| CHAPTER X.
SURGICAL ANOMALIES OF THE HEAD AND
NECK. Anomalies and Curiosities of Medicine | ||
10. CHAPTER X.
SURGICAL ANOMALIES OF THE HEAD AND
NECK.
Injuries of such a delicate organ as the eye, in which the slightest accident can produce such disastrous consequences, naturally elicit the interest of all. Examples of exophthalmos, or protrusion of the eye from the orbit from bizarre causes, are of particular interest. Among the older writers we find Ficker [10.1] and the Ephemerides giving instances of exophthalmos from vomiting. Fabricius Hildanus [10.2] mentions a similar instance. Salmuth, *[706] Verduc, *[799] and others mention extrusion of the eyeball from the socket, due to excessive coughing. Ab Heers *[409] and Sennert *[732] mention instances in which after replacement the sight was uninjured. Tyler relates the case of a man who, after arising in the morning, blew his nose violently, and to his horror his left eye extruded from the orbit. With the assistance of his wife it was immediately replaced and a bandage placed over it. When Tyler saw him the upper lid was slightly swollen and discolored, but there was no hemorrhage.
Hutchinson [10.3] describes extrusion of the eyeball from the orbit caused by a thrust with a stick. There was paraphymotic strangulation of the globe, entirely preventing replacement and necessitating excision. Reyssie [10.4] speaks of a patient who, during a fire, was struck in the right eye by a stream of water from a hose, violently thrusting the eye backward. Contracting under the double influence of shock and cold, the surrounding tissues forced the eyeball from the orbit, and an hour later Reyssie saw the patient with the eye hanging by the optic nerve and muscles. Its reduction was easy, and after some minor treatment vision was perfectly restored in the injured organ. Thirty months after the accident the patient had perfect vision, and the eye had never in the slightest way discommoded him.
Bodkin [10.5] mentions the case of a woman of sixty who fell on the key in a door and completely avulsed her eye. In von Graefe's Archiv there is a record of a man of seventy-five who suffered complete avulsion of the eye by a cartwheel passing over his head. Verhaeghe records [10.6] complete avulsion of the eye caused by a man falling against the ring of a sharp-worn key. Hamill [10.7]
In former days there was an old-fashioned manner of fighting called "gouging.'' In this brutal contest the combatant was successful who could, with his thumb, press his opponent's eyeball out. Strange to say, little serious or permanently bad results followed such inhuman treatment of the eye. Von Langenbeck of Berlin mentions an instance of fracture of the superior maxilla, in which the eyeball was so much displaced as to lodge in the antrum of Highmore. Von Becker of Heidelberg reports the history of a case in which a blow from the horn of a cow dislocated the eye so far back in the orbit as to present the appearance of enucleation. The conjunctiva hid the organ from view, but when it was pulled aside the eyeball was exposed, and in its remote position still possessed the power of vision. In some cases in which exophthalmos has been seemingly spontaneous, extreme laxity of the lids may serve as an explanation. There is an instance on record in which a Polish dew appeared in a Continental hospital, saying that while turning in bed, without any apparent cause, his eyeball was completely extruded. There have been people who prided themselves on their ability to produce partial exophthalmos.
Rupture of the Eyeball.—Jessop mentions the case of a child of eight who suffered a blow on the eye from a fall against a bedpost, followed by compound rupture of the organ. The wound in the sclerotic was three or four lines in length, and the rent in the conjunctiva was so large that it required three sutures. The chief interest in this case was the rapid and complete recovery of vision.
Adler [10.9] reports a case of fracture of the superior maxillary in which the dislocated bone-fragment of the lower orbital border, through pressure on the inferior maxillary and counter pressure on the skull, caused rupture of the conjunctiva of the left eye.
Serious Sequelæ of Orbital Injuries.—In some instances injuries primarily to the orbit either by extension or implication of the cerebral contents provoke the most serious issues. Pointed instruments thrust into the orbital cavity may by this route reach the brain. There is a record [10.10] of death
Pepper records a case in which a knife was thrust through the spheroidal fissure, wounding a large meningeal vein, causing death from intracranial hemorrhage. Nélaton describes an instance in which the point of an umbrella wounded the cavernous sinus and internal carotid artery of the opposite side, causing the formation of an arteriovenous aneurysm which ultimately burst, and death ensued. Polaillon [10.12] saw a boy of eighteen who was found in a state of coma. It was stated that an umbrella stick had been thrust up through the roof of the orbit and had been withdrawn with much difficulty. The anterior lobe of the brain was evidently much wounded; an incision was made in the forehead and a portion of the frontal bone chiseled away entrance being thus effected, the aura was incised, and some blood and cerebrospinal fluid escaped. Five splinters were removed and a portion of the damaged brain-substance, and a small artery was tied with catgut. The debris of the eyeball was enucleated and a drain was placed in the frontal wound, coming out through the orbit. The patient soon regained consciousness and experienced no bad symptoms afterward. The drains were gradually withdrawn, the process of healing advanced rapidly, and recovery soon ensued.
Annandale [10.13] mentions an instance in which a knitting-needle penetrated the brain through the orbit. Hewett [10.14] speaks of perforation of the roof of the orbit and injury to the brain by a lead-pencil.
Gunshot Injuries of the Orbit.—Barkan [10.15] recites the case in which a leaden ball 32/100 inch in diameter was thrown from a sling into the left orbital cavity, penetrating between the eyeball and osseous wall of the orbit without rupturing the tunics of the eye or breaking the bony wall of the cavity. It remained lodged two weeks without causing any pain or symptoms, and subsequently worked itself forward, contained in a perfect conjunctival sac, in which it was freely movable.
Buchanan [10.16] recites the case of a private in the army who was shot at a
It is said [10.17] that an old soldier of one of Napoleon's armies had a musket-ball removed from his left orbit after twenty-four years' lodgment. He was struck in the orbit by a musket-ball, but as at the same time a companion fell dead at his side he inferred that the bullet rebounded from his orbit and killed his comrade. For twenty-four years he had suffered from cephalalgia and pains and partial exophthalmos of the left eye. After removal of the ball the eye partially atrophied.
Warren reports a case of a man of thirty-five whose eyeball was destroyed by the explosion of a gun, the breech-pin flying off and penetrating the head. The orbit was crushed; fourteen months afterward the man complained of soreness on the hard palate, and the whole breech-pin, with screw attached, was extracted. The removal of the pin was followed by fissure of the hard palate, which, however, was relieved by operation. The following is an extract [10.18] of a report by Wenyon of Fatshan, South China:—
"Tang Shan, Chinese farmer, thirty-one years of age, was injured in the face by the bursting of a shot-gun. After being for upward of two months under the treatment of native practitioners, he came to me on December 4, 1891. I observed a cicatrix on the right side of his nose, and above this a sinus, still unhealed, the orifice of which involved the inner canthus of the right eye, and extended downward and inward for about a centimeter. The sight of the right eye was entirely lost, and the anterior surface of the globe was so uniformly red that the cornea could hardly be distinguished from the surrounding conjunctiva. There was no perceptible enlargement or protrusion of the eyeball, and it did not appear to have sustained any mechanical injury or loss of tissue. The ophthalmia and keratitis were possibly caused by the irritating substances applied to the wound by the Chinese doctors. The sinus on the side of the nose gave exit to a continuous discharge of slightly putrid pus, and the patient complained of continuous headache and occasional dizziness, which interfered with his work. The pain was referred to the right frontal and temporal regions, and the skin on this part of the head had a slight blush, but there was no superficial tenderness. The patient had been told by his native doctors, and he believed it himself, that there was no foreign body in the wound; but on probing it I easily recognized the lower edge of a hard metallic substance at a depth of about one inch posteriorly from the orifice of the sinus. Being unable to obtain any reliable information as to the probable size or shape of the object, I cautiously made several attempts to remove it through a slightly enlarged opening, but without success. I therefore continued the incision along the side of the nose to the nostril,
The extent of permanent injury done by foreign bodies in the orbit is variable. In some instances the most extensive wound is followed by the happiest result, while in others vision is entirely destroyed by a minor injury.
Carter [10.19] reports a case in which a hat-peg 3 3/10 inches long and about 1/4 inch in diameter (upon one end of which was a knob nearly 1/2 inch in diameter) was impacted in the orbit for from ten to twenty days, and during this
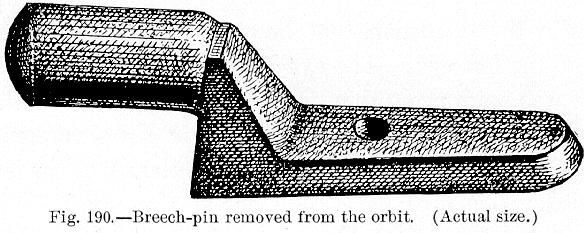
Fig. 190.—Breech-pin removed from the orbit (Actual size.)
[Description: Drawing of a breech-pin]
time the patient was not aware of the fact. Recovery followed its extraction, the vision and movements of the eye being unimpaired.
According to the Philosophical Transactions [10.20] a laborer thrust a long lath with great violence into the inner canthus of the left eye of his fellow workman, Edward Roberts. The lath broke off short, leaving a piece two inches long, 1/2 inch wide, and 1/4 inch thick, in situ. Roberts rode about a mile to the surgery of Mr. Justinian Morse, who extracted it with much difficulty; recovery followed, together with restoration of the sight and muscular action. The lath was supposed to have passed behind the eyeball. Collette [10.21] speaks of an instance in which 186 pieces of glass were extracted from the left orbit, the whole mass weighing 186 Belgian grains. They were blown in by a gust of wind that broke a pane of glass; after extraction no affection of the brain or eye occurred. Watson [10.22] speaks of a case in which a chip of steel 3/8 inch long was imbedded in cellular tissue of the orbit for four days, and was removed without injury to the eye. Wordsworth [10.23] reports a case in which a foreign body was deeply imbedded in the orbit for six weeks, and was removed
Foreign bodies are sometimes contained in the eyeball for many years. There is an instance on record [10.25] in which a wooden splinter, five mm. long and two mm. broad, remained in the eye forty-seven years. It was extracted, with the lens in which it was lodged, to relieve pain and other distressing symptoms. Snell [10.26] reports a case in which a piece of steel was imbedded and encapsulated in the ciliary process twenty-nine years without producing sympathetic irritation of its fellow, but causing such pain as to warrant enucleation of this eye. Gunning [10.27] speaks of a piece of thorn 5/8 inch long, imbedded in the left eyeball of an old man for six years, causing total loss of vision; he adds that, after its removal, some improvement was noticed.
Williams mentions a stone-cutter whose left eye was put out by a piece of stone. Shortly after this his right eye was wounded by a knife, causing traumatic cataract, which was extracted by Sir William Wilde, giving the man good sight for twelve years, after which iritis attacked the right eye and produced a false membrane over the pupil so that the man could not work. It was in this condition that he consulted Williams, fourteen years after the loss of the left eye. The eye was atrophied, and on examination a piece of stone was seen projecting from it directly between the lids. The visible portion was 1/4 inch long, and the end in the shrunken eye was evidently longer than the end protruding. The sclera was incised, and, after fourteen years' duration in the eye, the stone was removed.
