writers spoke of the frequency and intensity of nostalgia among the Swiss. Numerous cases of suicide from this affliction have been noticed among these hardy mountaineers, particularly on hearing the mountain-song of their homes, "Ranz des vaches.'' This statement, which is an established fact, is possibly due to the social constitution of the Swiss mountaineers, who are brought up to a solitary home life, and who universally exhibit great attachment to and dependence upon their parents and immediate family. In the European armies nostalgia has always been a factor in mortality. In the Army of the Moselle, and in Napoleon's Alpine Army, the terrible ravages of suicide among the young Bretons affected with nostalgia have been recorded; it is among the French people that most of the investigation on this subject has been done. Moreau speaks of a young soldier in a foreign country and army who fell into a most profound melancholy when, by accident, he heard his native tongue. According to Swinger and Sauvages women are less subject to nostalgia than men. Nostalgia has been frequently recorded in hospital wards. Percy and Laurent [17.52] have discussed this subject very thoroughly, and cite several interesting cases among emigrants, soldiers, marines, etc. Hamilton [17.53] speaks of a recruit who became prostrated by longing for his home in Wales. He continually raved, but recovered from his delirium when assured by the hospital authorities of his forthcoming furlough. Taylor [17.54] records two cases of fatal nostalgia. One of the victims was a Union refugee who went to Kentucky from his home in Tennessee. He died talking about and pining for his home. The second patient was a member of a regiment of colored infantry; he died after repeatedly pining for his old home.
Animals are sometimes subject to nostalgia, and instances are on record in which purchasers have been compelled to return them to the old home on account of their literal home-sickness. Oswald tells of a bear who, in the presence of food, committed suicide by starvation.
Hypochondria consists of a mild form of insanity in which there is a tendency to exaggerate the various sensations of the body and their importance, their exaggeration being at times so great as to amount to actual
Morbid fears or impulses, called by the Germans Zwangsvorstellungen, or Zwangshandlungen, and by the French, peurs maladies, have only been quite recently studied, and form most interesting cases of minor insanity. Gelineau *[370] has made extensive investigations in this subject, and free reference has been made to his work in the preparation of the following material.
Aichmophobia is a name given by the French to the fear of the sight of any sharp-pointed instrument, such as a pin, needle, fish-spine, or naked sword. An illustrious sufferer of this 'phobia was James I. of England, who could never tolerate the appearance of a drawn sword. Gélineau reports an interesting case of a female who contracted this malady after the fatigue of lactation of two children. She could not tolerate knives, forks, or any pointed instruments on the table, and was apparently rendered helpless in needle-work on account of her inability to look at the pointed needle.
Agoraphobia is dread of an open space, and is sometimes called Kenophobia. The celebrated philosopher Pascal was supposed to have been affected with this fear. In agoraphobia the patient dreads to go across a street or into a field, is seized with an intense feeling of fright, and has to run to a wall or fall down, being quite unable to proceed. There is violent palpitation, and a feeling of constriction is experienced. According to Suckling, pallor and profuse perspiration are usually present, but there is no vertigo, confusion of mind, or loss of consciousness. The patient is quite conscious of the foolishness of the fears, but is unable to overcome them. The will is in abeyance and is quite subservient to the violent emotional disturbances. Gray mentions a patient who could not go over the Brooklyn Bridge or indeed over any bridge without terror. Roussel speaks of a married woman who had never had any children, and who was apparently healthy, but who for the past six months had not been able to put her head out of the window or go upon a balcony. When she descended into the street she was unable to traverse the open spaces. Chazarin mentions a case in a woman of fifty, without any other apparent symptom of diathesis. Gélineau *[370] quotes a case of agoraphobia, secondary to rheumatism, in a woman of thirty-nine. There is a corresponding fear of high places often noticed, called acrophobia; so that many people dare not trust themselves on high buildings or other eminences.
