| CHAPTER XI.
SURGICAL ANOMALIES OF THE EXTREMITIES. Anomalies and Curiosities of Medicine | ||
11. CHAPTER XI.
SURGICAL ANOMALIES OF THE EXTREMITIES.
Reunion of Digits.—An interesting phenomenon noticed in relation to severed digits is their wonderful capacity for reunion. Restitution of a severed part, particularly if one of considerable function, naturally excited the interest of the older writers. Locher [11.1] has cited an instance of avulsion of the finger with restitution of the avulsed portion; and Brulet, [11.2] Van Esh, Farmer, *[338] Ponteau, Regnault, and Rosenberg cite instances of reunion of a digit after amputation or severance. Eve's "Remarkable Cases in Surgery'' contains many instances of reunion of both fingers and thumbs, and in more recent years several other similar cases have been reported. [11.3] At the Emergency Hospital in Washington, D. C., there was a boy brought in who had completely severed one of his digits by a sharp bread-cutter. The amputated finger was wrapped up in a piece of brown paper, and, being apparently healthy and the wound absolutely clean, it was fixed in the normal position on the stump, and covered by a bichlorid dressing. In a short time complete function was restored. In this instance no joint was involved, the amputation being in the middle of the 2d phalanx. Staton [11.4] has described a case in which the hand was severed from the arm by an accidental blow from an axe. The wound extended from the styloid process directly across to the trapezium, dividing all the muscles and blood-vessels, cutting through bones. A small portion of the skin below the articulation, with the ulna, remained intact. After an unavoidable delay of an hour, Staton proceeded to replace the hand with silver sutures, adhesive plaster, and splints. On the third day pulsation was plainly felt in the hand, and on the fourteenth day the sutures were removed. After some time the patient was able to extend the fingers of the wounded member, and finally to grasp with all her wonted strength.
The reproduction or accidental production of nails after the original part has been torn away by violence or destroyed by disease, is quite interesting. Sometimes when the whole last phalanx has been removed, the nail regrows at the tip of the remaining stump. Tulpius *[842] seems to have met with this remarkable condition. Maréchal de Rougères, [11.5] Voigtel, and Ormançey [11.6] have related instances of similar growths on the 2d phalanx
In some instances avulsion of a finger is effected in a peculiar manner. In 1886 Anche reported to his confrères in Bordeaux a rare accident of this nature that occurred to a carpenter. The man's finger was caught between a rope and the block of a pulley. By a sudden and violent movement on his part he disengaged the hand but left the 3d finger attached to the pulley. At first examination the wound looked like that of an ordinary amputation by the usual oval incision; from the center of the wound the proximal fragment of the 1st phalanx projected. Polaillon [11.8] has collected 42 similar instances, in none of which, however, was the severance complete.
It occasionally happens that in avulsion of the finger an entire tendon is stripped up and torn off with the detached member. Vogel [11.9] describes an instance of this nature, in which the long flexor of the thumb was torn off with that digit. In the Surgical Museum at Edinburgh there is preserved a thumb and part of the flexor longus pollicis attached, which were avulsed simultaneously. Nunnely [11.10] has seen the little finger together with the tendon and body of the longer flexor muscle avulsed by machinery. Stone [11.11] details the description of the case of a boy named Lowry, whose left thumb was caught between rapidly twisting strands of a rope, and the last phalanx, the neighboring soft parts, and also the entire tendon of the flexor longus pollicis were instantly torn away. There was included even the tendinous portion of that small slip of muscle taking its origin from the anterior aspect of the head and upper portion of the ulna, and which is so delicate and insignificant as to
Pinkerton [11.12] describes a carter of thirty-one who was bitten on the thumb by a donkey. The man pulled violently in one direction, and the donkey, who had seized the thumb firmly with his teeth, pulled forcibly in the other direction until the tissues gave way and the man ran off, leaving his thumb in the donkey's mouth. The animal at once dropped the thumb, and it was picked up by a companion who accompanied the man to the hospital. On examination the detached portion was found to include the terminal phalanx of the thumb, together with the tendon of the flexor longus pollicis measuring ten inches, about half of which length had a fringe of muscular tissue hanging from the free borders, indicating the extent and the penniform arrangement of the fibers attached to it. Meyer [11.13] cites a case in which the index finger was torn off and the flexor muscle twisted from its origin. The authors know of an unreported case in which a man running in the street touched his hand to a hitching block he was passing; a ring on one of his fingers caught in the hook of the block, and tore off the finger with the attached tendon and muscle. There is a similar instance of a Scotch gentleman who slipped, and, to prevent falling, he put out his hand to catch the railing. A ring on one of his fingers became entangled in the railing and the force of the fall tore off the soft parts of the finger together with the ring.
