| CHAPTER XVI.
ANOMALOUS SKIN-DISEASES. Anomalies and Curiosities of Medicine | ||
16. CHAPTER XVI.
ANOMALOUS SKIN-DISEASES.
Ichthyosis is a disease of the skin characterized by a morbid development of the papillæ and thickening of the epidermic lamellæ; according as the skin is affected over a larger or smaller area, or only the epithelial lining of the follicles, it is known as ichthyosis diffusa, or ichthyosis follicularis. The hardened masses of epithelium develop in excess, the epidermal layer loses in integrity, and the surface becomes scaled like that of a fish. Ichthyosis may be congenital, and over sixty years ago Steinhausen [16.1] described a fetal monster in the anatomic collection in Berlin, the whole surface of whose body was covered with a thick layer of epidermis, the skin being so thick as to form a covering like a coat-of-mail. According to Rayer the celebrated "porcupine-man'' who exhibited himself in England in 1710 was an example of a rare form of ichthyosis. This man's body, except the face, the palms of the hands, and the soles of the feet, was covered with small excrescences in the form of prickles. These appendages were of a reddish-brown color, and so hard and elastic that they rustled and made a noise when the hand was passed over their surfaces. They appeared two months after birth and fell off every winter, to reappear each summer. In other respects the man was in very good health. He had six children, all of whom were covered with excrescences like himself. The hands of one of these children has been represented by Edwards in his "Gleanings of Natural History.'' A picture of the hand of the father is shown in the fifty-ninth volume of the Philosophical Transactions.
Pettigrew [16.2] mentions a man with warty elongations encasing his whole body. At the parts where friction occurred the points of the elongations were worn off. This man was called "the biped armadillo.'' His great grandfather was found by a whaler in a wild state in Davis's Straits, and for four generations the male members of the family had been so encased. The females had normal skins. All the members of the well-known family of Lambert had the body covered with spines. Two members, brothers, aged twenty-two and fourteen, were examined by Geoffroy-Saint-Hilaire. This thickening of the epidermis and hair was the effect of some morbid predisposition which was transmitted from father to son, the daughters not being affected. Five generations could be reckoned which had been affected in the manner described.
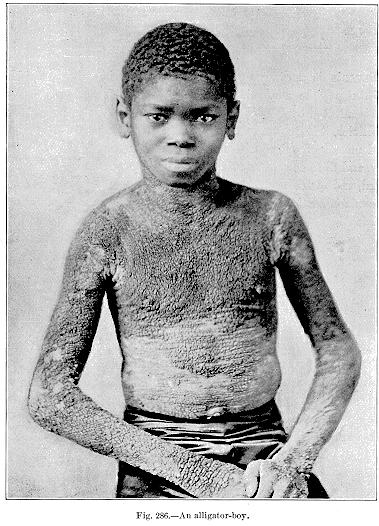
Fig. 286.—An alligator-boy.
[Description: Photograph of "alligator-boy"]
skin was covered with strong hairs like the bristles of a boar. When numerous and thick the scales sometimes assumed a greenish-black hue. An example of this condition was the individual who exhibited under the name of the "alligator-boy.'' Figure 286 represents an "alligator-boy'' exhibited by C. T. Taylor. The skin affected in this case resembled in color and consistency that of a young alligator. It was remarked that his olfactory sense was intact.
Contagious follicular keratosis is an extremely rare affection in which there are peculiar, spine-like outgrowths, consisting in exudations of the mouths of the sebaceous glands. Leloir and Vidal shorten the name to acné cornée.
Erasmus Wilson speaks of it as ichthyosis sebacea cornea. H. G. Brooke describes a case in a girl of six. The first sign had been an eruption of little black spots on the nape of the neck. These spots gradually developed into papules, and the whole skin took on a dirty yellow color. Soon afterward the same appearances occurred on both shoulders, and, in the same order, spread gradually down the outer sides of the arms—first black specks, then papules, and lastly pigmentation. The black specks soon began to project, and comedo-like plugs and small, spine-like growths were produced. Both the spines and plugs were very hard and firmly-rooted. They resisted firm pressure with the forceps, and when placed on sheets of paper rattled like scraps of metal. A direct history of contagion was traced from this case to others.
Mibelli [16.5] describes an uncommon form of keratodermia (porokeratosis). The patient was a man of twenty-one, and exhibited the following changes in his skin: On the left side of the neck, beyond a few centimeters below the lobe of the ear, there were about ten small warty patches, irregularly scattered, yellowish-brown in color, irregular in outline, and varying in size from a lentil to a half-franc piece, or rather more. Similar patches were seen on other portions of the face. Patches of varying size and form, sharply limited by a kind of small, peripheral "dike,'' sinuous but uninterrupted, of a color varying from red to whitish-red, dirty white, and to a hue but little different
Diffuse symmetric scleroderma, or hide-bound disease, is quite rare, and presents itself in two phases: that of infiltration (more properly called hypertrophy) and atrophy, caused by shrinkage. The whole body may be involved, and each joint may be fixed as the skin over it becomes rigid. The muscles may be implicated independently of the skin, or simultaneously, and they give the resemblance of rigor mortis. The whole skin is so hard as to suggest the idea of a frozen corpse, without the coldness, the temperature being only slightly subnormal. The skin can neither be pitted nor pinched. As Crocker has well put it, when the face is affected it is gorgonized, so to speak, both to the eye and to the touch. The mouth cannot be opened; the lids usually escape, but if involved they are half closed, and in either case immovable. The effect of the disease on the chest-walls is to seriously interfere with the respiration and to flatten and almost obliterate the breasts; as to the limbs, from the shortening of the distended skin the joints are fixed in a more or less rigid position. The mucous membranes may be affected, and the secretion of both sweat and sebum is diminished in proportion to the degree of the affection, and may be quite absent. The atrophic type of scleroderma is preceded by an edema, and from pressure-atrophy of the fat and muscles the skin of the face is strained over the bones; the lips are shortened, the gums shrink from the teeth and lead to caries, and the nostrils are compressed. The strained skin and the emotionless features (relieved only by telangiectatic striæ) give the countenance a ghastly, corpse-like aspect. The etiology and pathology of this disease are quite obscure. Happily the prognosis is good, as there is a tendency to spontaneous recovery, although the convalescence may be extended.