Thalassophobia is the fear of the view of immense spaces or uninterrupted expanses. The Emperor Heraclius, at the age of fifty-nine, had an insurmountable fear of the view of the sea; and it is said that when he crossed the Bosphorus a bridge of boats was formed, garnished on both sides with plants and trees, obscuring all view of the water over which the Emperor peacefully traversed on horseback. The moralist Nicole, was equally a thalassophobe, and always had to close his eyes at the sight of a large sheet
Claustrophobia is the antithesis of agoraphobia. Raggi [17.55] describes a case of such a mental condition in a patient who could not endure being within an enclosure or small space. Suckling [17.56] mentions a patient of fifty-six who suffered from palpitation when shut in a railway carriage or in a small room. She could only travel by rail or go into a small room so long as the doors were not locked, and on the railroad she had to bribe the guard to leave the doors unlocked. The attacks were purely mental, for the woman could be deceived into believing that the door to a railroad carriage was unlocked, and then the attack would immediately subside. Suckling also mentions a young woman brought to him at Queen's Hospital who had a great fear of death on getting into a tram car, and was seized with palpitation and trembling on merely seeing the car. This patient had been in an asylum. The case was possibly due more to fear of an accident than to true claustrophobia. Gorodoichze [17.57] mentions a case of claustrophobia in a woman of thirty-eight, in whose family there was a history of hereditary insanity. Ball [17.58] speaks of a case in a woman who was overcome with terror half way in the ascension of the Tour Saint-Jacques, when she believed the door below was closed. Gélineau quotes the case of a brave young soldier who was believed to be afraid of nothing, but who was unable to sleep in a room of which the door was closed.
Astrophobia or astropaphobia is a morbid fear of being struck by lightning. It was first recognized by Bruck of Westphalia, who knew a priest who was always in terror when on a country road with an unobstructed view of the sky, but who was reassured when he was under the shelter of trees. He was advised by an old physician always to use an umbrella to obstruct his view of the heavens, and in this way his journeys were made tranquil. Beard knew an old woman who had suffered all her life from astrophobia. Her grandmother had presented the same susceptibility and the same fears. Sometimes she could tell the approach of a storm by her nervous symptoms. Caligula, Augustus, Henry III., and other celebrated personages, were overcome with fear during a storm.
Mysophobia is a mild form of insanity characterized by a dread of the contact of dirt. It was named by Hammond, whose patient washed her hands innumerable times a day, so great was the fear of contamination. These patients make the closest inspection of their toilet, their eating and drinking utensils, and all their lives are intensely worried by fear of dirt.
Hematophobia is a horror of blood, which seems to be an instinctive sentiment in civilized man, but which is unknown among savages. When
Necrophobia and thanatophobia are allied maladies, one being the fear of dead bodies and the other the fear of death itself.
Anthropophobia is a symptom of mental disease consisting in fear of society. Beard, Mitchell, Baillarger, and others have made observations on this disease. The antithesis of this disease is called monophobia. Patients are not able to remain by themselves for even the shortest length of time. This morbid dread of being alone is sometimes so great that even the presence of an infant is an alleviation. Gélineau cites an instance in a man of forty-five which was complicated with agoraphobia.
Bacillophobia is the result of abnormal pondering over bacteriology. Huchard's case was in a woman of thirty-eight who, out of curiosity, had secretly read the works of Pasteur, and who seemed to take particular pleasure in conning over the causes of death in the health-reports. Goyard mentions an instance in a Swiss veterinary surgeon.
Kleptophobia, examples of which have been cited by Cullère, [17.59] is the fear of stealing objects in view, and is often the prelude of kleptomania. The latter disease has gained notoriety in this country, and nearly every large store has agents to watch the apparently growing number of kleptomaniacs. These unfortunate persons, not seldom from the highest classes of society, are unable to combat an intense desire to purloin articles. Legal proceedings have been instituted against many, and specialists have been called into court to speak on this question. Relatives and friends have been known to notify the large stores of the thieving propensities of such patients.
Le Grande du Saulle has given to the disease in which there is a morbid doubt about everything done, the name folie de doute. Gray mentions a case in a patient who would go out of a door, close it, and then come back, uncertain as to whether he had closed it, close it again, go off a little way, again feel uncertain as to whether he had closed it properly, go back again, and so on for many times. Hammond relates the history of a case in an intelligent man who in undressing for bed would spend an hour or two determining whether he should first take off his coat or his shoes. In the morning he would sit for an hour with his stockings in his hands, unable to determine which he should put on first.