The older writers mentioned as a curious fact that avulsion of the arm, unaccompanied by hemorrhage, had been noticed. Belchier, *[629] Carmichael, *[594] and Clough [11.14] report instances of this nature, and, in the latter case, the progress of healing was unaccompanied by any uncomfortable symptoms. In the last century Hunezoysky observed complete avulsion of the arm by a cannon-ball, without the slightest hemorrhage. The Ephemerides contains an account of the avulsion of the hand without any bleeding, and Woolcomb [11.15] has observed a huge wound of the arm from which hemorrhage was similarly absent. Later observations have shown that in this accident absence of hemorrhage is the rule and not the exception. The wound is generally lacerated and contused and the mouths of the vessels do not gape, but are twisted and crushed. The skin usually separates at the highest point and the muscles protrude, appearing to be tightly embraced and almost strangulated by the skin, and also by the tendons, vessels, and nerves which, crushed and twisted with the fragments of bone, form a conical stump. Cheselden reports the history of a case, which has since become classic, that he observed in St. Thomas' Hospital in London, in 1837. A miller had carelessly thrown a slip-knot of rope about his wrist, which became caught in a revolving cog, drawing him from the ground and violently throwing his body against a beam. The force exerted by the cog drawing on the rope was sufficient to avulse his whole arm and shoulder-blade. There was comparatively little hemorrhage
According to Billroth the avulsion of an arm is usually followed by fatal shock. Fischer, however, relates the case of a lion-tamer whose whole left arm was torn from the shoulder by a lion; the loss of blood being very slight and the patient so little affected by shock that he was able to walk to the hospital.
Mussey [11.16] describes a boy of sixteen who had his left arm and shoulder-blade completely torn from his body by machinery. The patient became so involved in the bands that his body was securely fastened to a drum, while his legs hung dangling. In this position he made about 15 revolutions around the drum before the motion of the machinery could be effectually stopped by cutting off the water to the great wheel. When he was disentangled from the bands and taken down from the drum a huge wound was seen at the shoulder, but there was not more than a pint of blood lost. The collarbone projected from the wound about half an inch, and hanging from the wound were two large nerves (probably the median and ulnar) more than 20 inches long. He was able to stand on his feet and actually walked a few steps; as his frock was opened, his arm, with a clot of blood, dropped to the floor. This boy made an excellent recovery. The space between the plastered ceiling and the drum in which the revolutions of the body had taken place was scarcely 7 1/2 inches wide. Horsbeck's case was of a negro of thirty-five who, while pounding resin on a 12-inch leather band, had his hand caught between the wheel and band. His hand, forearm, arm, etc., were rapidly drawn in, and he was carried around until his shoulder came to a large beam, where the body was stopped by resistance against the beam, fell to the floor, and the arm and scapula were completely avulsed and carried on beyond the beam. In this case, also, the man experienced little pain, and there was comparatively little hemorrhage. Maclean [11.17] reports the history of an accident to a man of twenty-three who had both arms caught between a belt and the shaft while working in a woolen factory, and while the machinery was in full operation. He was carried around the shaft with great velocity until his arms were torn off at a point about four inches below the shoulder-joint on each side. The patient landed on his feet, the blood spurting from each brachial artery in a large stream. His fellow-workmen, without delay, wound a piece of rope around each bleeding member, and the man recovered after primary amputation of each stump. Will [11.18] gives an excellent instance of avulsion of the right arm and scapula in a girl of eighteen, who was caught in flax-spinning machinery. The axillary artery was seen lying in the wound, pulsating feebly, but had been efficiently closed by the torsion of the machinery. The girl recovered.