Although regarded by many as a disease distinct from scleroderma, morphea is best described as a circumscribed scleroderma, and presents itself in two clinical aspects: patches and bands, the patches being the more common.
Scleroderma neonatorum is an induration of the skin, congenital and occurring soon after birth, and is invariably fatal. A disease somewhat analogous is edema neonatorum, which is a subcutaneous edema with induration affecting the new-born. If complete it is invariably fatal, but in a few cases in which the process has been incomplete recovery has occurred.
Possibly the most interesting of the examples of skin-anomaly was the "elephant-man'' of London (Figs. 287 and 288). His real name was Merrick. He was born at Leicester, and gave an elaborate account of shock experienced by his mother shortly before his birth, when she was knocked down by an elephant at a circus; to this circumstance he attributed his unfortunate condition. He derived his name from a proboscis-like projection of his nose and lips, together with a peculiar deformity of the forehead. He was victimized by showmen during his early life, and for a time was shown in Whitechapel Road, where his exhibition was stopped by the police. He was afterward shown in Belgium, and was there plundered of all his savings. The gruesome spectacle he presented ostracized him from the pleasures of friendship and society, and sometimes interfered with his travels. On one occasion a steamboat captain refused to take him as a passenger. Treves exhibited him twice before the Pathological Society of London. [16.7] His affection was not elephantiasis, but a complication of congenital hypertrophy of certain bones and pachydermatocele and papilloma of the skin. From his youth he suffered from a disease of the left hip-joint. The papillary masses developed on the skin of the back, buttock, and occiput. In the right pectoral and posterior aspect of the right axillary region, and over the buttocks, the affected skin hung in heavy pendulous flaps. His left arm was free from disease. His head grew so heavy that at length he had great difficulty in holding it up. He slept in a sitting or crouching position, with his hands clasped over his legs, and his head on his knees. If he lay down flat, the
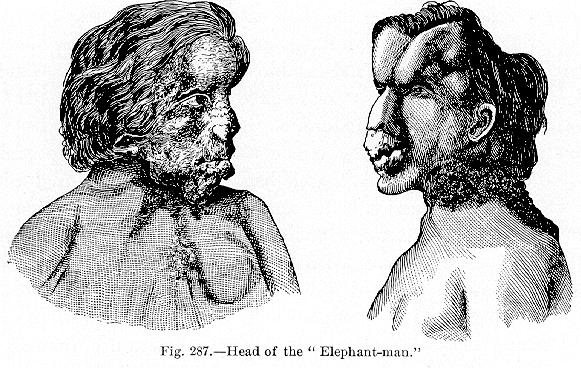
Fig. 287.—Head of the "Elephant-man.''
[Description: Drawing of the head of the "Elephant-man"]
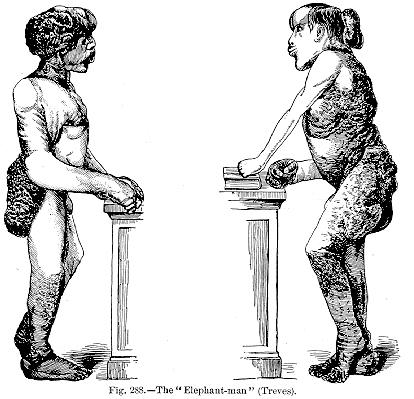
Fig. 288.—The "Elephant-man'' (Treves).
[Description: Drawing of body of the "Elephant-man"]
April 11, 1890; while in bed his ponderous head had fallen backward and dislocated his neck.
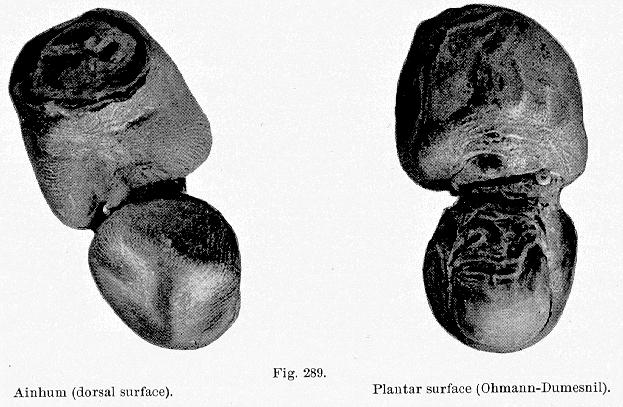
Ainhum may be defined as a pathologic process, the ultimate result of which is a spontaneous amputation of the little toe. It is confined almost
In 1866 da Silva Lima of Bahia, at the Misericordia Hospital, gave the first reports of this curious disease, and for quite a period it was supposed to be confined to Brazilian territory. Since then, however, it has been reported from nearly every quarter of the globe. Relative to its geographic distribution, Pyle [16.8] states that da Silva Lima and Seixas of Bahia have reported numerous cases in Brazil, as have Figueredo, Pereira, Pirovano, Alpin, and Guimares. Toppin reports it in Pernambuco. Mr. Milton reports a case from Cairo, and Dr. Creswell at Suez, both in slaves. E. A. G. Doyle reports several cases at the Fernando Hospital, Trinidad. Digby reports its prevalence on the west coast of Africa, particularly among a race of negroes called Krumens. Messum reports it in the South African Republic, and speaks of its prevalence among the Kaffirs. Eyles reports it on the Gold Coast. It has also been seen in Algiers and Madagascar. Through the able efforts of Her Majesty's surgeons in India the presence of ainhum has been shown in India, and considerable investigation made as to its etiology, pathologic histology, etc. Wise at Dacca, Smyth and Crombie at Calcutta, Henderson at Bombay, and Warden, Sen, Crawford, and Cooper in other portions of Southern India have all rendered assistance in the investigation of ainhum. In China a case has been seen, and British surgeons speak of it as occurring in Ceylon. Von Winckler presents an admirable report of 20 cases at Georgetown, British Guiana. Dr. Potoppidan sends a report of a case in a negress on St. Thomas Island. The disease has several times been observed in Polynesia.
Dr. Hornaday reports a case in a negress from North Carolina, and, curious to relate, Horwitz of Philadelphia and Shepherd of Canada found cases in negroes both of North Carolina antecedents. Dr. James Evans reports a case in a negro seventy-four years of age, at Darlington, S. C. Dr. R. H. Days of Baton Rouge, La., had a case in a negress, and Dr. J. L. Deslates, also of Louisiana, reports four cases in St. James Parish. Pyle has seen a case in a negress aged fifty years, at the Emergency Hospital in Washington.