Syphilophobia is morbid fear of syphilis. Lyssophobia is a fear of hydrophobia which sometimes assumes all the symptoms of the major disease, and even produces death. Gélineau, Colin, Berillon, and others have studied cases. In Berillon's case the patient was an artist, a woman of brunet complexion, who for six years had been tormented with the fear of becoming mad, and in whom the symptoms became so intense as to constitute
Spermatophobia has been noticed among the ignorant, caused or increased by inspection of sensational literature, treatises on the subject of spermatorrhea, etc. Ferré mentions a woman of thirty-six, of intense religious scruples, who was married at eighteen, and lost her husband six years afterward. She had a proposition of marriage which she refused, and was prostrated by the humid touch of the proposer who had kissed her hand, imagining that the humidity was due to semen. She was several times overcome by contact with men in public conveyances, her fear of contamination being so great. Zoophobia, or dread of certain animals, has been mentioned under another chapter under the head of idiosyncrasies. Pantophobia is a general state of fear of everything and everybody. Phobophobia, the fear of being afraid, is another coinage of the wordmakers. The minor 'phobias, such as pyrophobia, or fear of fire; stasophobia, or inability to arise and walk, the victims spending all their time in bed; toxicophobia or fear of poison, etc., will be left to the reader's inspection in special works on this subject.
Demonomania is a form of madness in which a person imagines himself possessed of the devil. Ancient records of this disease are frequent, and in this century Lapointe [17.60] reports the history of demonomania in father, mother, three sons, and two daughters, the whole family, with the exception of one son, who was a soldier, being attacked. They imagined themselves poisoned by a sorceress, saw devils, and had all sorts of hallucinations, which necessitated the confinement of the whole family in an asylum for over a month. They continued free from the hallucinations for two years, when first the mother, and then gradually all the other members of the family, again became afflicted with demonomania and were again sent to the asylum, when, after a residence therein of five months, they were all sufficiently cured to return home.
Particular aversions may be temporary only, that is, due to an existing condition of the organism, which, though morbid, is of a transitory character. Such, for instance, are those due to dentition, the commencement or cessation of the menstrual function, pregnancy, etc. These cases are frequently of a serious character, and may lead to derangement of the mind. Millington relates the history of a lady who, at the beginning of her first pregnancy, acquired an overpowering aversion to a half-breed Indian woman who was employed in the house as a servant. Whenever this woman came near her she was at once seized with violent trembling; this ended in a few minutes with vomiting and great mental and physical prostration lasting several hours. Her husband would have sent the woman away, but Mrs. X insisted on her remaining, as she was a good servant, in order that she might overcome what she regarded as an unreasonable prejudice. The effort was, however, too
Circular or periodic insanity is a rare psychosis. According to Drewry reports of very few cases have appeared in the medical journals. "Some systematic writers,'' says Drewry, "regard it as a mere subdivision of periodic insanity (Spitzka). A distinguished alienist and author of Scotland however has given us an admirable lecture on the subject. He says: `I have had under my care altogether about 40 cases of typical folie circulaire.' In the asylum at Morningside there were, says Dr. Clouston, in 800 patients 16 cases of this peculiar form of mental disease. Dr. Spitzka, who was the first American to describe it, found in 2300 cases of pauper insane four per cent. to be periodic, and its sub-group, circular, insanity. Dr. Stearns states that less than one-fourth of one per cent. of cases in the Hartford (Conn.) Retreat classed as mania and melancholia have proved to be folie circulaire. Upon examination of the annual reports of the superintendents of hospitals for the insane in this country, in only a few are references made to this as a distinct form of insanity. In the New York State hospitals there is a regular uniform classification of mental diseases in which `circular (alternating) insanity' occupies a place. In the report of the Buffalo Hospital for 1892, in statistical table No. 4, `showing forms of insanity in those admitted, etc., since 1888,' out of 1428 cases, only one was `alternating (circular) insanity.' In the St. Lawrence Hospital only one case in 992 was credited to this special class. In the institution in Philadelphia, of which Dr. Chapin is the superintendent, 10,379 patients have been treated, only three of whom were diagnosed cases of manie circulaire. Of the 900 cases of insanity in the State Hospital at Danville, Pa., less than four per cent. were put in this special class. There are in the Central (Va.) State Hospital (which is exclusively for the colored insane) 775 patients, three of whom are genuine cases of circular insanity, but they are included in `periodic insanity.' This same custom evidently prevails in many of the other hospitals for the insane.''
Drewry [17.61] reports three cases of circular insanity, one of which was as follows:—
"William F., a negro, thirty-six years old, of fair education, steady, sober habits, was seized with gloomy depression a few weeks prior to his
Katatonia, according to Gray, is a cerebral disease of cyclic symptoms, ranging in succession from primary melancholia to mania, confusion, and dementia, one or more of these stages being occasionally absent, while convulsive and epileptoid symptoms accompany the mental changes.