Taylor [10.28] reports the removal of a piece of bone which had remained quiescent in the eye for fourteen years; after the removal of the eye the bone was found adherent to the inner tunics. It resembled the lens in size and shape. Williams [10.29] mentions continual tolerance of foreign bodies in the eyeball for fifteen and twenty-two years; and Chisholm [10.30] reports the lodgment of a fragment of metal in the iris for twenty-three years. Liebreich [10.31] extracted a piece of steel from the interior of the eye where it had been lodged twenty-two years. Barkar [10.32] speaks of a piece of steel which penetrated through the cornea and lens, and which, five months later, was successfully removed by the extraction of the cataractous lens. Critchett [10.33] gives an instance of a foreign body being loose in the anterior chamber for sixteen years. Rider [10.34] speaks of the lodgment of a fragment of a copper percussion cap in the left eye, back of the inner ciliary margin of the iris, for thirty-five years; and Bartholinus [10.35] mentions a thorn in the canthus for thirty years. Jacob [10.36] reports a case in which a chip of iron remained in the eyeball twenty-eight years
Snell [10.37] gives an instance in which a piece of steel was imbedded close to the optic disc with retention of sight. It was plainly visible by the opthalmoscope eighteen months after the accident, when as yet no diminution of sight was apparent. Smyly [10.38] speaks of a portion of a tobacco pipe which was successfully removed from the anterior chamber by an incision through the cornea. Clark [10.39] mentions a case in which molten lead in the eye caused no permanent injury; and there are several cases mentioned in confirmation of the statement that the eye seems to be remarkably free from disastrous effects after this injury.
Williamson [10.40] mentions eyelashes in the anterior chamber of the eye, the result of a stab wound of this organ.
Contusion of the eyeball may cause dislocation of the lens into the anterior chamber, and several instances have been recorded. We regret our inability to give the reference or authority for a report that we have seen, stating that by one kick of a horse the lenses of both eyes of a man were synchronously knocked through the eyeballs by the calkins of the horseshoe. Oliver mentions extraction of a lens by a thrust of a cow's horn.
Lowe [10.41] speaks of rupture of the anterior capsule of the lens from violent sneezing, with subsequent absorption of the lenticular substance and restoration of vision. Trioen [10.42] mentions a curious case of expulsion of the crystalline lens from the eye in ophthalmia, through the formation of a corneal fissure. The authors have personal knowledge of a case of spontaneous extrusion of the lens through a corneal ulcer, in a case of ophthalmia of the new-born.
Injury of the Eyeball by Birds.—There are several instances in which birds have pierced the eyeball with their bills, completely destroying vision. Not long since a prominent taxidermist winged a crane, picked it up, and started to examine it, when it made one thrust with its bill and totally destroyed his eyeball. In another instance a man was going from the railroad station to his hotel in a gale of wind, when, as he turned the corner of the street, an English sparrow was blown into his face. Its bill penetrated his eyeball and completely ruined his sight. There are several instances on record in which game fowls have destroyed the eyes of their owners. In one case a game cock almost completed the enucleation of the eye of his handler by striking him with his gaff while preparing in a cock-pit.
Moorehead [10.43] explains a rare accident to an eye as follows:—
"Mr. S. B. A., while attending to his bees, was stung by one upon the right upper eyelid near its center. An employee, who was assisting in the work, immediately discovered the sting driven in the lid and cautiously extracted
"The next morning, the trouble continuing, he came to me for relief. Upon examination of the lid, no opening could be made out where the sting had penetrated, and a minute inspection of the conjunctival surface with a good glass failed to reveal any foreign substance. Cleansing the lid thoroughly, and carefully inspecting with a lens under strong light, a minute dark point was made out about the center of the lid. Feeling that this might be the point of the sting, I had recourse to several expedients for its removal, but without success. Finally, with a fine knife, I succeeded in cutting down by the side of the body and tilting it out. Examination with a 1/5 inch objective confirmed my opinion that it was the point of the bee-sting.
"The barbed formation of the point explains how, under the stroking with the finger, it was forced through the dense tarsal cartilage and against the cornea of the eye.''
There is a story told in La Médecine Moderne [10.44] of a seamstress of Berlin who was in the habit of allowing her dog to lick her face. She was attacked with a severe inflammation of the right eye, which had to be enucleated, and was found full of tenia echinococcus, evidently derived from the dog's tongue.
Gabb [10.45] mentions a case of epistaxis in which the blood welled up through the lacrimal ducts and suffused into the eye so that it was constantly necessary to wipe the lower eyelid, and the discharge ceased only when the nose stopped bleeding. A brief editorial note on epistaxis through the eyes, referring to a case in the Medical News of November 30, 1895, provoked further reports from numerous correspondents. Among others, the following:—
"Dr. T. L. Wilson of Bellwood, Pa., relates the case of an old lady of seventy-eight whom he found with the blood gushing from the nostrils. After plugging the nares thoroughly with absorbent cotton dusted with tannic acid he was surprised to see the blood ooze out around the eyelids and trickle down the cheeks. This oozing continued for the greater part of an hour, being controlled by applications of ice to both sides of the nose.''
"Dr. F. L. Donlon of New York City reports the case of a married woman, about fifty years old, in whom epistaxis set in suddenly at 11 P. M., and had continued for several hours, when the anterior nares were plugged.
"Dr. T. G. Wright of Plainville, Conn., narrates the case of a young man whom he found in the night, bleeding profusely, and having already lost a large amount of blood. Shortly after plugging both anterior and posterior nares the blood found its way through the lacrimal ducts to the eyes and trickled down the cheeks.''
"Dr. Charles W. Crumb cites the case of a man, sixty-five years old, with chronic nephritis, in whom a slight bruise of the nose was followed by epistaxis lasting twenty-four hours. When the nares were plugged blood escaped freely from the eyes. A cone-shaped bit of sponge, saturated with ferrous sulphate, was passed into each anterior naris, and another piece of sponge, similarly medicated, into either posterior naris. The patient had been taking various preparations of potassium, and it was thought that his blood contained a deficiency of fibrin. Upon removal of the nasal plugs a catarrhal inflammation developed which lasted a long time and was attended with considerable purulent discharge.''
Late Restoration of Sight.—There are some marvelous cases on record in which, after many years of blindness, the surgeon has been able, by operation, to restore the sight. McKeown [10.46] gives the history of a blind fiddler of sixty-three, who, when one and a half years old, had lost the sight of both eyes after an attack of small-pox. Iridectomy was performed, and after over sixty years of total blindness his sight was restored; color-perception was good. Berncastle [10.47] mentions a case of extraction of double cataract and double iridectomy for occluded pupils, which, after thirty years of blindness, resulted in the recovery of good sight. The patient was a blind beggar of Sydney.
To those interested in this subject, Jauffret [10.48] has a most interesting description of a man by the name of Garin, who was born blind, who talked at eight or nine months, showed great intelligence, and who was educated at a blind asylum. At the age of twenty-four he entered the hospital of Forlenze, to be operated upon by that famous oculist. Garin had never seen, but could distinguish night or darkness by one eye only, and recognized orange and red when placed close to that eye. He could tell at once the sex and age of a person approximately by the voice and tread, and formed his conclusions more rapidly in regard to females than males. Forlenze diagnosed cataract, and, in the presence of a distinguished gathering, operated with the happiest result. The description that follows, which is quoted by Fournier [10.49] and is readily accessible to any one, is well worth reading, as it contains an account of the first sensations of light, objects, distance, etc., and minor analogous
Hansell and Clark *[843] say that the perplexities of learning to see after twenty-six years of blindness from congenital disease, as described by a patient of Franke, remind one of the experience of Shelley's Frankenstein. Franke's patient was successfully operated on for congenital double cataract, at twenty-six years of age. The author describes [10.50] the difficulties the patient had of recognizing by means of vision the objects he had hitherto known through his other senses, and his slowness in learning to estimate distances and the comparative size of objects.
Sight is popularly supposed to be occasionally restored without the aid of art, after long years of blindness. Benjamin Rush saw a man of forty-five who, twelve years before, became blind without ascertainable cause, and recovered his sight equally without reason. St. Clair mentions Marshal Vivian, who at the age of one hundred regained sight that for nearly forty years had gradually been failing almost to blindness, and preserved this new sight to the time of his death.
There are many superstitions prevalent among uneducated people as to "second sight,'' recovery of vision, etc., which render their reports of such things untrustworthy. The real explanations of such cases are too varied for discussion here.
Nyctalopia etymologically means night blindness, but the general usage, making the term mean night-vision, is so strongly intrenched that it is useless and confusing to attempt any reinstatement of the old significance. The condition in which one sees better by night, relatively speaking, than by day is due to some lesion of the macular region, rendering it blind. At night the pupil dilates more than in the day-time, and hence vision with the extramacular or peripheral portions of the retina is correspondingly better. It is, therefore, a symptom of serious retinal disease. All night-prowling animals have widely dilatable pupils, and in addition to this they have in the retina a special organ called the tapetum lucidum, the function of which is to reflect to a focus in front of them the relatively few rays of light that enter the widely-dilated pupil and thus enable them the better to see their way. Hence the luminous appearance of the eyes of such animals in the dark.
Hemeralopia (etymologically day-blindness, but by common usage meaning day-vision or night-blindness) is a symptom of a peculiar degenerative disease of the retina, called retinitis pigmentosa. It also occurs in some cases of extreme denutrition, numerous cases having been reported among those who make the prolonged fasts customary in the Russian church. In retinitis pigmentosa the peripheral or extramacular portions of the retina are subject to a pigmentary degeneration that renders them insensitive to light, and patients so afflicted are consequently incapable of seeing at night as well as others. They stumble and run against objects easily seen by the normal eye.
Other forms of retinal injury from too great or too prolonged exposure to light are "moon-blindness,'' due to sleeping with the eyes exposed to bright moonlight, and that due to lightning—a case, e.g., being reported by Knies. [10.52] Silex [10.53] also reports such a case and reviews the reported cases, 25 in number, in ten of which cataract ensued. In the Annual of the Universal Medical Sciences, 1888, there is a report of seven cases of retinal injury with central scotoma, amblyopia, etc., in Japanese medical students, caused by observation of the sun in eclipse.
In discussing the question of electric-light injuries of the eyes Gould [10.54] reviews the literature of the subject and epitomizes the cases reported up to that time. They numbered 23. No patient was seriously or permanently injured, and none was in a person who used the electric light in a proper manner as an illuminant. All were in scientific investigators or workmen about the light, who approached it too closely or gazed at it too long and without the colored protecting spectacles now found necessary by such workers.