Additional cases of avulsion of the upper extremity are reported by
Avulsion of the Lower Extremity.—The symptoms following avulsion of the upper extremity are seen as well in similar accidents to the leg and thigh, although the latter are possibly the more fatal. Horlbeck [11.28] quotes Benomont's description of a small boy who had his leg torn off at the knee by a carriage in motion; the child experienced no pain, and was more concerned about the punishment he expected to receive at home for disobedience than about the loss of his leg. Carter [11.29] speaks of a boy of twelve who incautiously put the great toe of his left foot against a pinion wheel of a mill in motion. The toe was fastened and drawn into the mill, the leg following almost to the thigh. The whole left leg and thigh, together with the left side of the scrotum, were torn off; the boy died as a result of his injuries.
Ashurst reported to the Pathological Society of Philadelphia the case of a child of nine who had its right leg caught in the spokes of a carriage wheel. The child was picked up unconscious, with its thigh entirely severed, and the bone broken off about the middle third; about three inches higher the muscles were torn from the sheaths and appeared as if cut with a knife. The great sciatic nerve was found hanging 15 inches from the stump, having given way from its division in the popliteal space. The child died in twelve hours. One of the most interesting features of the case was the rapid cooling of the body after the accident and prolongation of the coolness with slight variations until death ensued. Ashurst remarks that while the cutaneous surface of the stump was acutely sensitive to the touch, there was no manifestation of pain evinced upon handling the exposed nerve.
With reference to injuries to the sciatic nerve, Küster [11.30] mentions the case of a strong man of thirty, who in walking slipped and fell on his back. Immediately after rising to his feet he felt severe pain in the right leg and numbness in the foot. He was unable to stand, and was carried to his house, where Küster found him suffering great pain. The diagnosis had been fracture of the neck of the femur, but as there was no crepitation and passive movements caused but little pain, Küster suspected rupture of the sciatic nerve. The subsequent history of the case confirmed this diagnosis. The patient was confined to bed six weeks, and it was five months afterward before he was able to go about, and then only with a crutch and a stick.
Park [11.31] mentions an instance of rupture of the sciatic nerve caused by a patient giving a violent lurch during an operation at the hip-joint.
The instances occasionally observed of recovery of an injured leg after
Washington [11.33] reports in full the case of a boy of eleven, who, in handing a fowling piece across a ditch, was accidentally shot. The contents of the gun were discharged through the leg above the ankle, carrying away five-sixths of the structure—at the time of the explosion the muzzle of the gun was only two feet away from his leg. The portions removed were more than one inch of the tibia and fibula (irregular fractures of the ends above and below), a corresponding portion of the posterior tibial muscle, and the long flexors of the great and small toes, as well as the tissue interposed between them and the Achilles tendon. The anterior tibial artery was fortunately uninjured. The remaining portions consisted of a strip of skin two inches in breadth in front of the wound, the muscles which it covered back of the wound, the Achilles tendon, and another piece of skin, barely enough to cover the tendon. The wound was treated by a bran-dressing, and the limb was saved with a shortening of but 1 1/2 inches.
There are several anomalous injuries which deserve mention. Markoe [11.34] observed a patient of seventy-two, who ruptured both the quadriceps tendons of each patella by slipping on a piece of ice, one tendon first giving way, and followed almost immediately by the other. There was the usual depression immediately above the upper margin of the patella, and the other distinctive signs of the accident. In three months both tendons had united to such an extent that the patient was able to walk slowly. Gibney [11.35] records a case in which the issue was not so successful, his patient being a man who, in a fall ten years previously, had ruptured the right quadriceps tendon, and four years later had suffered the same accident on the opposite side. As a result of his injuries, at the time Gibney saw him, he had completely lost all power of extending the knee-joint. Partridge [11.36] mentions an instance, in a
Marshall [11.37] had under his observation a case in which the femoral artery was ruptured by a cart wheel passing over the thigh, and death ensued although there were scarcely any external signs of contusion and positively no fracture. Boerhaave cites a curious instance in which a surgeon attempted to stop hemorrhage from a wounded radial artery by the application of a caustic, but the material applied made such inroads as to destroy the median artery and thus brought about a fatal hemorrhage.
Spontaneous fractures are occasionally seen, but generally in advanced age, although muscular action may be the cause. There are several cases on record in which the muscular exertion in throwing a stone or ball, or in violently kicking the leg, has fractured one or both of the bones of an extremity. In old persons intracapsular fracture may be caused by such a trivial thing as turning in bed, and even a sudden twist of the ankle has been sufficient to produce this injury. In a boy of thirteen Storrs [11.38] has reported fracture of the femur within the acetabulum. In addition to the causes enumerated, inflammation of osseous tissue, or osteoid carcinoma, has been found at the seat of a spontaneous fracture.