It is manifestly impossible to enter into the manifold forms and instances of insanity in this volume, but there is one case, seldom quoted, which may be of interest. It appeared under the title, "A Modern Pygmalion.'' [17.62] It recorded a history of a man named Justin, who died in the Bicêtre Insane
An interesting condition, which has been studied more in France than elsewhere, is double consciousness, dual personality, or, as it is called by the Germans, Doppelwahrnehmungen. In these peculiar cases an individual at different times seems to lead absolutely different existences. The idea from a moralist's view is inculcated in Stevenson's "Dr. Jekyl and Mr. Hyde.'' In an article on this subject [17.63] Weir Mitchell illustrated his paper by examples, two of which will be quoted. The first was the case of Mary Reynolds who, when eighteen years of age, became subject to hysteric attacks, and on one occasion she continued blind and deaf for a period of five or six weeks. Her hearing returned suddenly, and her sight gradually. About three months afterward she was discovered in a profound sleep. Her memory had fled, and she was apparently a new-born individual. When she awoke it became apparent that she had totally forgotten her previous existence, her parents, her country, and the house where she lived. She might be compared to an immature child. It was necessary to recommence her education. She was taught to write, and wrote from right to left, as in the Semitic languages. She had only five or six words at her command—mere reflexes of articulation which were to her devoid of meaning. The labor of re-education, conducted methodically, lasted from seven to eight weeks. Her character had experienced as great a change as her memory; timid to excess in the first state, she became gay, unreserved, boisterous, daring, even to rashness. She strolled through the woods and the mountains, attracted by the dangers of the wild country in which she lived. Then she had a fresh attack of sleep, and returned to her first condition; she recalled all the memories and again assumed a melancholy character, which seemed to be aggravated. No conscious memory of the second state existed. A new attack brought back the second state, with the phenomenon of consciousness which accompanied it the first time. The patient passed successively a great many times from one of these states to the other. These repeated changes stretched over a period of sixteen years. At the end of that time the variations ceased. The patient was then thirty-six years of age; she lived in a mixed state, but more closely resembling the second than the first; her
The second case was that of an itinerant Methodist minister named Bourne, living in Rhode Island, who one day left his home and found himself, or rather his second self, in Norristown, Pennsylvania. Having a little money, he bought a small stock in trade, and instead of being a minister of the gospel under the Methodist persuasion, he kept a candy shop under the name of A. J. Brown, paid his rent regularly, and acted like other people. At last, in the middle of the night, he awoke to his former consciousness, and finding himself in a strange place, supposed he had made a mistake and might be taken for a burglar. He was found in a state of great alarm by his neighbors, to whom he stated that he was a minister, and that his home was in Rhode Island. His friends were sent for and recognized him, and he returned to his home after an absence of two years of absolutely foreign existence. A most careful investigation of the case was made on behalf of the London Society for Psychical Research.
An exhaustive paper on this subject, written by Richard Hodgson in the proceedings of the Society for Psychical Research, states that Mr. Bourne had in early life shown a tendency to abnormal psychic conditions; but he had never before engaged in trade, and nothing could be remembered which would explain why he had assumed the name A. J. Brown, under which he did business. He had, however, been hypnotized when young and made to assume various characters on the stage, and it is possible that the name A. J. Brown was then suggested to him, the name resting in his memory, to be revived and resumed when he again went into a hypnotic trance.
Alfred Binet describes a case somewhat similar to that of Mary Reynolds: "Felida, a seamstress, from 1858 up to the present time (she is still living) has been under the care of a physician named Azam in Bordeaux. Her normal, or at least her usual, disposition when he first met her was one of melancholy and disinclination to talk, conjoined with eagerness for work. Nevertheless her actions and her answers to all questions were found to be perfectly rational. Almost every day she passed into a second state. Suddenly and without the slightest premonition save a violent pain in the temples she would fall into a profound slumber-like languor, from which she would awake in a few moments a totally different being. She was now as gay and cheery as she had formerly been morose. Her imagination was over-excited. Instead of being indifferent to everything, she had become alive to excess. In this state she remembered everything that had happened in the other similar states that had preceded it, and also during her normal life. But when at the end of an hour or two the languor reappeared, and she returned to her normal melancholy state, she could not recall anything that had happened in her second, or joyous, stage. One day, just after passing into the second stage, she attended the funeral of an acquaintance. Returning
Jackson [17.64] reports the history of the case of a young dry-goods clerk who was seized with convulsions of a violent nature during which he became unconscious. In the course of twenty-four hours his convulsions abated, and about the third day he imagined himself in New York paying court to a lady, and having a rival for her favors; an imaginary quarrel and duel ensued. For a half-hour on each of three days he would start exactly where he had left off on the previous day. His eyes were open and to all appearances he was awake during this peculiar delirium. When asked what he had been doing he would assert that he had been asleep. His language assumed a refinement above his ordinary discourse. In proportion as his nervous system became composed, and his strength improved, this unnatural manifestation of consciousness disappeared, and he ultimately regained his health.