Injuries to the Ear.—The folly of the practice of boxing children's ears, and the possible disastrous results subsequent to this punishment, are well exemplified throughout medical literature. Stewart [10.55] quotes four cases of rupture of the tympanum from boxing the ears, and there is an instance [10.56] of a boy of eight, who was boxed on the ear at school, in whom subsequent brain-disease developed early, and death followed. Roosa of New York mentions the loss of hearing following a kiss on the ear. [10.57]
Dalby, [10.58] in a paper citing many different causes of rupture of the tympanic membrane, mentions the following: A blow in sparring; violent sneezing; blowing the nose; forcible dilatation of the Eustachian canal; a thorn or twig of a tree accidentally thrust into the head; picking the ear with a toothpick. In time of battle soldiers sometimes have their tympanums ruptured by the concussion caused by the firing of cannon. Dalby mentions an instance of an officer who was discharged for deafness acquired in this manner during the Crimean War. He was standing beside a mortar which, unexpectedly to him, was fired, causing rupture of the tympanic membrane, followed by hemorrhage from the ear. Similar cases were reported in the recent naval engagements between the Chinese and Japanese. Wilson [10.59] reports two
Perforation of the Tympanum.—Kealy [10.61] relates an instance in which a pin was introduced into the left ear to relieve an intolerable itching. It perforated the tympanum, and before the expiration of twenty-four hours was coughed up from the throat with a small quantity of blood. The pin was bent at an angle of about 120 degrees. Another similar case [10.62] was that of a girl of twenty-two who, while pricking her ear with a hair-pin, was jerked or struck on the arm by a child, and the pin forced into the ear; great pain and deafness followed, together with the loss of taste on the same side of the tongue; after treatment both of the disturbed senses were restored. A man of twenty [10.63] was pricked in the ear by a needle entering the meatus. He uttered a cry, fell senseless, and so continued until the fourth day when he died. The whole auditory meatus was destroyed by suppuration. Gamgee [10.64] tells of a constable who was stabbed in the left ear, severing the middle meningeal artery, death ensuing. In this instance, after digital compression, ligature of the common carotid was practiced as a last resort. There is an account [10.65] of a provision-dealer's agent who fell asleep at a public house at Tottenham. In sport an attendant tickled his ear with a wooden article used as a pipe light. A quick, unconscious movement forced the wooden point through the tympanum, causing cerebral inflammation and subsequent death. There is a record [10.66] of death, in a child of nine, caused by the passage of a knitting-needle into the auditory meatus.
Kauffmann [10.67] reports a case of what he calls objective tinnitus aurium, in which the noise originating in the patient's ears was distinctly audible by others. The patient was a boy of fourteen, who had fallen on the back of his head and had remained unconscious for nearly two weeks. The noises were bilateral, but more distinct on the left than on the right side. The sounds were described as crackling, and seemed to depend on movements of
The introduction of foreign bodies in the ear is usually accidental, although in children we often find it as a result of sport or curiosity. There is an instance on record of a man who was accustomed to catch flies and put them in his ear, deriving from them a pleasurable sensation from the tickling which ensued. There have been cases in which children, and even adults, have held grasshoppers, crickets, or lady-birds to their ears in order to more attentively listen to the noise, and while in this position the insects have escaped and penetrated the auditory canal. Insects often enter the ears of persons reposing in the fields with the ear to the ground. Fabricius Hildanus speaks of a cricket penetrating the ear during sleep. Calhoun [10.68] mentions an instance of disease of the ear which he found was due to the presence of several living maggots in the interior of the ear. The patient had been sleeping in a horse stall in which were found maggots similar to those extracted from his ear. An analogous instance was seen in a negro in the Emergency Hospital, Washington, D. C., in the summer of 1894; and many others are recorded. The insects are frequently removed only after a prolonged lodgment.
D'Aguanno [10.69] gives an account of two instances of living larvæ of the musca sarcophaga in the ears of children. In one of the cases the larvæ entered the drum-cavity through a rupture in the tympanic membrane. In both cases the maggots were removed by forceps. Haug [10.70] has observed a tic (ixodes ricinus) in the ear of a lad of seventeen. The creature was killed by a mercuric-chlorid solution, and removed with a probe.
There is a common superstition that centipedes have the faculty of entering the ear and penetrating the brain, causing death. The authors have knowledge of an instance in which three small centipedes were taken from the ear of a policeman after remaining there three days; during this time they caused excruciating pain, but there was no permanent injury. The Ephemerides contains instances in which, while yet living, worms, crickets, ants, and beetles have all been taken from the ear. In one case the entrance of a cricket in the auditory canal was the cause of death. Martin [10.71] gives an instance in which larvæ were deposited in the ear. Stalpart van der Wiel *[750] relates an instance of the lodgment of a living spider in the ear.
Far more common than insects are inanimate objects as foreign bodies in the ear, and numerous examples are to be found in literature. Fabricius Hildanus *[334] tells of a glass ball introduced into the auditory canal of a girl of ten, followed by headache, numbness on the left side, and after four or five years epileptic seizures, and atrophy of the arm. He extracted it and the symptoms immediately ceased. Sabatier speaks of an abscess of the brain caused by a ball of paper in the ear; and it is quite common for persons in
Alley [10.74] mentions a New Orleans wharf laborer, in whose ear was poured some molten lead; seventeen months afterward the lead was still occupying the external auditory meatus. It is quite remarkable that the lead should have remained such a length of time without causing meningeal inflammation. There was deafness and palsy of that side of the face. A fungous growth occupied the external portion of the ear; the man suffered pain and discharge from the ear, and had also great difficulty in closing his right eyelid. Morrison [10.75] mentions an alcoholic patient of forty who, on June 6, 1833, had nitric acid poured in her right ear. There were no headache, febrile symptoms, stupor, or vertigo. Debility alone was present. Two weeks after the injury paralysis began on the right side, and six weeks from the injury the patient died. This case is interesting from the novel mode of death, the perfect paralysis of the arm, paralysis agitans of the body (occurring as hemorrhage from the ear came on, and subsiding with it), and extensive caries of the petrous bone, without sensation of pain or any indicative symptoms.
There is an instance in a young girl in which a piece of pencil remained in the right ear for seven years. [10.76] Haug speaks of two beads lying in the auditory canal for twenty-eight years without causing any harm.
A boy of six introduced a carob-nut kernel into each ear. On the next day incompetent persons attempted to extract the kernel from the left side, but only caused pain and hemorrhage. The nut issued spontaneously from the right side. In the afternoon the auditory canal was found excoriated and red, and deep in the meatus the kernel was found, covered with blood. The patient had been so excited and pained by the bungling attempts at extraction that the employment of instruments was impossible; prolonged employment of injections was substituted. Discharge from the ear commenced, intense fever and delirium ensued, and the patient had to be chloroformed to facilitate the operation of extraction. The nut, when taken out, was found to have a consistency much larger than originally, caused by the agglutination of wax and blood. Unfortunately the symptoms of meningitis increased; three days
Fleury de Clermont [10.78] mentions a woman of twenty-five who consulted him for removal of a pin which was in her right ear. Vain attempts by some of her lay-friends to extract the pin had only made matters worse. The pin was directed transversely, and its middle part touched the membrane tympanum. The mere touching of the pin caused the woman intense pain; even after etherization it was necessary to construct a special instrument to extract it. She suffered intense cephalalgia and other signs of meningitis; despite vigorous treatment she lost consciousness and died shortly after the operation.
Winterbotham [10.79] reports an instance in which a cherry-stone was removed from the meatus auditorius after lodgment of upward of sixty years. Marchal de Calvi mentions intermittent deafness for forty years, caused by the lodgment of a small foreign body in the auditory canal. There is an instance in which a carious molar tooth has been tolerated in the same location for forty years. [10.80]
Albucasius, Fabricius Hildanus, Paré, and others, have mentioned the fact that seeds and beans have been frequently seen to increase in volume while lodged in the auditory canal. Tulpius *[842] speaks of an infant, playing with his comrades, who put a cherry-seed in his ear which he was not able to extract. The seed increased in volume to such an extent that it was only by surgical interference that it could be extracted, and then such serious consequences followed that death resulted. Albers [10.81] reports an instance in which a pin introduced into the ear issued from the pharynx.
Confusion of diagnosis is occasionally noticed in terrified or hysteric persons. Lowenberg was called to see a child of five who had introduced a button into his left ear. When he saw the child it complained of all the pain in the right ear, and he naturally examined this ear first but found nothing to indicate the presence of a foreign body. He examined the ear supposed to be healthy and there found the button lying against the tympanum. This was explained by the fact that the child was so pained and terrified by the previous explorations of the affected ear that rather than undergo them again he presented the well ear for examination. In the British Medical Journal for 1877 is an account of an unjustified exploration of an ear for a foreign body by an incompetent physician, who spent a half hour in exploration and manipulation, and whose efforts resulted in the extraction of several pieces of bone. The child died in one and a half hours afterward from extreme hemorrhage, and the medical bungler was compelled to appear before a coroner's jury in explanation of his ignorance.
In the external ear of a child Tansley observed a diamond which he
In the Therapeutic Gazette, August 15, 1896, there is a translation of the report of a case by Voss, in which a child of five pushed a dry pea in his ear. Four doctors spent several days endeavoring to extract it, but only succeeded in pushing it in further. It was removed by operation on the fifth day, but suppuration of the tympanic cavity caused death on the ninth day.
Barclay [10.84] reports a rare case of ensnared aural foreign body in a lady, aged about forty years, who, while "picking'' her left ear with a so-called "invisible hair-pin'' several hours before the consultation, had heard a sudden "twang'' in the ear, as if the hair-pin had broken. And so, indeed, it had; for on the instant she had attempted to jerk it quickly from the ear the sharp extremity of the inner portion of its lower prong sprang away from its fellow, penetrated the soft tissues of the floor of the external auditory canal, and remained imbedded there, the separated end of this prong only coming away in her grasp. Every attempt on her part to remove the hair-pin by traction on its projecting prong—she durst not force it inward for fear of wounding the drumhead—had served but to bury the point of the broken prong more deeply into the flesh of the canal, thereby increasing her suffering. Advised by her family physician not to delay, she forthwith sought advice and aid. On examination, it was found that the lower prong of the "invisible hair-pin'' had broken at the outer end of its wavy portion, and seemed firmly imbedded in the floor of the auditory canal, now quite inflamed, at a point about one-third of its depth from the outlet of the canal. The loop or turn of the hair-pin was about 1/2 inch from the flaccid portion of the drumhead, and, together with the unbroken prong, it lay closely against the roof of the canal. Projecting from the meatus there was enough of this prong to be easily grasped between one's thumb and finger. Removal of the hair-pin was effected by first inserting within the meatus a Gruber speculum, encircling the unbroken projecting prong, and then raising the end of the broken one with a long-shanked aural hook, when the hair-pin was readily withdrawn. The wound of the canal-floor promptly healed.
In the severest forms of scalp-injuries, such as avulsion of the scalp from the entangling of the hair in machinery, skin-grafting or replantation is of particular value. Ashhurst [10.85] reports a case which he considers the severest case of scalp-wound that he had ever seen, followed by recovery. The patient was a girl of fifteen, an operative in a cotton-mill, who was caught by
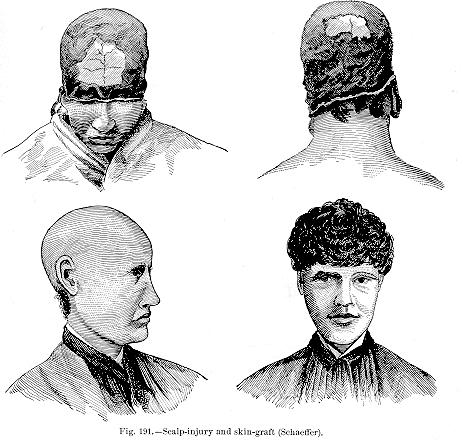
Schaeffer [10.88] has presented quite an extensive article on scalp-injuries in which grafting and transplantation has been used, and besides reporting his own he mentions several other cases. One was that of a young lady of twenty-four. While at work under a revolving shaft in a laundry the wind blew her hair and it was caught in the shaft. The entire skull was laid bare from the margin of the eyelids to the neck. The nasal bones were uncovered and broken, exposing the superior nasal meatus. The skin of the eyelids was removed from within three mm. of their edges. The lower margin of the wound
Schaeffer also reports the case of a woman working in a button factory at Union City, Conn., in 1871, who placed her head under a swiftly turning shaft to pick up a button, when her hair caught in the shaft, taking off her scalp from the nape of the neck to the eyebrows. The scalp was cleansed by her physician, Dr. Bartlett, and placed on her head about two hours after the accident, but it did not stay in position. Then the head was covered twice by skin-grafts, but each time the grafts were lost; but the third time a successful grafting was performed and she was enabled to work after a period of two years. The same authority also quotes Wilson and Way of Bristol, Conn., in an account of a complete avulsion of the scalp, together with tearing of the eyelid and ear. The result of the skin-grafting was not given. Powell of Chicago gives an account of a girl of nineteen who lost her scalp while working in the Elgin Watch Factory at Elgin, Illinois. The wound extended across the forehead above the eyebrows, but the ears were untouched. Skin-grafting was tried in this case but with no result, and the woman afterward lost an eye by exposure, from retraction of the eyelid.