So prevalent is the disease in India that Crawford found a case in every 2500 surgical cases at the Indian hospitals. The absence of pain or inconvenience in many instances doubtless keeps the number of cases reported few, and again we must take into consideration the fact that the class of persons afflicted with ainhum are seldom brought in contact with medical men.
The disease usually affects the 5th phalanx at the interphalangeal joint. Cases of the 4th and other phalanges have been reported. Cooper speaks of
Ainhum is much more common in males than in females; it is, in fact, distinctly rare in the latter. Of von Winckler's 20 cases all were males.
It may occur at any age, but is most common between thirty and thirty-five. It has been reported in utero by Guyot, and was seen to extend up to the thigh, a statement that is most likely fallacious. However, there are well-authenticated cases in infants, and again in persons over seventy years of age.
In some few cases the metatarso-phalangeal joint is affected; but no case has been seen at the base of the ungual phalanx. The duration of the disease is between two and four years, but Dr. Evans's case had been in progress fifty years. It rarely runs its full course before a year.
Ainhum begins as a small furrow or crack, such as soldiers often experience, at the digito-plantar fold, seen first on the inner side. This process of furrowing never advances in soldiers, and has been given a name more expressive than elegant. In ainhum the toe will swell in a few days, and a pain, burning or shooting in nature, may be experienced in the foot and leg affected. Pain, however, is not constant. There may be an erythematous
The histology of ainhum shows it to be a direct ingrowth of epithelium, with a corresponding depression of surface due to a rapid hyperplasia that pushes down and strangles the papillæ, thus cutting off the blood supply from the epithelial cells, causing them to undergo a horny change.
The disease is not usually symmetric, as formerly stated, nor is it simultaneous in different toes. There are no associated constitutional symptoms, no tendency to similar morbid changes in other parts, and no infiltration elsewhere. There is little or no edema with ainhum. In ainhum there is, first, simple hypertrophy, then active hyperplasia The papillæ degenerate when deprived of blood supply, and become horny. Meanwhile the pressure thus exerted on the nervi vasorum sets up vascular changes which bring about epithelial changes in more distant areas, the process advancing anteriorly, that is, in the direction of the arteries. This makes the cause, according to Eyles, an inflammatory and trophic phenomenon due mainly to changes following pressure on the vasomotor nerves.
Etiology.—The theories of the causation of ainhum are quite numerous. The first cause is the admirable location for a furrow in the digito-plantar fold, and the excellent situation of the furrow for the entrance of sand or other particles to make the irritation constant, thus causing chronic inflammatory changes, which are followed subsequently by the changes peculiar to ainhum. The cause has been ascribed to the practice of wearing rings on the toes; but von Winckler says that in his locality (British Guinea) this practice is confined to the coolie women, and in not one of his 20 cases had a ring been previously worn on the toe; in fact all of the patients were males. Digby says, however, that the Krumens, among whom the disease is common, have long worn brass or copper rings on the fifth toe. Again the
Injury, such as stone-bruise, has been attributed as the initial cause, and well-authenticated cases have been reported in which traumatism is distinctly remembered; but Smyth, Weber, and several other observers deny that habits, accidents, or work, are a feature in causation.
Von Düring reports a curious case which he calls sclerodactylia annularis ainhumoides. The patient was a boy about twelve years old, born in Erzeroum, brought for treatment for scabies, and not for the affection about to be described. A very defective history led to the belief that a similar affection had not been observed in the family. When he was six years old it began on the terminal phalanges of the middle fingers. A myxomatous swelling attacked the phalanges and effected a complete absorption of the terminal phalanx. It did not advance as far as gangrene or exfoliation of bone. At the time of report the whole ten fingers were involved; the bones seemed to be thickened, the soft parts being indurated or sclerosed. In the right index finger a completely sclerosed ring passed around the middle phalanx. The nails on the absorbed phalanges had become small and considerably thickened plates. No analogous changes were found elsewhere, and sensation was perfectly normal in the affected parts. There were no signs whatever of a multiple neuritis nor of a leprous condition.
There is a rare and curious condition known as "deciduous skin'' or keratolysis, in which the owners possess a skin, which, like that of a serpent, is periodically cast off, that of the limbs coming off like the finger of a glove. Preston [16.9] of Canterbury, New Zealand, mentions the case of a woman who had thus shed her skin every few weeks from the age of seven or even earlier. The woman was sixty-seven years of age; the skin in every part of the body came away in casts and cuticles which separated entire and sometimes in one unbroken piece like a glove or stocking. Before each paroxysm she had an associate symptom of malaise. Even the skin of the nose and ears came off complete. None of the patient's large family showed this idiosyncrasy, and she said that she had been told by a medical man that it had been due to catching cold after an attack of small-pox. Frank [16.10] mentions a case in which there was periodic and complete shedding of the cuticle and nails of the hands and feet, which was repeated for thirty-three consecutive years on July 24th of each year, and between the hours of 3 P. M. and 9 P. M. The patient remembered shedding for the first time while a child at play. The paroxysms always commenced abruptly, constitutional febrile symptoms were first experienced, and the skin became dry and hot. The acute symptoms subsided in three or four hours and were entirely gone in twelve hours, with the exception of the redness of the skin, which did not disappear for thirty-six hours more. The patient had been delirious during this
There is a case of general and habitual desquamation of the skin in the Ephemerides of 1686; and Newell [16.11] records a case which recovered under the use of Cheltenham water for several seasons. Latham [16.12] describes a man of fifty who was first seized about ten years previously with a singular kind of fever, and this returned many times afterward, even twice in the course of the same year, attended with the same symptoms and circumstances, and appearing to be brought on by obstructed perspiration, in consequence of catching cold. Besides the common febrile symptoms, upon the invasion of the disease his skin universally itched, more especially at the joints, and the itching was followed by many little red spots, with a small degree of swelling. Soon after this his fingers became stiff; hard, and painful at the ends, and at the roots of the nails. In about twenty-four hours the cuticle began to separate from the cutis, and in ten or twelve days this separation was general from head to foot, during which time he completely turned the cuticle off from the wrists to the fingers' ends like a glove, and in like manner on the legs to the toes, after which his nails shot gradually from their roots, at first with exquisite pain, which abated as the separation of the cuticle advanced, and the old nails were generally thrown off by new ones in about six months. The cuticle rose in the palms and soles like blisters, having, however, no fluid beneath, and when it came off it left the underlying cutis exposed for a few days. Sometimes, upon catching cold, before quite free from feverish symptoms, a second separation of the cuticle from the cutis occurred, but it appeared so thin as to be like scurf, demonstrating the quick renewal of the parts.