One of the most interesting subjects in the history of surgery is the gradual evolution of the rational treatment of dislocations. Possibly no portion of the whole science was so backward as this. Thirty-five centuries ago Darius, son of Hydaspis, suffered a simple luxation of the foot; it was not diagnosed in this land of Apis and of the deified discoverer of medicine. Among the wise men of Egypt, then in her acme of civilization, there was not one to reduce the simple luxation which any student of the present day would easily diagnose and successfully treat. Throughout the dark ages and down to the present century, the hideous and unnecessary apparatus employed, each decade bringing forth new types, is abundantly pictured in the older books on surgery; in some almost recent works there are pictures of windlasses and of individuals making superhuman efforts to pull the luxated member back—all of which were given to the student as advisable means of treatment.
Relative to anomalous dislocations the field is too large to be discussed here, but there are two recent ones worthy of mention. Bradley [11.39] relates an instance of death following a subluxation of the right humerus backward on the scapula It could not be reduced because the tendon of the biceps lay between the head of the humerus and a piece of the bone which was chipped off.
Congenital Dislocations.—The extent and accuracy of the knowledge possessed by Hippocrates on the subject of congenital dislocations have excited the admiration of modern writers, and until a comparatively recent
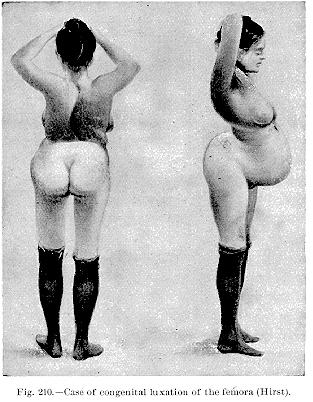
time examples of certain of the luxations described by him had not been recorded. With regard, for instance, to congenital dislocations at the shoulder-joint, little or nothing was known save what was contained in the writings of Hippocrates, till R. M. Smith and Guérin discussed the lesion in their works.
Among congenital dislocations, those of the hips are most common—in fact, 90 per cent. of all. They are sometimes not recognizable until after the lapse of months and sometimes for years, but their causes—faulty developments of the joint, paralysis, etc.—are supposed to have existed at birth. One or both joints may be involved, and according to the amount of involvement the gait is peculiar. As to the reduction of such a dislocation, the most that
The interesting instances of major amputations are so numerous and so well known as to need no comment here. Amputation of the hip with recovery is fast becoming an ordinary operation; at Westminster Hospital in London, there is preserved the right humerus and scapula, presenting an enormous bulk, which was removed by amputation at the shoulder-joint, for a large lymphosarcoma growing just above the clavicle. The patient was a man of twenty-two, and made a good recovery. Another similar preparation is to be seen in London at St. Bartholomew's Hospital.
Simultaneous, synchronous, or consecutive amputations of all the limbs have been repeatedly performed. Champeuois [11.41] reports the case of a Sumatra boy of seven, who was injured to such an extent by an explosion as to necessitate the amputation of all his extremities, and, despite his tender age and the extent of his injuries, the boy completely recovered. Jackson, quoted by Ashhurst, [11.42] had a patient from whom he simultaneously amputated all four limbs for frost-bite.