A further example of this psychologic phenomenon was furnished quite meetly at a meeting of the Clinical Society of London, where a well known physician exhibited a girl of twelve, belonging to a family of good standing, who displayed in the most complete and indubitable form this condition of dual existence. A description of the case is as follows:—
"Last year, after a severe illness which was diagnosed to be meningitis, she became subject to temporary attacks of unconsciousness, on awakening from which she appeared in an entirely different character. In her normal condition she could read and write and speak fluently, and with comparative correctness. In the altered mental condition following the attack she loses all memory for ordinary events, though she can recall things that have taken place during previous attacks. So complete is this alteration of memory, that at first she was unable to remember her own name or to identify herself or her parents. By patient training in the abnormal condition she has
Proust [17.65] tells a story of a Parisian barrister of thirty-three. His father was a heavy drinker, his mother subject to nervous attacks, his younger brother mentally deficient, and the patient himself was very impressionable. It was said that a judge in a court, by fixing his gaze on him, could send him into an abnormal state. On one occasion, while looking into a mirror in a café, he suddenly fell into a sleep, and was taken to the Charité where he was awakened. He suffered occasional loss of memory for considerable lengths of time, and underwent a change of personality during these times. Though wide awake in such conditions he could remember nothing of his past life, and when returned to his original state he could remember nothing that occurred during his secondary state, having virtually two distinct memories. On September 23, 1888, he quarreled with his stepfather in Paris and became his second self for three weeks. He found himself in a village 100 miles from Paris, remembering nothing about his journey thereto; but on inquiry he found that he had paid a visit to the priest of the village who thought his conduct odd, and he had previously stayed with an uncle, a bishop, in whose house he had broken furniture, torn up letters, and had even had sentence passed upon him by a police court for misdemeanor. During these three weeks he had spent the equivalent of $100, but he could not recall a single item of expenditure. Davies [17.66] cites a remarkable case of sudden loss of memory in a man who, while on his way to Australia, was found by the police in an exhausted condition and who was confined in the Kent County Insane Asylum. He suffered absolute loss of all memory with the exception of the names of two men not close acquaintances, both of whom failed to recognize him in his changed condition in confinement. Four months later his memory returned and his identity was established.
A young man named Spencer, an inmate of the Philadelphia Hospital, was exhibited before the American Neurological Society in June, 1896, as an example of dual personality. At the time of writing he is and has been in apparently perfect health, with no evidence of having been in any other condition. His faculties seem perfect, his education manifests itself in his intelligent performance of the cleric duties assigned to him at the hospital, yet the thread of continuous recollection which connects the present moment with its predecessors—consciousness and memory—has evidently been snapped at some point of time prior to March 3d and after January 19th, the last date at which he wrote to his parents, and as if in a dream, he is now living another life. The hospital staff generally believe that the man is not "shamming,'' as many circumstances seem to preclude that theory. His memory is perfect as to everything back to March 3d. The theory of hypnotism was advanced in explanation of this case.