There is a similar case in the Philosophical Transactions [16.13] in a miller of thirty-five who was exposed to great heat and clouds of dust. On the first cold a fever attacked him, and once or twice a year, chiefly in the autumn, this again occurred, attended with a loosening and detachment of the cuticle. The disorder began with violent fever, attended with pains in the head, back, limbs, retching, vomiting, dry skin, furred tongue, urgent thirst, constipation, and high-colored urine. Usually the whole surface of the body then became yellow. It afterward became florid like a rash, and then great uneasiness was felt for several days, with general numbness and tingling; the urine then began to deposit a thick sediment. About the third week from the first attack the cuticle appeared elevated in many places, and in eight or ten days afterward became so loose as to admit of its easy removal in large flakes. The cuticle of the hands, from the wrists to the fingers' ends, came off
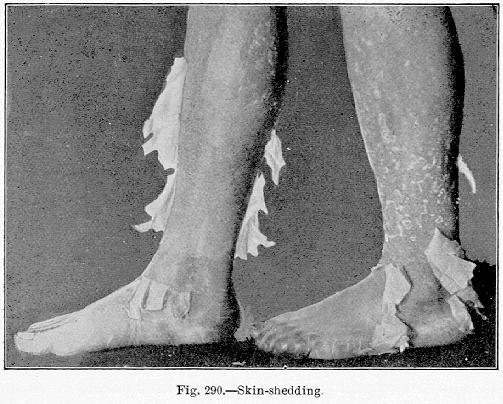
Fig. 290.—Skin shedding.
[Description: Photograph of feet and legs shedding skin]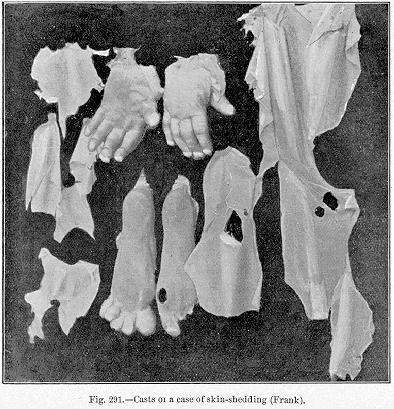
It is quite natural that such cases as this should attract the attention of the laity, and often find report in newspapers. The following is a lay-report of a "snake-boy'' in Shepardstown, Va.:—
"Jim Twyman, a colored boy living with his foster-parents ten miles from this place, is a wonder. He is popularly known as the "snake-boy.'' Mentally he is as bright as any child of his age, and he is popular with his playmates, but his physical peculiarities are probably unparalleled. His entire skin, except the face and hands, is covered with the scales and markings of a snake. These exceptions are kept so by the constant use of Castile soap, but on the balance of his body the scales grow abundantly. The child sheds his skin every year. It causes him no pain or illness. From the limbs it can be pulled in perfect shape, but off the body it comes in pieces. His feet and hands are always cold and clammy. He is an inordinate eater, sometimes spending an hour at a meal, eating voraciously all the time, if permitted to do so. After these gorgings he sometimes sleeps two days. There is a strange suggestion of a snake in his face, and he can manipulate his tongue, accompanied by hideous hisses, as viciously as a serpent.''
Under the name of dermatitis exfoliativa neonatorum, Ritter has described an eruption which he observed in the foundling asylum at Prague, where nearly 300 cases occurred in ten years. According to Crocker it begins in the second or third week of life, and occasionally as late as the fifth week, with diffuse and universal scaling, which may be branny or in laminæ like pityriasis rubra, and either dry or with suffusion beneath the epidermis. Sometimes it presents flaccid bullæ like pemphigus foliaceus, and then there are crusts as well as scales, with rhagades on the mouth, anus, etc.; there is a total absence of fever or other general symptoms. About 50 per cent. die of marasmus and loss of heat, with or without diarrhea. In those who recover the surface gradually becomes pale and the desquamation ceases. Opinions differ regarding it, some considering it of septic origin, while others believe it to be nothing but pemphigus foliaceus. Kaposi regards it as an aggravation of the physiologic exfoliation of the new-born. Elliott of New York [16.14] reports two cases with a review of the subject, but none have been reported in England. Cases on the Continent have been described by Billard, von Baer, Caspary, those already mentioned, and others.
The name epidemic exfoliative dermatitis has been given to an epidemic skin-disease which made its appearance in 1891 in England; 425 cases were collected in six institutions, besides sporadic cases in private houses.
Of sphaceloderma, or gangrene of the skin, probably the most interesting is Raynaud's disease of symmetric gangrene, a vascular disorder, which is seen in three grades of intensity: there is local syncope, producing the condition known as dead-fingers or dead-toes, and analogous to that produced by intense cold; and local asphyxia, which usually follows local syncope, or may develop independently. Chilblains are the mildest manifestation of this condition. The fingers, toes, and ears, are the parts usually affected. In the most extreme degree the parts are swollen, stiff, and livid, and the capillary circulation is almost stagnant; this is local or symmetric gangrene, the mildest form of which follows asphyxia. Small areas of necrosis appear on the pads of the fingers and of the toes; also at the edges of the ears and tip of the nose. Occasional symmetric patches appear on the limbs and trunk, and in extensive cases terminate in gangrene. Raynaud suggested that the local syncope was produced by contraction of the vessels; the asphyxia is probably caused by a dilatation of the capillaries and venules, with persistence of the spasm of the arterioles. According to Osler two forms of congestion occur, which may be seen in adjacent fingers, one of which may be swollen, intensely red, and extremely hot; the other swollen, cyanotic, and intensely cold. Sometimes all four extremities are involved, as in Southey's case, [16.15] in a girl of two and a half in whom the process began on the calves, after a slight feverish attack, and then numerous patches rapidly becoming gangrenous appeared on the backs of the legs, thighs, buttocks, and upper arms, worse where there was pressure; the child died thirty-two hours after the onset. The whole phenomenon may be unilateral, as in Smith's case, quoted by Crocker,— in a girl of three years in whom the left hand was cold and livid, while on the right there was lividity, progressing to gangrene of the fingers and of the thumb up to the first knuckles, where complete separation occurred.