Muller [11.43] reports a case of amputation of all four limbs for frost-bite, with recovery. The patient, aged twenty-six, while traveling to his home in Northern Minnesota, was overtaken by a severe snow storm, which continued for three days; on December 13th he was obliged to leave the stage in a snow-drift on the prairie, about 110 miles distant from his destination. He wandered over the prairie that day and night, and the following four days, through the storm, freezing his limbs, nose, ears, and cheeks, taking no food or water until, on December 16th, he was found in a dying condition by Indian scouts, and taken to a station-house on the road. He did not reach the hospital at Fort Ridgely until the night of December 24th—eleven days after his first exposure. He was almost completely exhausted, and, after thawing the ice from his clothes, stockings, and boots,—which had not been removed since December 13th,—it was found that both hands and forearms were completely mortified up to the middle third, and both feet and legs as far as the upper third; both knees over and around the patellæ, and the alæ and tip of the nose all presented a dark bluish appearance and fairly circumscribed swelling. No evacuation of the bowels had taken place for over two weeks,
Begg of Dundee [11.44] successfully performed quadruple amputation on a woman, the victim of idiopathic gangrene. With artificial limbs she was able to earn a livelihood by selling fancy articles which she made herself. This woman died in 1885, and the four limbs, mounted on a lay figure, were placed in the Royal College of Surgeons, in London. Wallace, of Rock Rapids, Iowa, has successfully removed both forearms, one leg, and half of the remaining foot, for frost-bite. Allen [11.45] describes the case of a boy of eight who was run over by a locomotive, crushing his right leg, left foot, and left forearm to such an extent as to necessitate primary triple amputation at the left elbow, left foot, and right leg, the boy recovering. Ashhurst remarks that Luckie, Alexander, Koehler, Lowman, and Armstrong have successfully removed both legs and one arm simultaneously for frost-bite, all the patients making excellent recoveries in spite of their mutilations; he adds that he himself has successfully resorted to synchronous amputation of the right hip-joint and left leg for a railroad injury occurring in a lad of fifteen, and has twice synchronously amputated three limbs from the same patient, one case recovering.
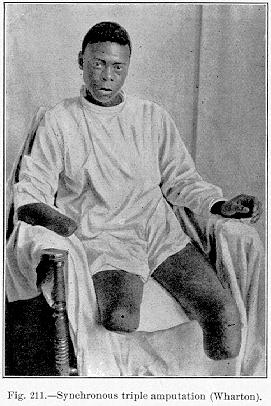
Wharton [11.46] reports a case of triple major amputation on a negro of twenty-one, who was run over by a train (Fig. 211). His right leg was crushed at the knee, and the left leg crushed and torn off in the middle third; the right forearm and hand were crushed. In order to avoid chill and exposure, he was operated on in his old clothes, and while one limb was being amputated the other was being prepared. The most injured member was removed first. Recovery was uninterrupted.
There are two cases of spontaneous amputation worthy of record. Boerhaave mentions a peasant near Leyden, whose axillary artery was divided
of demarcation extended to the spine of the scapula, laying bare the bone and exposing the acromion process and involving the pectoral muscles. It was again decided to let Nature continue her work. The bones exfoliated, the spine and the acromial end of the scapula came away, and a good stump was formed. Figure 212 represents the patient at the age of twenty-eight.
By ingenious mechanical contrivances persons who have lost an extremity are enabled to perform the ordinary functions of the missing member with but slight deterioration. Artificial arms, hands, and legs have been developed to such a degree of perfection that the modern mechanisms of this nature are very unlike the cumbersome and intricate contrivances formerly used.
Le Progrés Médical [11.48] contains an interesting account of a curious contest held between dis-

membered athletes at Nogent-Sur-Marne, a small town in the Department of the Seine, in France. Responding to a general
On several occasions in England, cricket matches have been organized between armless and legless men. In Charles Dickens' paper, "All the Year Round,'' October 5, 1861, there is a reference to a cricket match between a one-armed eleven and a one-legged eleven. There is a recent report from De Kalb, Illinois, of a boy of thirteen who had lost both legs and one arm, but who was nevertheless enabled to ride a bicycle specially constructed for him by a neighboring manufacturer. With one hand he guided the handle bar, and bars of steel attached to his stumps served as legs. He experienced no trouble in balancing the wheel; it is said that he has learned to dismount, and soon expects to be able to mount alone; although riding only three weeks, he has been able to traverse one-half a mile in two minutes and ten seconds. While the foregoing instance is an exception, it is not extraordinary in the present day to see persons with artificial limbs riding bicycles, and even in Philadelphia, May 30, 1896, there was a special bicycle race for one-legged contestants.
The instances of interesting cases of foreign bodies in the extremities are not numerous. In some cases the foreign body is tolerated many years in this location. There are to-day many veterans who have bullets in their extremities. Girdwood [11.49] speaks of the removal of a foreign body after twenty-five years' presence in the forearm. Pike [11.50] mentions a man in India, who, at the age of twenty-two, after killing a wounded hare in the usual manner by striking it on the back of the neck with the side of the hand, noticed a slight cut on the hand which soon healed but left a lump under the skin. It gave him no trouble until two months before the time of report, when he asked to have the lump removed, thinking it was a stone. It was cut down upon and removed, and proved to be the spinous process of the vertebra of a hare. The bone was living and healthy and had formed a sort of arthrodial joint on the base of the phalanx of the little finger and had remained in this position for nearly twenty-two years.