The morbid sympathy of twin brothers, illustrated in Dumas's "Corsican Brothers,'' has been discussed by Sedgwick, Elliotson, Trousseau, Laycock, Cagentre, and others. Marshall Hall relates what would seem to verify the Corsican myth, the history of twin brothers nine months of age, who always became simultaneously affected with restlessness, whooping and crowing in breathing three weeks previous to simultaneous convulsions, etc. Rush [17.67] describes a case of twin brothers dwelling in entirely different places, who had the same impulse at the same time, and who eventually committed suicide synchronously. Baunir [17.68] describes a similar development of suicidal tendency in twin brothers. A peculiar case of this kind was that of the twin brothers Laustand who were nurses in a hospital at Bordeaux; they invariably became ill at the same time, and suffered cataract of the lens together. [17.69]
Automatism has been noticed as a sequel to cranial injuries, and Huxley quotes a remarkable case reported by Mesnet. [17.70] The patient was a young man whose parietal bone was partially destroyed by a ball. He exhibited signs of hemiplegia on the right side, but these soon disappeared and he became subject to periodic attacks lasting from twenty-four to forty-eight
It is particularly in hypnotic subjects that manifestations of automatism are most marked. At the suggestion of battle an imaginary struggle at once begins, or if some person present is suggested as an enemy the fight is continued, the hypnotic taking care not to strike the person in question. Moll conceded that this looked like simulation, but repetition of such experiments forced him to conclude that these were real, typical hypnoses, in which, in spite of the sense-delusions, there was a dim, dreamy consciousness existing, which influenced the actions of the subject, and which prevented him from striking at a human being, although hitting at an imaginary object. Many may regard this behavior of hypnotics as pure automatism; and Moll adds that, as when walking in the street while reading we automatically avoid knocking passers-by, so the hypnotic avoids hitting another person, although he is dimly or not at all aware of his existence.
Gibbs [17.71] reports a curious case of lack of integrity of the will in a man of fifty-five. When he had once started on a certain labor he seemed to have no power to stop the muscular exercise that the task called forth. If he went to the barn to throw down a forkful of hay, he would never stop until the hay was exhausted or someone came to his rescue. If sent to the wood-pile for a handful of wood, he would continue to bring in wood until the pile was exhausted or the room was full. On all occasions his automatic movements could only be stopped by force.
At a meeting in Breslau Meschede [17.72] rendered an account of a man who suffered from simple misdirection of movement without any mental derangement. If from his own desire, or by direction of others, he wanted to attempt any muscular movement, his muscles performed the exact opposite to his inclinations. If he desired to look to the right, his eyes involuntarily moved to the left. In this case the movement was not involuntary, as the
Presentiment, or divination of approaching death, appearing to be a hypothetic allegation, has been established as a strong factor in the production of a fatal issue in many cases in which there was every hope for a recovery. In fact several physicians have mentioned with dread the peculiar obstinacy of such presentiment. Hippocrates, Romanus, Moller, Richter, Jordani, and other older writers speak of it. Montgomery [17.73] reports a remarkable case of a woman suffering from carcinoma of the uterus. He saw her on October 6, 1847, when she told him she had a strong presentiment of death on October 28th. She stated that she had been born on that day, her first husband had died on October 28th, and she had married her second husband on that day. On October 27th her pulse began to fail, she fell into a state of extreme prostration, and at noon on the 28th she died. In substantiation of the possibility of the influence of presentiment Montgomery cites another case in which he was called at an early hour to visit a lady, the mother of several children. He found her apparently much agitated and distressed, and in great nervous excitement over a dream she had had, in which she saw a handsome monument erected by some children to their mother. She had awakened and became dreadfully apprehensive, she could not tell as to what. The uneasiness and depression continued, her pulse continued to grow weak, and she died at twelve that night without a struggle. Andrews [17.74] has made several observations on this subject, and concludes that presentiment of death is a dangerous symptom, and one which should never be overlooked. One of his cases was in a man with a fractured leg in the Mercy Hospital at Pittsburg. The patient was in good health, but one day he became possessed of a cool, quiet, and perfectly clear impression that he was about to die. Struck with his conviction, Andrews examined his pulse and general condition minutely, and assured the patient there was not the slightest ground for apprehension. But he persisted, and was attacked by pneumonia three days later which brought him to the verge of the grave, although he ultimately recovered. In another instance a young man of ruddy complexion and apparent good health, after an operation for varicocele, had a very clear impression that he would die. Careful examination showed no reason for apprehension. After five or six days of encouragement and assurance, he appeared to be convinced that his reasoning was foolish, and he gave up the idea of death. About the ninth day the wound presented a healthy, rosy appearance, and as the patient was cheerful he was allowed to leave his bed. After a few hours the nurse heard the noise of labored breathing, and on investigation found the patient apparently in a dying condition. He was given stimulants and regained consciousness, but again relapsed, and died in a few moments. At the necropsy the heart was found healthy, but there were two or three spots of
| CHAPTER XVII.
ANOMALOUS NERVOUS AND MENTAL DISEASES. Anomalies and Curiosities of Medicine | ||