Neuroses of the skin consist in augmentation of sensibility or hyperesthesia and diminution of sensibility or anesthesia. There are some curious old cases of loss of sensation. Ferdinandus [16.17] mentions a case of a young man of twenty-four who, after having been seized with insensibility of the whole body with the exception of the head, was cured by purgatives and other remedies. Bartholinus cites the case of a young man who lost the senses of taste and feeling; and also the case of a young girl who could permit the skin of her forehead to be pricked and the skin of her neck to be burned without experiencing any pain. In his "Surgery'' Lamothe mentions a case of insensibility of the hands and feet in consequence of a horse-kick in the head without the infliction of any external wound. In the "Mémoires de l'Académie des Sciences'' for the year 1743, we read an account of a soldier who, after having accidentally lost all sensation in his left arm, continued to go through the whole of the manual exercise with the same facility as ever. It was also known that La Condamine was able to use his hands for many years after they had lost their sensation. Rayer gives a case of paralysis of the skin of the left side of the trunk without any affection of the muscles, in a man of forty-three of apoplectic constitution. The paralysis extended from

mad. He was greatly frightened by the accident and every time he saw a dog he trembled violently, and on one occasion he suffered a convulsive attack for one and a half hours. The convulsions increased in number and frequency, he lost his memory, and exhibited other signs of incipient dementia. He was admitted to the hospital with two small wounds upon the head, one above the left eyebrow and the other on the scalp, occasioned by a fall on his entrance into the hospital. For several days a great degree of insensibility of the skin of the whole body was observed without any
Duhring [16.18] reports a very rare form of disease of the skin, which may be designated neuroma cutis dolorosum, or painful neuroma of the skin (Fig. 292). The patient was a boiler-maker of seventy who had no family history bearing on the disease. Ten years previously a few cutaneous tubercles the size and shape of a split-pea were noticed on the left shoulder, attended with decided itching but not with pain. The latter symptom did not come on until three years later. In the course of a year or two the lesions increased in number, so that in four years the shoulder and arm were thickly studded with them. During the next five years no particular changes occurred either in lesions or in the degree of pain. The region affected simply looked like a solid sheet of variously-sized, closely-packed, confluent tubercles, hard and dense. The tubercles were at all times painful to the touch, and even the contact of air was sufficient to cause great suffering. During the paroxysms, which occurred usually at several short intervals every day, the skin changed color frequently and rapidly, passing through various reddish and violet tints, at times becoming purplish.
As a paroxysm came on the man was in the habit of gently pressing and holding the arm closely to his body. At one time he endured the attack in a standing posture, walking the floor, but usually he seated himself very near a hot stove, in a doubled-up, cramped position, utterly unmindful of all surroundings, until the worst pain had ceased. Frequently he was unable to control himself, calling out piteously and vehemently and beseeching that his life be terminated by any means. In desperation he often lay and writhed on the floor in agony. The intense suffering lasted, as a rule, for about a half hour, but he was never without pain of the neuralgic type. He was freer of pain in summer than in winter. Exsection of the brachial plexus was performed, but gave only temporary relief. The man died in his eighty-fourth year of senile debility.
According to Osler the tubercula dolorosa or true fascicular neuroma is not always made up of nerve-fibers, but, as shown by Hoggan, may be an adenomatous growth of the sweat-glands.
Yaws may be defined as an endemic, specific, and contagious disease, characterized by raspberry-like nodules with or without constitutional disturbance. Its synonym, frambesia, is from the French, framboise, a raspberry. Yaws is derived from a Carib word, the meaning of which is doubtful. It is a disease confined chiefly to tropical climates, and is found on the west coast of Africa for about ten degrees on each side of the equator, and also on the east coast in the central regions, but rarely in the north. It is also found in Madagascar, Mozambique, Ceylon, Hindoostan, and nearly all the tropical islands of the world. Crocker believes it probable that the
Frambesia or yaws was observed in Brazil as early as 1643, [16.19] and in America later by Lebat in 1722. In the last century Winterbottom and Hume describe yaws in Africa, Hume calling it the African distemper. In 1769 in an essay on the "Natural History of Guiana,'' Bancroft mentions yaws; and Thomson [16.20] speaks of it in Jamaica. Hillary in 1759 describes yaws in Barbadoes; and Bajou in Domingo and Cayenne in 1777, Dazille having already observed it in San Domingo in 1742. [16.21]
Crocker takes his account of yaws from Numa Rat of the Leeward Islands, who divides the case into four stages: incubation, primary, secondary, and tertiary. The incubation stage is taken from the date of infection to the first appearance of the local lesion at the sight of inoculation. It varies from three to ten weeks. The symptoms are vague, possibly palpitation, vertigo, edema of the limbs and eyelids. The primary stage begins with the initial lesion, which consists of a papule which may be found most anywhere on the body. This papule ulcerates. The secondary stage commences about a fortnight after the papule has healed. There is intermittent fever, headache, backache, and shooting pains in the limbs and intercostal spaces, like those of dengue, with nocturnal exacerbations. An eruption of minute red spots appears first on the face, and gradually extends so that the whole body is covered at the end of three days. By the seventh day the apex of the papule is of a pale yellow color, and the black skin has the appearance of being dotted over with yellow wax. The papule then develops into nodules of cylindric shape, with a dome-shaped, thick, yellow crust. It is only with the crust off that there is any resemblance to a raspberry. During the month following the raspberry appearance the skin is covered with scabs which, falling off, leave a pale macula; in dark races the macula becomes darker than normal, but in pale races it becomes paler than the natural skin, and in neither case is it scarcely ever obliterated. Intense itching is almost always present, and anemia is also a constant symptom. The disease is essentially contagious and occurs at all ages and among all sexes, to a lesser degree in whites and hybrids, and is never congenital. It seems to have a tendency to undergo spontaneous recovery.