Tousey [11.52] reports a case of foreign body in the axilla that was taken for a necrotic fragment of the clavicle. The patient was a boy of sixteen, who climbed up a lamp-post to get a light for his bicycle lamp; his feet slipped off the ornamental ledge which passed horizontally around the post about four feet from the ground, and he fell. In the fall a lead pencil in his waistcoat pocket caught on the ledge and was driven into the axilla, breaking off out of sight. This was supposed to be a piece of the clavicle, and was only discovered to be a pencil when it was removed six weeks after.
There are several diseases of the bone having direct bearing on the anomalies of the extremities which should have mention here. Osteomalacia
Rachitis or rickets is not a disease of adult life, but of infancy and childhood, and never occurs after the age of puberty. It seldom begins before six months or after three years. There are several theories as to its causation, one being that it is due to an abnormal development of acids. There is little doubt that defective nutrition and bad hygienic surroundings are prominent factors in its production. The principal pathologic change is seen in the epiphyseal lines of long bones and
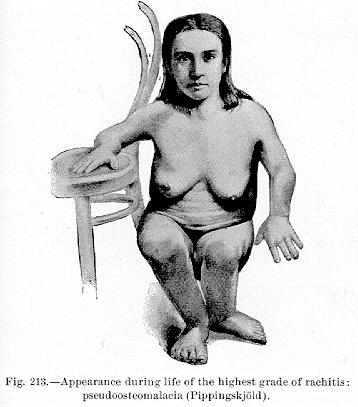
beneath the periosteum. Figure 213 shows the appearance during life of a patient with the highest grade of rachitis, and it can be easily understood what a barrier to natural child-birth it would produce. In rachitis epiphyseal swellings are seen at the wrists and ankle-joints, and in superior cases at the ends of the phalanges of the fingers and toes. When the shaft of a long bone is affected, not only deformity, but even fracture may occur. Under these circumstances the humerus and femur appear to be the bones
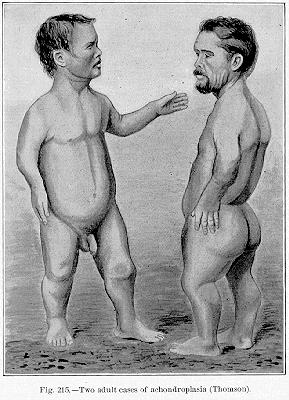
Analogous to rachitis is achondroplasia, or the so called fetal rickets—a disease in which deformity results from an arrest, absence, or perversion of the normal process of enchondral ossification. It is decidedly an intrauterine affection, and the great majority of fetuses die in utero. Thomson [11.53] reports three living cases of achondroplasia. The first was a child five months of age, of pale complexion, bright and intelligent, its head measuring 23 inches in length. There was a narrow thorax showing the distinct beads of rickets; the upper and lower limbs were very short, but improved under antirachitic
Osteitis deformans is a hyperplasia of bone described by Paget in 1856. Paget's patient was a gentleman of forty-six who had always enjoyed good health; without assignable cause he began to be subject to aching pains in the thighs and legs. The bones of the left leg began to increase in size, and a year or two later the left femur; also enlarged considerably. During a period of twenty years these changes were followed by a growth of other bones. The spine became firm and; rigid, the head increased 5 1/4 inches in circumference. The bones of the face were not affected. When standing, the patient had a peculiar bowed condition of the legs, with marked flexure at the knees. He finally died of osteosarcoma, originating in the left radius, Paget collected eight cases, five of whom died of malignant disease. The postmortem of Paget's case showed extreme thickening in the bones affected, the femur and cranium particularly showing osteoclerosis. Several cases have been recorded in this country; according to Warren, Thieberge analyzed 43 cases; 21 were men, 22 women; the disease appeared usually after forty.
Acromegaly is distinguished from osteitis deformans in that it is limited to hypertrophy of the hands, feet, and face, and it usually begins earlier. In gigantism the so-called "giant growth of bones'' is often congenital in character, and is unaccompanied by inflammatory symptoms.