In some cases extensive wounds of the scalp heal without artificial
Cerebral Injuries.—The recent advances in brain-surgery have, in a measure, diminished the interest and wonder of some of the older instances of
major injuries of the cerebral contents with unimportant after-results, and in reviewing the older cases we must remember that the recoveries were made under the most unfavorable conditions, and without the slightest knowledge of all important asepsis and antisepsis.
Penetration or even complete transfixion of the brain is not always attended with serious symptoms. Dubrisay [10.90] is accredited with the description of a man of forty-four, who, with suicidal intent, drove a dagger ten cm. long and one cm. wide into his brain. He had deliberately held the dagger
Warren describes a case of epilepsy of seven months' standing, from depression of the skull caused by a red hot poker thrown at the subject's head. Striking the frontal bone just above the orbit, it entered three inches into the cerebral substance. Kesteven [10.91] reports the history of a boy of thirteen who, while holding a fork in his hand, fell from the top of a load of straw. One of the prongs entered the head one inch behind and on a line with the lobe of the left ear and passed upward and slightly backward to almost its entire length. With some difficulty it was withdrawn by a fellow workman; the point was bent on itself to the extent of two inches. The patient lived nine days. Abel and Colman [10.92] have reported a case of puncture of the brain with loss of memory, of which the following extract is an epitome: "A railway-fireman, thirty-six years old, while carrying an oil-feeder in his hand, slipped and fell forward, the spout of the can being driven forcibly into his face. There was transitory loss of consciousness, followed by twitching and jerking movements of the limbs, most marked on the left side, the legs being drawn up and the body bent forward. There was no hemorrhage from mouth, nose, or ears. The metallic spout of the oil-can was firmly fixed in the base of the skull, and was only removed from the grasp of the bone by firm traction with forceps. It had passed upward and toward the middle line, with its concavity directed from the middle line. Its end was firmly plugged by bone from the base of the skull. No hemorrhage followed its removal. The wound was cleansed and a simple iodoform-dressing applied. The violent jerking movements were replaced by a few occasional twitchings. It was now found that the left side of the face and the left arm were paralyzed, with inability to close the left eye completely. The man became drowsy and confused, and was unable to give replies to any but the simplest questions. The temperature
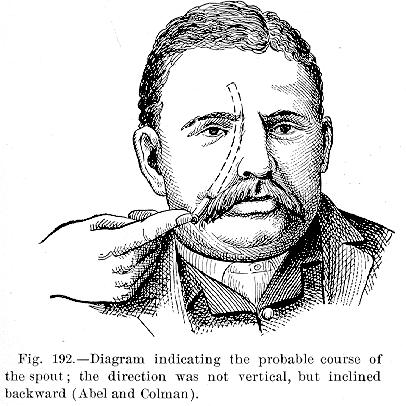
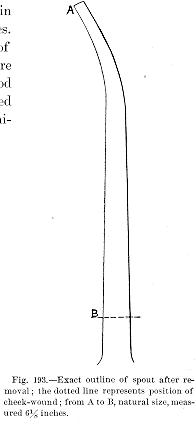
persisted, although the man was able to get about. Sensibility was lost to all forms of stimuli in the right upper eyelid, forehead, and anterior part of the scalp, corresponding with the distribution of the supraorbital and nasal nerves. The cornea was completely anesthetic, and the right cheek, an inch and a half external to the angle of the nose, presented a small patch of anesthesia. There was undue emotional mobility, the patient laughing or crying on slight provocation. The condition of mind-blindness remained. It is believed that the spout of the oil-can must have passed under the zygoma to the base of the skull, perforating the great wing of the spheroid bone and penetrating
Figures 192 and 193 show the outline and probable course of the spout.
Beaumont [10.93] reports the history of an injury in a man of forty-five, who, standing but 12 yards away, was struck in the orbit by a rocket, which penetrated through the spheroidal fissure into the middle and posterior lobes of the left hemisphere. He did not fall at the time he was struck, and fifteen minutes after the stick was removed he arose without help and walked away. Apparently no extensive cerebral lesion had been caused, and the man suffered no subsequent cerebral symptoms except, three years afterward, impairment of memory.
There is an account given by Chelius [10.94] of an extraordinary wound caused by a ramrod. The rod was accidentally discharged while being employed in loading, and struck a person a few paces away. It entered the head near the root of the zygomatic arch, about a finger's breadth from the outer corner of the right eye, passed through the head, emerging at the posterior superior angle of the parietal bone, a finger's breadth from the sagittal suture, and about the same distance above the superior angle of the occipital bone. The wounded man attempted to pull the ramrod out, but all his efforts were ineffectual. After the tolerance of this foreign body for some time, one of his companions managed to extract it, and when it was brought out it was as straight as the day it left the maker's shop. Little blood was lost, and the wound healed rapidly and completely; in spite of this major injury the patient recovered.
Carpenter [10.95] reports the curious case of an insane man who deliberately bored holes through his skull, and at different times, at a point above the ear, he inserted into his brain five pieces of No. 20 broom wire from 2 1/16 to 6 3/4 inches in length, a fourpenny nail 2 1/4 inches long, and a needle 1 5/8 inches long. Despite these desperate attempts at suicide he lived several months, finally accomplishing his purpose by taking an overdose of morphin. MacQueen [10.96] has given the history of a man of thirty-five, who drove one three-inch nail into his forehead, another close to his occiput, and a third into his vertex an inch in front and 1/4 inch to the left of the middle line. He had used a hammer to effect complete penetration, hoping that death would result from his injuries. He failed in this, as about five weeks later he was discharged from the Princess Alice Hospital at Eastbourne, perfectly recovered. There is a record [10.97] of a man by the name of Bulkley who was found, by a police officer in Philadelphia, staggering along the streets, and was taken to the inebriate ward of the Blockley Hospital, where he subsequently sank and died, after having been transferred from ward to ward, his symptoms appearing inexplicable. A postmortem examination revealed the fact that an ordinary knife-blade had been driven into his brain on the right side, just above
Thudicum [10.98] mentions the case of a man who walked from Strafford to Newcastle, and from Newcastle to London, where he died, and in his brain was found the breech-pin of a gun. Neiman [10.99] describes a severe gunshot wound of the frontal region, in which the iron breech-block of an old-fashioned muzzle-loading gun was driven into the substance of the brain, requiring great force for its extraction. The patient, a young man of twenty-eight, was unconscious but a short time, and happily made a good recovery. A few pieces of bone came away, and the wound healed with only a slight depression of the forehead. Wilson [10.100] speaks of a child who fell on an upright copper paper-file, which penetrated the right side of the occipital bone, below the external orifice of the ear, and entered the brain for more than three inches; and yet the child made a speedy recovery.
Baron Larrey knew of a man whose head was completely transfixed by a ramrod, which extended from the middle of the forehead to the left side of the nape of the neck; despite this serious injury the man lived two days.
Jewett [10.101] records the case of an Irish drayman who, without treatment, worked for forty-seven days after receiving a penetrating wound of the skull 1/4 inch in diameter and four inches deep. Recovery ensued in spite of the delay in treatment.
Gunshot Injuries.—Swain [10.102] mentions a patient who stood before a looking glass, and, turning his head far around to the left, fired a pistol shot into his brain behind the right ear. The bullet passed into his mouth, and he spat it out. Some bleeding occurred from both the internal and external wounds; the man soon began to suffer with a troublesome cough, with bloody expectoration; his tongue was coated and drawn to the right; he became slightly deaf in his right ear and dragged his left leg in walking. These symptoms, together with those of congestion of the lung, continued for about a week, when he died, apparently from his pulmonary trouble.
Ford [10.103] quotes the case of a lad of fifteen who was shot in the head, 3/4 inch anterior to the summit of the right ear, the ball escaping through the left os frontis, 1 1/4 inch above the center of the brow. Recovery ensued, with a cicatrix on the forehead, through which the pulsations of the brain could be distinctly seen. The senses were not at all deteriorated.
Richardson [10.104] tells of a soldier who was struck by a Minié ball on the left temporal bone; the missile passed out through the left frontal bone 1/2 inch to the left of the middle of the forehead. He was only stunned, and twenty-four hours later his intellect was undisturbed. There was no operation; free
Angle [10.105] records the case of a cowboy who was shot by a comrade in mistake. The ball entered the skull beneath the left mastoid process and passed out of the right eye. The man recovered.
Rice [10.106] describes the case of a boy of fourteen who was shot in the head, the ball directly traversing the brain substance, some of which protruded from the wound. The boy recovered. The ball entered one inch above and in front of the right ear and made its exit through the lambdoidal suture posteriorly.
Hall of Denver, Col., [10.107] in an interesting study of gunshot wounds of the brain, writes as follows:—
"It is in regard to injuries involving the brain that the question of the production of immediate unconsciousness assumes the greatest interest. We may state broadly that if the medulla or the great centers at the base of the brain are wounded by a bullet, instant unconsciousness must result; with any other wounds involving the brain-substance it will, with very great probability, result. But there is a very broad area of uncertainty. Many instances have been recorded in which the entrance of a small bullet into the anterior part of the brain has not prevented the firing of a second shot on the part of the suicide. Personally, I have not observed such a case, however. But, aside from the injuries by the smallest missiles in the anterior parts of the brain, we may speak with almost absolute certainty with regard to the production of unconsciousness, for the jar to the brain from the blow of the bullet upon the skull would produce such a result even if the damage to the brain were not sufficient to do so.
"Many injuries to the brain from bullets of moderate size and low velocity do not cause more than a temporary loss of consciousness, and the subjects are seen by the surgeon, after the lapse of half an hour or more, apparently sound of mind. These are the cases in which the ball has lost its momentum in passing through the skull, and has consequently done little damage to the brain-substance, excepting to make a passage for itself for a short distance into the brain. It is apparently well established that, in the case of the rifle-bullet of high velocity, and especially if fired from the modern military weapons using nitro-powders, and giving an enormous initial velocity to the bullet, the transmission of the force from the displaced particles of brain (and this rule applies to any other of the soft organs as well) to the adjacent parts is such as to disorganize much of the tissue surrounding the original track of the missile. Under these circumstances a much slighter wound would be necessary to produce unconsciousness or death than in the case of a bullet of low velocity, especially if it were light in weight. Thus I have recorded elsewhere an
"Slight injury to the brain, and especially if it be unilateral, then, may not produce unconsciousness. It is not very uncommon for a missile from a heavy weapon to strike the skull, and be deflected without the production of such a state. Near the town in which I formerly practiced, the town-marshal shot at a negro, who resisted arrest, at a distance of only a few feet, with a 44-caliber revolver, striking the culprit on the side of the head. The wound showed that the ball struck the skull and plowed along under the scalp for several inches before emerging, but it did not even knock the negro down, and no unconsciousness followed later. I once examined an express-messenger who had been shot in the occipital region by a weapon of similar size, while seated at his desk in the car. The blow was a very glancing one and did not produce unconsciousness, and probably, as in the case of the negro, because it did not strike with sufficient directness.''