Furunculus orientalis, or its synonyms, Oriental boil, Aleppo boil, Delhi boil, Biskra button, etc., is a local disease occurring chiefly on the face
Pigmentary Processes.—Friction, pressure, or scratching, if long continued, may produce extensive and permanent pigmentation. This is seen in its highest degree in itching diseases like prurigo and pityriasis. Greenhow [16.22] has published instances of this kind under the name of "vagabond's disease,'' a disease simulating morbus addisonii, and particularly found in tramps and vagrants. In aged people this condition is the pityriasis nigra of Willan. According to Crocker in two cases reported by Thibierge, the oral mucous membrane was also stained. Carrington and Crocker both record cases of permanent pigmentation following exposure to great cold. [16.23] Gautier is accredited with recording in 1890 the case of a boy of six in whom pigmented patches from sepia to almost black began to form at the age of two, and were distributed all over the body. Precocious maturity of the genital organs preceded and accompanied the pigmentation, but the hair was illy developed.
Chloasma uterinum presents some interesting anomalies. Swayne records a singular variety in a woman in whom, during the last three months of three successive pregnancies, the face, arms, hands, and legs were spotted like a leopard, and remained so until after her confinement. Crocker speaks of a lady of thirty whose skin during each pregnancy became at first bronze, as if it had been exposed to a tropical sun, and then in spots almost black. Kaposi knew a woman with a pigmented mole two inches square on the side of the neck, which became quite black at each pregnancy, and which was the first recognizable sign of her condition. It is quite possible that the black disease of the Garo Hills in Assam [16.24] is due to extreme and acute development of a pernicious form of malaria. In chronic malaria the skin may be yellowish, from a chestnut-brown to a black color, after long exposure to the influence of the fever. Various fungi, such as tinea versicolor and the Mexican "Caraati,'' may produce discoloration on the skin.
Acanthosis Nigricans may be defined as a general pigmentation with papillary mole-like growths. In the "International Atlas of Rare Skin Diseases'' there are two cases pictured, one by Politzer in a woman of sixty-two, and the other by Janovsky in a man of forty-two. The regions affected were mostly of a dirty-brown color, but in patches of a bluish-gray. The disease began suddenly in the woman, but gradually in the man. Crocker has
Xeroderma pigmentosum, first described by Kaposi in 1870, is a very rare disease, but owing to its striking peculiarities is easily recognized. Crocker saw the first three cases in England, and describes one as a type. The patient was a girl of twelve, whose general health and nutrition were good. The disease began when she was between twelve and eighteen months old, without any premonitory symptom. The disease occupied the parts habitually uncovered in childhood. The whole of these areas was more or less densely speckled with pigmented, freckle-like spots, varying in tint from a light, raw umber to a deep sepia, and in size from a pin's head to a bean, and of a roundish and irregular shape. Interspersed among the pigment-spots, but not so numerous, were white atrophic spots, which in some parts coalesced, forming white, shining, cicatrix-like areas. The skin upon this was finely wrinkled, and either smooth or shiny, or covered with thin, white scales. On these white areas bright red spots were conspicuous, due to telangiectasis, and there were also some stellate vascular spots and strife interspersed among the pigment. Small warts were seen springing up from some of the pigment spots. These warts ulcerated and gave rise to numerous superficial ulcerations, covered with yellow crusts, irregularly scattered over the face, mostly on the right side. The pus coming from these ulcers was apparently innocuous. The patient complained neither of itching nor of pain. Archambault [16.26] has collected 60 cases, and gives a good resume to date. Amiscis reports two cases of brothers, in one of whom the disease began at eight months, and in the other at a year, and concludes that it is not a lesion due to external stimuli or known parasitic elements, but must be regarded as a specific, congenital dystrophy of the skin, of unknown pathogenesis. However, observations have shown that it may occur at forty-three years (Riehl), and sixty-four years (Kaposi). Crocker believes that the disease is an atrophic degeneration of the skin, dependent on a primary neurosis, to which there is a congenital predisposition.
Nigrities is a name given by the older writers to certain black blotches occurring on the skin of a white person—in other words, it is a synonym of melasma. According to Rayer it is not uncommon to see the scrotum and the skin of the penis of adults almost black, so as to form a marked contrast with the pubes and the upper part of the thighs. Haller [16.27] met with a woman in whom the skin of the pubic region was as black as that of a negress. During nursing the nipples assume a deep black color which disappears after weaning. Le Cat speaks of a woman of thirty years, whose forehead assumed a dusky hue of the color of iron rust when she was pregnant about the seventh month. By degrees the whole face became black except the eyes and the edges of the
Mitchell Bruce has described an anomalous discoloration of the skin and mucous membranes resembling that produced by silver or cyanosis. The patient, a harness-maker of forty-seven, was affected generally over the body, but particularly in the face, hands, and feet. The conjunctival, nasal, and aural mucosa were all involved. The skin felt warm, and pressure did not influence the discoloration. The pains complained of were of an intermittent, burning, shooting character, chiefly in the epigastric and left lumbar regions. The general health was good, and motion and sensation were normal. Nothing abnormal was discovered in connection with the abdominal and thoracic examinations. The pains and discoloration had commenced two years before his admission, since which time the skin had been deepening in tint. He remained under observation for three months without obvious change in his symptoms. There was nothing in the patient's occupation to account for the discoloration. A year and a half previously he had taken medicine for his pains, but its nature could not be discovered. He had had syphilis.
Galtier mentions congenital and bronze spots of the skin. A man born in Switzerland the latter part of the last century, calling himself Joseph Galart, attracted the attention of the curious by exhibiting himself under the
Billard [16.30] has published an extraordinary case of blue discoloration of the skin in a young laundress of sixteen. Her neck, face, and upper part of the chest showed a beautiful blue tint, principally spreading over the forehead, the alæ, and the mouth. When these parts were rubbed with a white towel the blue parts of the skin were detached on the towel, coloring it, and leaving the skin white. The girl's lips were red, the pulse was regular and natural, and her strength and appetite like that of a person in health. The only morbid symptom was a dry cough, but without mucous rattle or any deficiency of the sound of the chest or alteration of the natural beat of the heart. The catamenia had never failed. She had been engaged as a laundress for the past two years. From the time she began this occupation she perceived a blueness around her eyes, which disappeared however on going into the air. The phenomenon reappeared more particularly when irons were heated by a bright charcoal fire, or when she worked in a hot and confined place. The blueness spread, and her breast and abdomen became shaded with an azure blue, which appeared deeper or paler as the circulation was accelerated or retarded. When the patient's face should have blushed, the face became blue instead of red. The changes exhibited were like the sudden transition of shades presented by the chameleon. The posterior part of the trunk, the axillæ, the sclerotic coats of the eyes, the nails, and the skin of the head remained in
Artificial discolorations of the skin are generally produced by tattooing, by silver nitrate, mercury, bismuth, or some other metallic salt.