The deformities of the articulations may be congenital but in most cases are acquired. When these are of extreme degree, locomotion is effected in most curious ways. Ankylosis at unnatural angles and even complete reversion of the joints has been noticed. Paré gives a case of reversion, and of crooked hands and feet; and Barlow [11.54] speaks of a child of two and three-quarter years with kyphosis, but mobility of the lumbar region, which walked on its elbows and knees. The pathology of this deformity is obscure, but there might have been malposition in utero. Wilson presented a similar case before the Clinical Society of London, in 1888. The "Camel-boy,'' exhibited some years ago throughout the United States, had reversion of the joints, which resembled those of quadrupeds. He walked on all fours, the mode of progression resembling that of a camel.
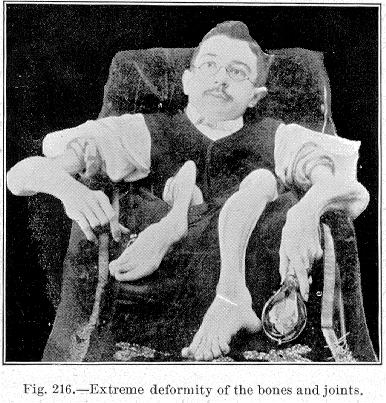
Figure 216 represents Orloff, "the transparent man,'' an exhibitionist, showing curious deformity of the long bones and atrophy of the extremities. He derived his name from the remarkable transparency of his deformed members
Figure 217, taken from Hutchinson's "Archives of Surgery,'' [11.55] represents an extreme case of deformity of the knee-joints in a boy of seven, the result of severe osteoarthritis. The knees and elbows were completely ankylosed.

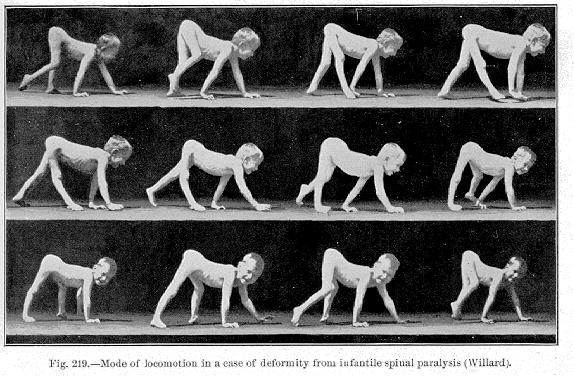
Infantile spinal paralysis is often the cause of distressing deformities, forbidding locomotion in the ordinary manner. In a paper on the surgical and mechanical treatment of such deformities Willard [11.56] mentions a boy of fourteen, the victim of infantile paralysis, who at the age of eleven had never walked, but dragged his legs along (Fig. 218). His legs were greatly twisted, and there was flexion at right angles at the hips and knees. There was equinovarus in the left foot and equinovalgus in the right. By an operation of
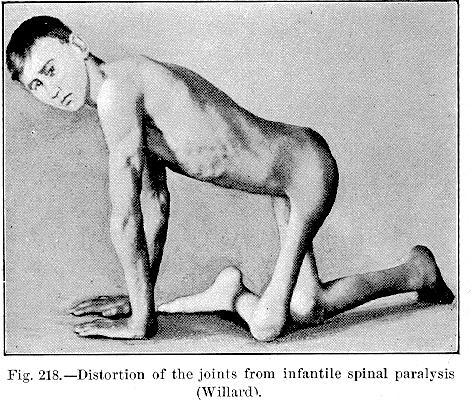
subcutaneous section at the hips, knees, and feet, with application of plaster-of-Paris
Relative to anomalous increase or hypertrophy of the bones of the extremities, Fischer shows that an increase in the length of bone may follow slight injuries. He mentions a boy of twelve, who was run over by a wagon and suffered a contusion of the bones of the right leg. In the course of a year this leg became 4 1/2 cm. longer than the other, and the bones were also much thicker than in the other. Fischer also reports several cases of abnormal growth of bone following necrosis. A case of shortening 3 3/4 cm., after a fracture, was reduced to one cm. by compensatory growth. Elongation of the bone is also mentioned as the result of the inflammation of the joint. Warren also quotes Taylor's case of a lady who fell, injuring, but not fracturing, the thigh. Gradual enlargement, with an outward curving of the bone, afterward took place.
| CHAPTER XI.
SURGICAL ANOMALIES OF THE EXTREMITIES. Anomalies and Curiosities of Medicine | ||