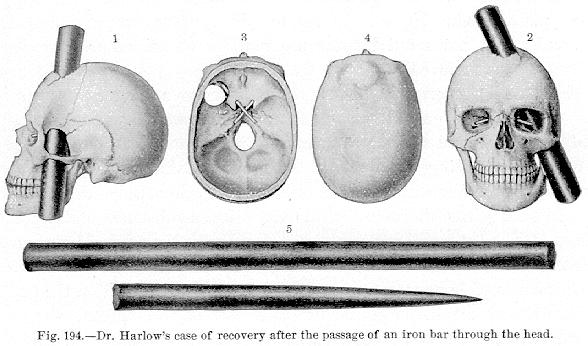
Head Injuries with Loss of Cerebral Substance.—The brain and its membranes may be severely wounded, portions of the cranium or cerebral substance destroyed or lost, and yet recovery ensue. Possibly the most noted injury of this class was that reported by Harlow [10.108] and commonly known as "Bigelow's Case'' or the "American Crow-bar Case.'' Phineas P. Gage, aged twenty-five, a foreman on the Rutland and Burlington Railroad, was employed September 13, 1847, in charging a hole with powder preparatory to blasting. A premature explosion drove a tamping-iron, three feet seven inches long, 1 1/4 inches in diameter, weighing 13 1/4 pounds, completely through the man's head. The iron was round and comparatively smooth; the pointed end entered first. The iron struck against the left side of the face, immediately anterior to the inferior maxillary and passed under the zygomatic arch, fracturing portions of the spheroid bone and the floor of the left orbit; it then passed through the left anterior lobe of the cerebrum, and, in the median line, made its exit at the junction of the coronal and sagittal sutures, lacerating the longitudinal sinus, fracturing the parietal and frontal bones, and breaking up considerable of the brain; the globe of the left eye protruded nearly one-half of its diameter. The patient was thrown backward and gave a few convulsive movements of
As was most natural such a wonderful case of cerebral injury attracted much notice. Not only was the case remarkable in the apparent innocuous loss of cerebral substance, but in the singular chance which exempted the brain from either concussion or compression, and subsequent inflammation. Professor Bigelow examined the patient in January, 1850, and made a most excellent report of the case, [10.109] and it is due to his efforts that the case attained world-wide notoriety. Bigelow found the patient quite recovered in his faculties of body and mind, except that he had lost the sight of the injured eye. He exhibited a linear cicatrix one inch long near the angle of the ramus of the left lower jaw. His left eyelid was involuntarily closed and he had no power to overcome his ptosis. Upon the head, well covered by the hair, was a large unequal depression and elevation. In order to ascertain how far it might be possible for a bar of the size causing the injury to traverse the skull in the track assigned to it, Bigelow procured a common skull in which the zygomatic arches were barely visible from above, and having entered a drill near the left angle of the inferior maxilla, he passed it obliquely upward to the median line of the cranium just in front of the junction of the sagittal and coronal sutures. This aperture was then enlarged until it allowed the passage of the bar in question, and the loss of substance strikingly corresponded with the lesion said to have been received by the patient. From the coronoid process of the inferior maxilla there was removed a fragment measuring about 3/4 inch in length. This fragment, in the patient's case, might have been fractured and subsequently reunited. The iron bar, together with a cast of the patient's head, was placed in the Museum of the Massachusetts Medical College.
Bigelow appends an engraving (Fig. 194) to his paper. In the illustration the parts are as follows:—
(2) Front view of same.
(3) Plan of the base seen from within. In these three figures the optic foramina are seen to be intact and are occupied by small white rods.
(4) Cast taken from the shaved head of the patient representing the appearance of the fracture in 1850, the anterior fragment being considerably elevated in the profile view.
(5) The iron bar with length and diameter in proportion to the size of the other figures.
Heaton [10.110] reports a case in which, by an explosion, a tamping-iron was driven through the chin of a man into the cerebrum. Although there was loss of brain-substance, the man recovered with his mental faculties unimpaired.
A second case was that of a man who, during an explosion, was wounded in the skull. There was visible a triangular depression, from which, possibly, an ounce of brain-substance issued. This man also recovered.
Jewett mentions a case in which an injury somewhat similar to that in Bigelow's case was produced by a gas-pipe.
Among older writers, speaking of loss of brain-substance with subsequent recovery, Brasavolus saw as much brain evacuated as would fill an egg shell; the patient afterward had an impediment of speech and grew stupid. Franciscus Arcæus gives the narrative of a workman who was struck on the head by a stone weighing 24 pounds falling from a height. The skull was fractured; fragments of bone were driven into the brain. For three days the patient was unconscious and almost lifeless. After the eighth day a cranial
Mendenhall [10.111] reports the history of an injury to a laborer nineteen years old. While sitting on a log a few feet from a comrade who was chopping wood, the axe glanced and, slipping from the woodman's grasp, struck him just above the ear, burying the "bit'' of the axe in his skull. Two hours afterward he was seen almost pulseless, and his clothing drenched with blood which was still oozing from the wound with mixed brain-substance and fragments of bone. The cut was horizontal on a level with the orbit, 5 1/2 inches long externally, and, owing to the convex shape of the axe, a little less internally. Small spicules of bone were removed, and a cloth was placed on the battered skull to receive the discharges for the inspection of the surgeon, who on his arrival saw at least two tablespoonfuls of cerebral substance on this cloth. Contrary to all expectation this man recovered, but, strangely, he had a marked and peculiar change of voice, and this was permanent. From the time of the reception of the injury his whole mental and moral nature had undergone a pronounced change. Before the injury, the patient was considered a quiet, unassuming, and stupid boy, but universally regarded as honest. Afterward he became noisy, self-asserting, sharp, and seemingly devoid of moral sense or honesty. These new traits developed immediately, and more strikingly so soon as convalescence was established.
Bergtold [10.112] quotes a case reported in 1857 *[545] of extreme injury to the cranium and its contents. While sleeping on the deck of a canal boat, a man at Highspire was seriously injured by striking his head against a bridge. When seen by the surgeon his hair was matted and his clothes saturated with blood. There was a terrible gap in the scalp from the superciliary ridge to the occipital
Buchanan [10.113] mentions the history of a case in a woman of twenty-one, who, while working in a mill, was struck by a bolt. Her skull was fractured and driven into the brain comminuted. Hanging from the wound was a bit of brain-substance, the size of a finger,
composed of convolution as well as white matter. The wound healed, there was no hernia, and at the time of report the girl was conscious of no disturbance, not even a headache. There was nothing indicative of the reception of the injury except a scar near the edge of the hair on the upper part of the right side of the forehead. Steele, [10.114] in a school-boy of eight, mentions a case of very severe injury to the bones of the face and head, with escape of cerebral substance, and recovery. The injury was caused by falling into machinery.
There was a seaman aboard of the U. S. S. "Constellation,'' [10.115] who fell through a hatchway from the masthead, landing on the vertex of the head. There was copious bleeding from the ears, 50 to 60 fluid-ounces of blood oozing in a few hours, mingled with small fragments of brain-tissue. The next day the discharge became watery, and in it were found small pieces of true brain-substance.
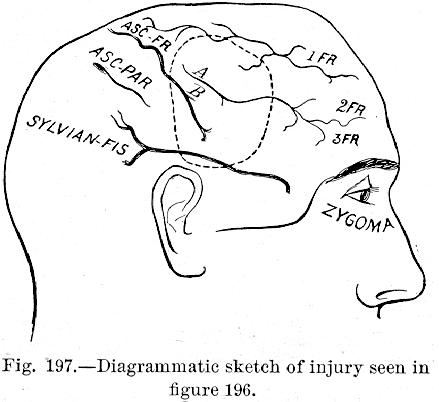
Cooke and Laycock [10.116] mention a case of intracranial injury with extensive destruction of brain-substance around the Rolandic area; there was recovery but with loss of the so called muscular sense. The patient, a workman of twenty-nine, while cutting down a gum-tree, was struck by a branch as thick as a man's arm, which fell from 100 feet overhead, inflicting a compound comminuted fracture of the cranium. The right eye was contused but the pupils equal; the vertex-wound was full of brain-substance and pieces of bone, ten of which were removed, leaving an oval opening four by three
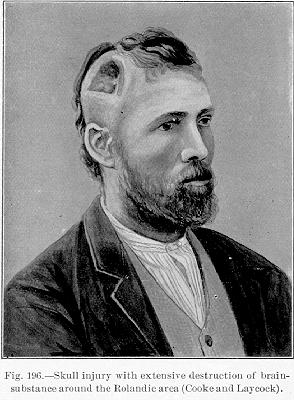
inches. The base of the skull was fractured behind the orbits; a fissure 1/4 inch wide was discernible, and the right frontal bone could be easily moved. The lacerated and contused brain-substance was removed. Consciousness returned six days after the operation. The accompanying illustrations (Figs. 196 and 197) show the extent of the injury. The lower half of the ascending frontal convolution, the greater half of the sigmoid gyrus, the posterior third of the lower and middle frontal convolutions, the base and posterior end of the upper convolution, and the base of the corresponding portion of the falciform lobe were involved. The sensory and motor functions of the arm were retained in a relative degree. There was power of simple movements, but complex movements were awkward. The tactile localization was almost lost.
There is the record [10.118] of a curious brain-injury in a man of twenty-two, who was struck on the skull by a circular saw. The saw cut directly down into the brain, severing the superior longitudinal sinus, besides tearing a branch of the meningeal artery. The wound was filled with sawdust left by the saw while it was tearing through the parts. After ordinary treatment the man recovered.
Bird [10.119] reports a compound comminuted fracture of the left temporal region, with loss of bone, together with six drams of brain-substance, which, however, was followed by recovery. Tagert [10.120] gives an instance of compound depressed fracture of the skull, with loss of brain-substance, in which recovery was effected without operative interference. Ballou, [10.121] Bartlett, [10.122] Buckner, Capon, [10.123] Carmichael, [10.124] Corban, [10.125] Maunder [10.126]
and many others, cite instances of cranial fracture and loss of brain-substance, with subsequent recovery. Halsted [10.127] reports the history of a boy of seventeen, who, while out fowling, had the breech-pin of a shot-gun blown out, the sharp point striking the forehead in the frontal suture, crushing the os frontis, destroying 1 3/4 inches of the longitudinal sinus, and causing severe hemorrhage from both the longitudinal and frontal sinuses. The pin was pulled out by the boy, who washed his own face, and lay down; he soon became semi-comatose, in which condition he remained for some days; but, after operation, he made complete recovery.