Melasma has been designated as an accidental and temporary blackish discoloration of the skin. There are several varieties: that called Addison's disease, that due to uterine disease, etc. In this affection the skin assumes a dark and even black hue.
Leukoderma is a pathologic process, the result of which is a deficiency in the normal pigmentation of the skin, and possibly its appendages. Its synonyms are leukopathia, vitiligo, achroma, leukasmus, and chloasma album. In India the disease is called sufaid-korh, meaning white leprosy. It has numerous colloquial appellations, such as chumba or phoolyree (Hindoo), buras (Urdu), cabbore (Singalese), kuttam (Taneil), dhabul (Bengal). It differs from albinism in being an acquired deficiency of pigment, not universal and not affecting the eye. Albinism is congenital, and the hair and eyes are affected as well as the skin.
The disease is of universal distribution, but is naturally more noticeable in the dark-skinned races. It is much more common in this country among the negroes than is generally supposed.
The "leopard-boy of Africa,'' so extensively advertised by dime museums over the country, was a well-defined case of leukoderma in a young mulatto, a fitting parallel for the case of ichthyosis styled the "alligator-boy.''
Figure 293 represents a family of three children, all the subjects of leukoderma. Leukoderma is more common among females. It is rarely seen in children, being particularly a disease of middle age. Bissell reports a case in an Indian ninety years of age, subsequent to an attack of rheumatism thirty years previous. It is of varying duration, nearly every case giving a different length of time. It may be associated with most any disease, and is directly attributable to none. In a number of cases collected rheumatism has been a marked feature. It has been noticed following typhoid fever and pregnancy.
In white persons there are spots or blotches of pale, lustreless appearance either irregular or symmetric, scattered over the body. In the negro and other dark-skinned races a mottled appearance is seen. If the process goes to completion, the whole surface changes to white. The hair, though rarely affected, may present a mottled appearance. There seems to be no constitutional disturbances, no radical change in the skin, no pain—in fact, no disturbance
It appears first in small spots, either on the lips, nose, eyelids, soles, palms, or forehead, and increases peripherally—the several spots fusing together. The skin is peculiarly thin and easily irritated. Exposure to the sun readily blisters it, and after the slightest abrasion it bleeds freely. Several cases have been reported in which the specific gravity of the urine was extremely high, due to an excess of urea. Wood calls attention to the wave-like

Fig. 293.—"The leopard family.''
[Description: Photograph of three members of "the leopard family"]
course of leukoderma, receding on one side, increasing on the other. The fading is gradual, and the margins may be abrupt or diffuse. The mucous membranes are rosy. The functions of the swell-glands are unimpaired.
The theory of the absence of pigment causing a loss of the olfactory sense, spoken of by Wallace, is not borne out by several observations of Wood and others. Wilson says: "Leukasma is a neurosis, the result of weakened innervation of the skin, the cause being commonly referable to the organs of assimilation or reproduction.'' It is not a dermatitis, as a dermatitis usually
Many observers have noticed that negroes become several degrees lighter after syphilization; but no definite relation between syphilis and leukoderma has yet been demonstrated in this race. Postmortem examinations of leukodermic persons show no change in the suprarenal capsule, a supposed organ of pigmentation.
Climate has no influence. It is seen in the Indians of the Isthmus of Darien, the Hottentots, and the Icelanders. Why the cells of the rete mucosum should have the function in some races of manufacturing or attracting pigment in excess of those of other races, is in itself a mystery. By his experiments on the pigment-cells of a frog Lister has established the relation existing between these elements and innervation, which formerly had been supposititious.
Doubtless a solution of the central control of pigmentation would confirm the best theory of the cause of leukoderma—i. e., faulty innervation of the skin. At present, whether the fault is in the cell proper, the conducting media, or the central center, we are unable to say. It is certainly not due to any vascular disturbances, as the skin shows no vascular changes.
White spots on the nails are quite common, especially on young people. The mechanic cause is the presence of air between the lamellæ of the affected parts, but their origin is unknown. According to Crocker in some cases they can be shown to be a part of trophic changes. Bielschowsky [16.31] records the case of a man with peripheral neuritis, in whom white spots appeared at the lower part of the finger-nails, grew rapidly, and in three weeks coalesced into a band across each nail a millimeter wide. The toes were not affected. Shoemaker mentions a patient who suffered from relapsing fever and bore an additional band for each relapse. Crocker quotes a case reported by Morison of Baltimore, in which transverse bars of white, alternating with the normal color, appeared without ascertainable cause on the finger-nails of a young lady and remained unchanged.
Giovannini describes a case of canities unguium in a patient of twenty-nine, following an attack of typhoid fever. On examining the hands of this patient the nails showed in their entire extent a white, opaque, almost ivory color. An abnormal quantity of air found in the interior of the nails explains in this particular case their impaired appearance. It is certain that the nails,
Plica polonica, or, as it was known in Cracow—weicselzopf, is a disease peculiar to Poland, or to those of Polish antecedents, characterized by the agglutination, tangling, and anomalous development of the hair, or by an alteration of the nails, which become spongy and blackish. In older days the disease was well known and occupied a prominent place in books on skin-diseases. Hercules de Saxonia and Thomas Minadous, in 1610, speak of plica as a disease already long known. The greater number of writers fix the date of its appearance in Poland at about the year 1285, under the reign of Lezekle-Noir. Lafontaine [16.32] stated that in the provinces of Cracow and Sandomir plica formerly attacked the peasantry, beggars, and Jews in the proportion of 1 1/2 in 20; and the nobility and burghers in the proportion of two in 30 or 40. In Warsaw and surrounding districts the disease attacked the first classes in the proportion of one to ten, and in the second classes one to 30. In Lithuania the same proportions were observed as in Warsaw; but the disease has gradually grown rarer and rarer to the present day, although occasional cases are seen even in the United States.
Plica has always been more frequent on the banks of the Vistula and Borysthenes, in damp and marshy situations, than in other parts of Poland. The custom formerly prevailing in Poland of shaving the heads of children, neglect of cleanliness, the heat of the head-dress, and the exposure of the skin to cold seem to favor the production of this disease.