Loss of Brain-substance from Cerebral Tumor.—Koser is accredited with reporting results of a postmortem held on a young man of twenty who suffered from a cerebral tumor of considerable duration. It was stated that, although there was a cavity in the brain at least five inches
Extensive Fractures of the Skull. Jennings [10.128] mentions an instance of extensive fracture of the skull, 14 pieces of the cranium being found (Fig. 198). The patient lived five weeks and two days after the injury, the immediate cause of death being edema of the lungs. His language was incoherent and full of oaths. Belloste, in his "Hospital Surgeon,'' states that he had under has care a most dreadful case of a girl of eleven or twelve years, who received 18 or 19 cutlass wounds of the head, each so violent as to chip out pieces of bone; but, notwithstanding her severe injuries, she made recovery. At the Emergency Hospital in Washington, D. C., there was received a negress with at least six gaping wounds of the head, in some cases denuding the periosteum and cutting the cranium. During a debauch the night before
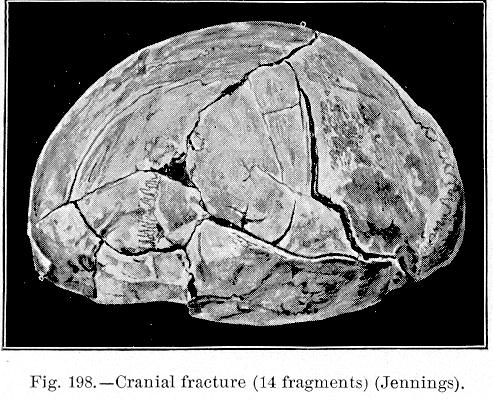
Fig. 198.—Cranial fracture (14 fragments) (Jennings).
[Description: Photograph of fractured skull]
she had been engaged in a quarrel with a negro with whom she lived, and was struck by him several times on the head with an axe. She lay all night unconscious, and was discovered the next morning with her hair and clothes and the floor on which she lay drenched with blood. The ambulance was summoned to take her to the morgue, but on the arrival of the police it was seen that feeble signs of life still existed. On admission to the hospital she was semi-comatose, almost pulseless, cold, and exhibiting all the signs of extreme hemorrhage and shock. Her head was cleaned up, but her condition would not permit of any other treatment than a corrosive-sublimate compress and a bandage of Scultetus. She was taken to the hospital ward, where warmth and stimulants were applied, after which she completely reacted. She progressed so well that it was not deemed advisable to remove the head-bandage until the fourth day, when it was seen that the wounds had almost entirely healed and suppuration was virtually absent. The patient rapidly and completely recovered, and her neighbors, on
A serious injury, which is not at all infrequent, is that caused by diving into shallow water, or into a bath from which water has been withdrawn. Curran [10.129] mentions a British officer in India who, being overheated, stopped at a station bath in which the previous night he had had a plunge, and without examining, took a violent "header'' into the tank, confidently expecting to strike from eight to ten feet of water. He dashed his head against the concrete bottom 12 feet below (the water two hours previously having been withdrawn) and crushed his brain and skull into an indistinguishable mass.
There are many cases on record in which an injury, particularly a gunshot wound of the skull, though showing no external wound, has caused death by producing a fracture of the internal table of the cranium. Paré *[618] gives details of the case of a nobleman whose head was guarded by a helmet and who was struck by a ball, leaving no external sign of injury, but it was subsequently found that there was an internal fracture of the cranium. Tulpius *[842] and Scultetus are among the older writers reporting somewhat similar instances, and there are several analogous cases reported as having occurred during the War of the Rebellion. Boling [10.130] reports a case in which the internal table was splintered to a much greater extent than the external.
Fracture of the base of the skull is ordinarily spoken of as a fatal injury, reported instances of recovery being extremely rare, but Battle, [10.131] in a paper on this subject, has collected numerous statistics of nonfatal fracture of the base of the brain, viz.:—
| Male. | Female. | ||
| Anterior fossa, | 16 | 5 | |
| Middle fossa, | 50 | 6 | |
| Posterior fossa, | 10 | 1 | |
| Middle and anterior fossæ, | 15 | 5 | |
| Middle and posterior fossæ, | 4 | 1 | |
| Anterior, middle, and posterior fossæ, | 1 | . | |
| — | — | ||
| 96 | 18 | Total, 114. |
In a paper on nonmortal fractures of the base of the skull, Lidell [10.132] gives an account of 135 cases. MacCormac [10.133] reports a case of a boy of nine who was run over by a carriage drawn by a pair of horses. He suffered fracture of the base of the skull, of the bones of the face, and of the left ulna, and although suppuration at the points of fracture ensued, followed by an optic neuritis, an ultimate recovery was effected. Ball, an Irish surgeon, has collected several instances in which the base of the skull has been driven in and the condyle of the jaw impacted in the opening by force transmitted through the lower maxilla.
The tolerance of foreign bodies in the brain is most marvelous. In the ancient chronicles of Kœnigsberg there is recorded the history of a man
Amatus Lusitanus *[119] speaks of a drunken courtesan who was wounded in a fray with a long, sharp-pointed knife which was driven into the head. No apparent injury resulted, and death from fever took place eight years after the reception of the injury. On opening the head a large piece of knife was found between the skull and dura. It is said that Benedictus mentions a Greek who was wounded, at the siege of Colchis, in the right temple by a dart and taken captive by the Turks; he lived for twenty years in slavery, the wound having completely healed. Obtaining his liberty, he came to Sidon, and five years after, as he was washing his face, he was seized by a violent fit of sneezing, and discharged from one of his nostrils a piece of the dart having an iron point of considerable length.
In about 1884 there died in the Vienna Hospital [10.134] a bookbinder of forty-five, who had always passed as an intelligent man, but who had at irregular intervals suffered from epileptic convulsions. An iron nail covered with rust was discovered in his brain; from the history of his life and from the appearances of the nail it had evidently been lodged in the cerebrum since childhood.
Slee [10.135] mentions a case in which, after the death of a man from septic peritonitis following a bullet-wound of the intestines, he found postmortem a knife-blade 5/16 inch in width projecting into the brain to the depth of one inch. The blade was ensheathed in a strong fibrous capsule 1/2 inch thick, and the adjacent brain-structure was apparently normal. The blade was black and corroded, and had evidently passed between the sutures during boyhood as there was no depression or displacement of the cranial bones. The weapon had broken off just on a level with the skull, and had remained in situ until the time of death without causing any indicative symptoms. Slee does not state the man's age, but remarks that he was a married man and a father at the time of his death, and had enjoyed the best of health up to the time he was shot in the abdomen. Callaghan, quoted in Erichsen's "Surgery,'' remarks that he knew of an officer who lived seven years with a portion of a gun-breech weighing three ounces lodged in his brain.
Lawson [10.136] mentions the impaction of a portion of a breech of a gun in the forehead of a man for twelve years, with subsequent removal and recovery. Waldon [10.137] speaks of a similar case in which a fragment of the breech weighing three ounces penetrated the cranium, and was lodged in the brain for two months previous to the death of the patient.
Pipe-stems, wires, shot, and other foreign bodies, are from time to time recorded as remaining in the brain for some time. Wharton [10.144] has compiled elaborate statistics on this subject, commenting on 316 cases in which foreign bodies were lodged in the brain, and furnishing all the necessary information to persons interested in this subject.
Injuries of the nose, with marked deformity, are in a measure combated by devices invented for restoring the missing portions of the injured member. Taliacotius, the distinguished Italian surgeon of the sixteenth century, devised an operation which now bears his name, and consists in fashioning a nose from the fleshy tissues of the arm. The arm is approximated to the head and held in this position by an apparatus or system of bandages for about ten days, at which time
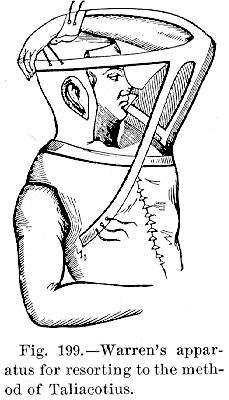
it is supposed that it can be severed, and further trimming and paring of the nose is then practiced. A column is subsequently made from the upper lip. In the olden days there was a timorous legend representing Taliacotius making noses for his patients from the gluteal regions of other persons, which statement, needless to say, is not founded on fact. Various modifications and improvements on the a Talicotian method have been made (Fig. 199); but in recent years the Indian method, introduced by Carpue into England in 1816, is generally preferred. Syme of Edinburgh, Wood, and Ollier have devised methods of restoring the nose, which bear their names.
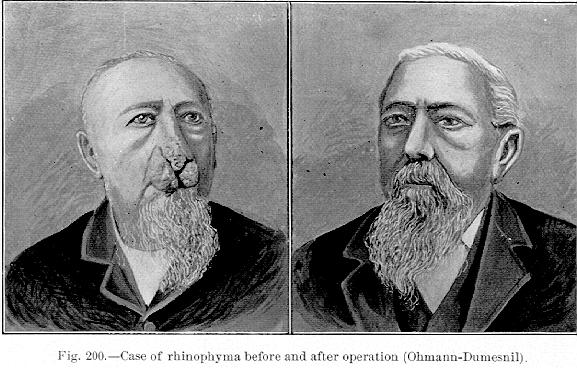
Ohmann-Dumesnil [10.145] reports a case of rhinophyma in a man of seventy-two, an alcoholic, who was originally affected with acne rosacea, on whom he performed a most successful operation for restoration. The accompanying
About 1892 Dr. J. P. Parker then of Kansas City, Mo., restored the missing bridge of a patient's nose by laying the sunken part open in two long flaps, denuding the distal extremity of the little finger of the patient's right hand of nail, flesh, tendons, etc., and binding it into the wound of the nose until firm union had taken place. The finger was then amputated at the second joint and the plastic operation completed, with a result pleasing both to patient and operator.
There is a case quoted [10.146] of a young man who, when first seen by his medical attendant, had all the soft parts of the nose gone, except one-third of the left ala
and a thin flap of the septum which was lying on the upper lip. The missing member was ferreted out and cleansed, and after an hour's separation sutured on. The nostrils were daily syringed with a corrosive sublimate solution, and on the tenth day the dressing was removed; the nose was found active and well, with the single exception of a triangular notch on the right side, which was too greatly bruised by the violence of the blow to recover. When we consider the varicosity of this organ we can readily believe the possibility of the foregoing facts, and there is little doubt that more precaution in suturing severed portions of the nose would render the operation of nose making a very rare one.
Maxwell [10.147] mentions a curious case of attempted suicide in which the ball, passing through the palatine process of the superior maxillary bone, crushing the vomer to the extent of its own diameter, fell back through the right nostril into the pharynx, was swallowed, and discharged from the anus.
Foreign bodies in the nose present phenomena as interesting as wounds of this organ. Among the living objects which have been found in the nose may be mentioned flies, maggots, worms, leeches, centipedes, and even lizards. Zacutus Lusitanus tells of a person who died in two days from the effects of a leech which was inadvertently introduced into the nasal fossa, and there is a somewhat similar case [10.149] of a military pharmacist, a member of the French army in Spain, who drank some water from a pitcher and exhibited, about a half hour afterward, a persistent hemorrhage from the nose. Emaciation progressively continued, although his appetite was normal. Three doctors, called in consultation, prescribed bleeding, which, however, proved of no avail. Three weeks afterward he carried in his nostril a tampon of lint, wet with an astringent solution, and, on the next day, on blowing his nose, there fell from the right nostril a body which he recognized as a leech. Healey [10.150] gives the history of four cases in which medicinal leeches were removed from the mouth and posterior nares of persons who had, for some days previously, been drinking turbid water. Sinclair [10.151] mentions the removal of a leech from the posterior nares.
Dempster [10.152] reports an instance of the lodgment of numerous live maggots within the cavity of the nose, causing sloughing of the palate and other complications. Nicholson [10.153] mentions a case of ulceration and abscess of the nostrils and face from which maggots were discharged. Jarvis [10.154] gives the history of a strange and repeated hemorrhage from the nose and adjacent parts that was found to be due to maggots from the ova of a fly, which had been deposited in the nose while the patient was asleep. Tomlinson [10.155] gives a case in which maggots traversed the Eustachian tube, some being picked out of the nostrils, while others were coughed up. Packard [10.156] records the accidental entrance of a centipede into the nostril. There is an account [10.157] of a native who was admitted to the Madras General Hospital, saying that a small lizard had crawled up his nose. The urine of these animals is very irritating, blistering any surface it touches. Despite vigorous treatment the patient died in consequence of the entrance of this little creature.
There have been instances among the older writers in which a pea has remained in the nose for such a length of time as to present evidences of sprouting. The Ephemerides renders an instance of this kind, and Breschet cites the history of a young boy, who, in 1718, introduced a pea into his nostril; in three days it had swollen to such an extent as to fill the whole passage. It could not be extracted by an instrument, so tobacco snuff was used, which excited sneezing, and the pea was ejected.
Vidal and the Ephemerides report several instances of tolerance of foreign bodies in the nasal cavities for from twenty to twenty-five years. Wiesman, in 1893, reported a rhinolith, which was composed of a cherry-stone enveloped in chalk, that had been removed after a sojourn of sixty years, with intense ozena as a consequence of its lodgment. Waring [10.158] mentions the case of a housemaid who carried a rhinolith, with a cherry-stone for a nucleus, which had been introduced twenty-seven years before, and which for twenty-five years had caused no symptoms. Grove [10.159] describes a necrosed inferior turbinated bone, to which was attached a coffee-grain which had been retained in the nostril for twenty years., Hickman [10.160] gives an instance of a steel ring which for thirteen and a half years had been impacted in the nasopharyngeal fossa of a child. It was detected by the rhinoscope and was removed. Parker [10.161] speaks of a gunbreech bolt which was removed from the
Howard [10.163] removed a large thimble from the posterior nares, although it had remained in its position for some time undetected. Eve reports a case in which a thimble was impacted in the right posterior nares. Gazdar [10.164] speaks, of a case of persistent neuralgia of one-half of the face, caused by a foreign body in the nose. The obstruction was removed after seven years' lodgment and the neuralgia disappeared. Molinier [10.165] has an observation on the extraction of a fragment of a knife-blade which had rested four years in the nasal fossæ, where the blade had broken off during a quarrel.
A peculiar habit, sometimes seen in nervous individuals, is that of "swallowing the tongue.'' Cohen claims that in some cases of supposed laryngeal spasm the tongue is swallowed, occluding the larynx, and sometimes with fatal consequences. There are possibly a half score of cases recorded, but this anomaly is very rare, and Major [10.166] is possibly the only one who has to a certainty demonstrated the fact by a laryngoscopic examination. By the laryngoscope he was enabled to observe a paroxysm in a woman, in which the tongue retracted and impinged on the epiglottis, but quickly recovered its position. Pettit mentions suffocation from "tongue swallowing,'' both with and without section of the frenum. Schobinger [10.167] cites a similar instance, due to loosening of the frenum.
Analogous to the foregoing phenomenon is the habit of "tongue sucking.'' Morris [10.168] mentions a young lady of fifteen who spontaneously dislocated her jaw, owing indirectly to this habit. Morris says that from infancy the patient was addicted to this habit, which was so audible as to be heard in all parts of the room. The continued action of the pterygoid muscles had so preternaturally loosened the ligaments and muscular structures supporting the joint as to render them unable to resist the violent action of "tongue sucking'' even during sleep.
Injuries to the Tongue.—Hobbs [10.169] describes a man of twenty-three who, while working, had a habit of protruding his tongue. One day he was hit under the chin by the chain of a crane on a pier, his upper teeth inflicting a wound two inches deep, three inches from the tip, and dividing the entire structure of the tongue except the arteries. The edges of the wound were brought into apposition by sutures, and after the removal of the latter perfect union and complete restoration of the sensation of taste ensued. Franck *[350] mentions regeneration of a severed tongue; and Van Wy has seen union of almost entirely severed parts of the tongue. De Fuisseaux [10.170] reports reunion of the tongue by suture after almost complete transverse division.
Articulation Without the Tongue.—Total or partial destruction of the tongue does not necessarily make articulation impossible. Banon [10.174] mentions a man who had nothing in his mouth representing a tongue. When he was young, he was attacked by an ulceration destroying every vestige of this member. The epiglottis, larynx, and pharynx, in fact the surrounding structures were normal, and articulation, which was at first lost, became fairly distinct, and deglutition was never interfered with. Paré gives a description of a man whose tongue was completely severed, in consequence of which he lost speech for three years, but was afterward able to make himself understood by an ingenious bit of mechanism. He inserted under the stump of the tongue a small piece of wood, in a most marvelous way replacing the missing member. Articulation with the absence of some constituent of the vocal apparatus has been spoken of on page 254.
Hypertrophy of the Tongue.—It sometimes happens that the tongue is so large that it is rendered not only useless but a decided hindrance to the performance of the ordinary functions into which it always enters. Ehrlich, Ficker, Klein, [10.175] Rodforffer, and the Ephemerides, all record instances in which a large tongue was removed either by ligation or amputation. Von Siebold [10.176] records an instance in which death was caused by the ligature of an abnormally sized tongue. There is a modern record of three cases of enormous tongues, the result of simple hypertrophy. [10.177] In one case the tongue measured 6 1/4 inches from the angle of the mouth about the sides and tip to the opposite angle, necessitating amputation of the protruding portion.
Carnochan [10.178] reports a case in which hypertrophy of the tongue was reduced to nearly the normal size by first tying the external carotid, and
The above conditions are known as macroglossia, which is a congenital hypertrophy of the tongue analogous to elephantiasis. It is of slow growth, and as the organ enlarges it interferes with deglutition and speech. It may protrude over the chin and reach even as far down as the sternum (Fig. 201).
The great enlargement may cause deformities of the teeth and lower jaw, and even present itself as an enormous tumor in the neck (Fig. 202). The protruding tongue itself may ulcerate,
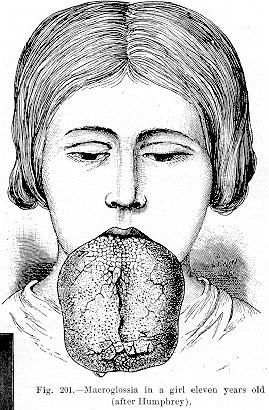
possibly bleed, and there is constant dribbling of saliva. The disease is probably due to congenital defect aggravated by frequent attacks of glossitis, and the treatment consists in the removal of the protruding portions by the knife, ligation, the cautery, or écraseur.
Living Fish in the Pharynx.— Probably the most interesting cases of foreign bodies are those in which living fish enter the pharynx and esophagus.
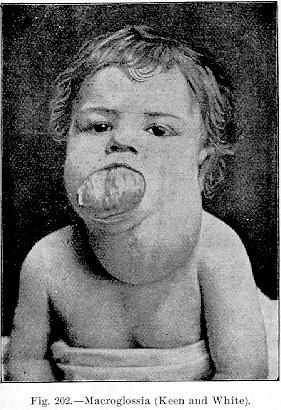
Chevers *[266] has collected five cases in which death was caused by living fish entering the mouth and occluding the air-passages. He has mentioned a case in which a large catfish jumped into the mouth of a Madras
A Leech in the Pharynx.—Granger, a surgeon in Her Majesty's Indian Service, [10.185] writes:—"Several days ago I received a note from the political sirdar, asking me if I would see a man who said he had a leech in his throat which he was unable to get rid of. I was somewhat sceptical, and thought that possibly the man might be laboring under a delusion. On going outside the fort to see the case, I found an old Pathan graybeard waiting for me. On seeing me, he at once spat out a large quantity of dark, half-clotted blood to assure me of the serious nature of his complaint. His history—mostly made out with the aid of interpreters—was that eleven days ago he was drinking from a rain-water tank and felt something stick in his throat, which he could not reject. He felt this thing moving, and it caused difficulty in swallowing, and occasionally vomiting. On the following day he began to spit up blood, and this continued until he saw me. He stated that he once vomited blood, and that he frequently felt that he was going to choke.
On examining his throat, a large clot of blood was found to be adherent to the posterior wall of the pharynx. On removing this clot of blood, no signs of the presence of a leech could be detected. However, on account of the symptoms complained of by the patient I introduced a polypus forceps
Foreign Bodies in the Pharynx and Esophagus.—Aylesbury [10.186] mentions a boy who swallowed a fish-hook while eating gooseberries. He tried to pull it up, but it was firmly fastened, and a surgeon was called. By ingeniously passing a leaden bullet along the line, the weight of the lead loosened the hook, and both bullet and hook were easily drawn up. Babbit and Battle [10.187] report an ingenious method of removing a piece of meat occluding the esophagus—the application of trypsin. Henry [10.188] speaks of a German officer who accidentally swallowed a piece of beer bottle, 3/8 x 1/8 inch, which subsequently penetrated the esophagus, and in its course irritated the recurrent laryngeal and vagi, giving rise to the most serious phlegmonous inflammation and distressing respiratory symptoms. A peculiar case [10.189] is that of the man who died after a fire at the Eddystone Lighthouse. He was endeavoring to extinguish the flames which were at a considerable distance above his head, and was looking up with his mouth open, when the lead of a melting lantern dropped down in such quantities as not only to cover his face and enter his mouth, but run over his clothes. The esophagus and tunica in the lower part of the stomach were burned, and a great piece of lead, weighing over 7 1/2 ounces, was taken from the stomach after death.
Evans [10.190] relates the history of a girl of twenty-one who swallowed four artificial teeth, together with their gold plate; two years and eight days afterward she ejected them after a violent attack of retching. Gauthier [10.191] speaks of a young girl who, while eating soup, swallowed a fragment of bone. For a long time she had symptoms simulating phthisis, but fourteen years afterward the
Instances of migration of foreign bodies from the esophagus are repeatedly recorded. There is an instance [10.193] of a needle which was swallowed and lodged in the esophagus, but twenty-one months afterward was extracted by an incision at a point behind the right ear. Kerckring speaks of a girl who swallowed a needle which was ultimately extracted from the muscles of her neck. Poulet *[641] remarks that Vigla has collected the most interesting of these cases of migration of foreign bodies. Hévin mentions several cases of grains of wheat abstracted from abscesses of the thoracic parietes, from thirteen to fifteen days after ingestion. Bonnet and Helmontius have reported similar facts. Volgnarius has seen a grain of wheat make its exit from the axilla, and Polisius mentions an abscess of the back from which was extracted a grain of wheat three months after ingestion. Bally [10.194] reports a somewhat similar instance, in which, three months after ingestion, during an attack of peripneumonia, a foreign body was extracted from an abscess of the thorax, between the 2d and 3d ribs. Ambrose [10.195] found a needle encysted in the heart of a negress. She distinctly stated that she had swallowed it at a time calculated to have been nine years before her death. Planque speaks of a small bone perforating the esophagus and extracted through the skin.