Plica began after an attack of acute fever, with pains like those of acute rheumatism in the head and extremities, and possibly vertigo, tinnitus aurium, ophthalmia, or coryza. Sometimes a kind of redness was observed on the thighs, and there was an alteration of the nails, which became black and rough, and again, there was clammy sweat. When the scalp was affected the head was sore to the touch and excessively itchy. A clammy and agglutinating sweat then occurred over the cranium, the hair became unctuous, stuck together, and appeared distended with an adhesive matter of reddish-brown color, believed by many observers to be sanguineous. The hair was so acutely sensitive that the slightest touch occasioned severe pain at the roots. A viscid matter of a very offensive smell, like that of spoiled vinegar, or according to Rayer like that of mice or garlic, exuded from the whole surface of each affected hair. This matter glued the hairs together, at first from their exit at the skin, and then along the entire length; it appeared to be secreted from the whole surface of the scalp and afterward dried into an incrustation. If there was no exudation the disease was called plica sicca. The hair was matted and stuck together in a variety of ways, so as to resemble ropes (plica multiformis).
Tinea nodosa is a name given by Morris and Cheadle to a case of nodular growth on the beard and whiskers of a young man. In a case noticed by Crocker this disease affected the left side of the mustache of a medical man, who complained that the hair, if twisted up, stuck together. When disintegrated the secretion in this case seemed to be composed of fungous spores. Epithelium fragments, probably portions of the internal root-sheath, sometimes adhere to the shaft of the hair as it grows up, and look like concretions. Crocker states that he is informed by White of Boston that this disease is common in America in association with alopecia furfuracea, and is erroneously thought to be the cause of the loss of hair, hence the popular name, "hair-eaters.''
Jamieson reports a case of mycosis in a native of Aberdeenshire aged thirty-eight. There was no history of any previous illness. The disease began three years previous to his application for treatment, as a red, itching, small spot on the cheek. Two years later lumps presented themselves, at first upon his shoulders. The first thing to strike an
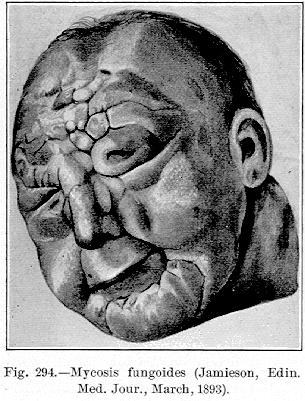
observer was the offensive odor about the patient. In the hospital wards it made all the occupants sick. The various stages of the disease were marked upon the different parts of the body. On the chest and abdomen it resembled an eczema, on the shoulders there were brown, pinkish-red areas. On the scalp the hair was scanty, the eye-brows denuded, and the eyelashes absent. The forehead was leonine in aspect. From between the various nodosities a continual discharge exuded, the nodosities being markedly irregular over the limbs. The backs of the hands, the dorsums of the feet, the wrists and ankles, had closely approximating growths upon them, while under the thick epidermis of the palms of the hands were blisters. Itching was intense. The patient became emaciated and died thirteen days after his admission into the hospital. A histologic examination showed the sarcomatous nature of the various growths. The disease differed
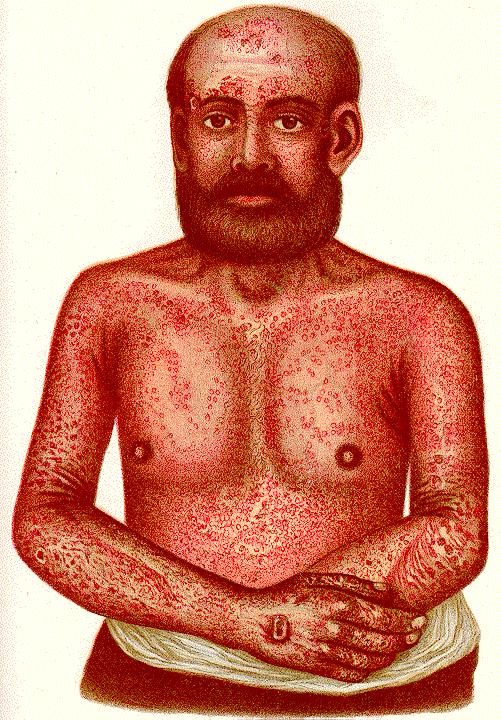
Morris [16.37] described an interesting case of universal dermatitis, probably a rare variety of mycosis fungoides (Plate 12). The patient had for many years a disease which had first appeared on the arms and legs, and which was usually regarded by the physicians who saw the case as eczema. At times the disease would entirely disappear, but it relapsed, especially during visits to India. At the time the patient came under the care of Morris, his general health seemed unaffected. The skin of the whole body, except the face, the scalp, and the front of the chest, was of a mahogany color. The skin of the lips was so thickened that it could not be pinched into folds, and was of a mottled appearance, due to hemorrhagic spots. All over the thickened and reddened surface were scattered crops of vesicles and boils. The nails were deformed, and the toes beyond the nails were tense with a serous accumulation. The glands in the right axilla and the groin were much enlarged. The hair on the pubes had disappeared. The abdomen was in a condition similar to that upon the limbs, but less in degree. The front of the chest below the nipples was covered with dark papules the size of a pin's head. The back, the buttocks, the face, and the scalp presented similar lesions. The most striking lesions were three ulcers—one on the back of the right hand, one on the right temple, and the other on the left cheek. The largest was the size of a florin, and had elevated borders, somewhat infiltrated; they were covered with a brown, dry scab. The patient suffered from itching at night so that he could not sleep. He was kept under observation, and in spite of treatment the malady advanced in a periodic manner, each exacerbation being preceded by a feeling of tension in the parts, after which a crop of vesicles would appear. Sometimes, especially on the feet, bullæ formed. The patient finally left the hospital and died of an intercurrent attack of pneumonia. A microscopic examination revealed a condition which might be found with a number of the chronic affections of the skin, but, in addition, there were certain cell-inclusions which were thought to represent psorosperms. Morris thought this case corresponded more to mycosis fungoides than any other malady.
| CHAPTER XVI.
ANOMALOUS SKIN-DISEASES. Anomalies and Curiosities of Medicine | ||