Abscess or ulceration, consequent upon periesophagitis, caused by the lodgment of foreign bodies in the esophagus, often leads to the most serious results. There is an instance *[662] of a soldier who swallowed a bone while eating soup, who died on the thirty-first day from the rupture internally of an esophageal abscess. Grellois [10.196] has reported the history of a case of a child twenty-two months old, who suffered for some time with impaction of a small bone in the esophagus. Less than three months afterward the patient died with all the symptoms of marasmus, due to difficult deglutition, and at the autopsy an abscess was seen in the posterior wall of the pharynx, opposite the 3d cervical vertebra; extensive caries was also noticed in the bodies of the 2d, 3d, and 4th cervical vertebræ. Guattani [10.197] mentions a curious instance in which a man playing with a chestnut threw it in the air, catching it in his
A peculiarly fatal accident in this connection is that in which a foreign body in the esophagus ulcerates, and penetrates one of the neighboring major vessels. Colles [10.198] mentions a man of fifty-six who, while eating, perceived a sensation as of a rent in the chest. The pain was augmented during deglutition, and almost immediately afterward he commenced to expectorate great quantities of blood. On the following day he vomited a bone about an inch long and died on the same day. At the autopsy it was found that there was a rent in the posterior wall of the esophagus, about 1/2 inch long, and a corresponding wound of the aorta. There was blood in the pleura, pericardium, stomach, and intestines. There is one case in which a man of forty-seven suddenly died, after vomiting blood, and at the autopsy it was demonstrated that a needle had perforated the posterior wall of the esophagus and wounded the aorta. [10.199] Poulet has collected [10.200] 31 cases in which ulceration caused by foreign bodies in the esophagus has resulted in perforation of the walls of some of the neighboring vessels. The order of frequence was as follows: aorta, 17; carotids, four; vena cava, two; and one case each of perforation of the inferior thyroid artery, right coronary vein, demi-azygos vein, the right subclavicular artery (abnormal), and the esophageal artery. In three of the cases collected there was no autopsy and the vessel affected was not known.
In a child of three years that had swallowed a half-penny, Atkins [10.201] reports rupture of the innominate artery. No symptoms developed, but six weeks later, the child had an attack of ulcerative stomatitis, from which it seemed to be recovering nicely, when suddenly it ejected two ounces of bright red blood in clots, and became collapsed out of proportion to the loss of blood. Under treatment, it rallied somewhat, but soon afterward it ejected four ounces more of blood and died in a few minutes. At the autopsy 3/4 pint of blood was found in the stomach, and a perforation was discovered on the right side of the esophagus, leading into a cavity, in which a blackened half-penny was found. A probe passed along the aorta into the innominate protruded into the same cavity about the bifurcation of the vessel.
Denonvilliers has described a perforation of the esophagus and aorta by a five-franc piece. A preserved preparation of this case, showing the coin in situ, is in the Musée Dupuytren (Fig. 203). Blaxland [10.202] relates the instance of a woman of forty-five who swallowed a fish bone, was seized with violent hematemesis, and died in eight hours. The necropsy revealed a penetration of the aorta through the thoracic portion of the esophagus. There is also in the Musée Dupuytren a preparation described by Bousquet, in which the aorta and the esophagus were perforated by a very irregular piece of bone
In some cases penetration of the esophagus allows the further penetration of some neighboring membrane or organ in the same manner as the foregoing cases. Dudley [10.203] mentions a case in which fatal hemorrhage was caused by penetration of the esophagus and lung by a chicken-bone. Buist [10.204] speaks of a patient who swallowed two artificial teeth. On the following day there was pain in the epigastrium, and by the fourth day the pain extended to the vertebræ, with vomiting, delirium, and death on the fifth day. At the autopsy it was found that a foreign body, seven cm. long had perforated the


pericardium, causing a suppurative pericarditis. Dagron *[242] reports a unique instance of death by purulent infection arising from perforation of the esophagus by a pin. The patient was a man of forty-two, and, some six weeks before he presented himself for treatment, before swallowing had experienced a severe pain low down in the neck. Five days before admission he had had a severe chill, followed by sweating and delirium. He died of a supraclavicular abscess on the fifth day; a black steel pin was found against the esophagus and trachea.
In connection with foreign bodies in the esophagus, it might be interesting
Injuries of the neck are usually inflicted with suicidal intent or in battle. Cornelius Nepos says that while fighting against the Lacedemonians, Epaminondas was sensible of having received a mortal wound, and apprehending that the lance was stopping a wound in an important vessel, remarked that he would die when it was withdrawn. When he was told that the Bœotians had conquered, exclaiming "I die unconquered,'' he drew out the lance and perished. Petrus de Largenta speaks of a man with an arrow in one of his carotids, who was but slightly affected before its extraction, but who died immediately after the removal of the arrow. Among the remarkable recoveries from injuries of the neck is that mentioned by Boerhaave, of a young man who lived nine or ten days after receiving a sword-thrust through the neck between the 4th and 5th vertebræ, dividing the vertebral artery. Benedictus, Bonacursius, and Monroe, all mention recovery after cases of cut-throat in which the esophagus as well as the trachea was wounded, and food protruded from the external cut. Warren [10.207] relates the history of a case in which the vertebral artery was wounded by the discharge of a pistol loaded with pebbles. The hemorrhage was checked by compression and packing, and after the discharge of a pebble and a piece of bone from the wound, the man was seen a month afterward in perfect health. Corson of Norristown, Pa., has reported the case of a quarryman who was stabbed in the neck with a shoemaker's knife, severing the left carotid one inch below its division. He was seen thirty minutes later in an apparently lifeless condition, but efforts at resuscitation were successfully made. The hemorrhage ceased spontaneously, and at the time of report, the man presented the symptoms of one who had had his carotid ligated (facial atrophy on one side, no pulse, etc.). Baron Larrey *[478] mentions a case of gunshot wound in which the carotid artery was open at its division into internal and external branches, and says that the wound was plugged by an artilleryman until ligation, and in this primitive manner the patient was saved. Sale [10.208] reports the case of a girl of nineteen, who fell on a china bowl that she had shattered, and wounded both the right common carotid artery and internal jugular vein. There was profuse and continuous hemorrhage for a time, and subsequently a false aneurysm developed, which ruptured in about three months, giving rise to enormous momentary hemorrhage; notwithstanding the severity of the injury and the extent of the hemorrhage, complete recovery ensued. Amos [10.209] relates the instance of a woman named Mary Green who, after complete division of all the vessels of the neck, walked 23 yards and climbed over an ordinary bar-gate nearly four feet high.
Relative to ligature of the common carotid artery, Ashhurst mentions the fact that the artery has been ligated in 228 instances, with 94 recoveries. Ellis [10.211] mentions ligature of both carotids in four and a half days, as a treatment for a gunshot wound, with subsequent recovery. Lewtas [10.212] reports a case of ligation of the innominate and carotid arteries for traumatic aneurysm (likely a hematoma due to a gunshot injury of the subclavian artery). The patient was in profound collapse, but steadily reacted and was discharged cured on the forty-fifth day, with no perceptible pulse at the wrist and only a feeble beat in the pulmonary artery.
Garengeot, Wirth, Fine, and Evers, all mention perforating wounds of the trachea and esophagus with recoveries. Van Swieten and Hiester mention cases in which part of the trachea was carried away by a ball, with recovery. Monro, Tulpius, Bartholinus, and Paré report severance of the trachea with the absence of oral breathing, in which the divided portions were sutured, with successful results. In his "Theatro Naturæ,'' Bodinus says that William, Prince of Orange, lost the sense of taste after receiving a wound of the larynx; according to an old authority, a French soldier became mute after a similar accident. Davies-Colley [10.213] mentions a boy of eighteen who fell on a stick about the thickness of the index finger, transfixing his neck from right to left; he walked to a doctor's house, 250 yards away, with the stick in situ. In about two weeks he was discharged completely well. During treatment he had no hemorrhage of any importance, and his voice was not affected, but for a while he had slight dysphagia.
Barker [10.214] gives a full account of a barber who was admitted to a hospital two and a half hours after cutting his throat. He had a deep wound running transversely across the neck, from one angle of the jaw to the other, cutting open the floor of the mouth and extending from the inner border of the sternocleidomastoid to the other, leaving the large vessels of the neck untouched. The razor had passed through the glosso-epiglottidean fold, a tip of the epiglottis, and through the pharynx down to the spinal column. There was little hemorrhage, but the man could neither swallow nor speak. The wound was sutured, tracheotomy done, and the head kept fixed on the chest by a copper splint. He was ingeniously fed by esophageal tubes and rectal enemata; in three weeks speech and deglutition were restored. Shortly afterward the esophageal tube was removed and recovery was virtually complete. Little [10.215] mentions an extraordinary case of a woman of thirty-six who was discharged
Hislop [10.216] records a case of cut-throat in a man of seventy-four. He had a huge gaping wound of the neck, extending to within a half inch of the carotids on each side. The trachea was almost completely severed, the band left was not more than 1/4 inch wide. Hislop tied four arteries, brought the ends of the trachea together with four strong silk sutures, and, as the operation was in the country, he washed the big cavity of the wound out with cold spring-water. He brought the superficial surfaces together with ten interrupted sutures, and, notwithstanding the patient's age, the man speedily recovered. This emphasizes the fact that the old theory of leaving wounds of this nature open was erroneous. Solly [10.217] reports the case of a tailor of twenty-two who attempted suicide by cutting through the larynx, entirely severing the epiglottis and three-fourths of the pharynx. No bleeding point was found, and recovery ensued.
Cowles [10.218] describes the case of a soldier of thirty-five who, while escaping from the patrols, was shot by the Officer of the Day with a small bullet from a pistol. The ball entered the right shoulder, immediately over the suprascapular notch, passed superficially upward and forward into the neck, wounding the esophagus posteriorly at a point opposite the thyroid cartilage, and lodged in the left side of the neck. The patient had little hemorrhage, but had expectorated and swallowed much blood. He had a constant desire to swallow, which continued several days. The treatment was expectant; and in less than three weeks the soldier was returned to duty. From the same authority there is a condensation of five reports of gunshot wounds of the neck, from all of which the patients recovered and returned to duty.
Braman [10.219] describes the case of a man on whom several injuries were inflicted by a drunken companion. The first wound was slight; the second a deep flesh-wound over the trapezius muscle; the third extended from the right sterno-cleido-mastoid midway upward to the middle of the jaw and down to the rapine of the trachea. The external jugular, the external thyroid, and the facial arteries were severed. Braman did not find it necessary to ligate, but was able to check the hemorrhage with lint and persulphate of iron, in powder, with pressure. After fourteen hours the wound was closed; the patient recovered, and was returned to duty in a short time.
Adams [10.221] describes the case of a woman who attempted suicide with a common table-knife, severing the thyroid, cricoid, and first three rings of the trachea, and lacerating the sternohyoid and thyroid arteries; she finally recovered.
There is a curious case of suicide [10.222] of a woman who, while under the effects of opium, forced the handle of a mirror into her mouth. From all appearances, the handle had broken off near the junction and she had evidently fallen forward with the remaining part in her mouth, driving it forcibly against the spine, and causing the point of the handle to run downward in
Injuries of the cervical vertebræ, while extremely grave, and declared by some authors to be inevitably fatal, are, however, not always followed by death or permanently bad results. Barwell [10.224] mentions a man of sixty-three who, in a fit of despondency, threw himself from a window, having fastened a rope to his neck and to the window-sill. He fell 11 or 12 feet, and in doing so suffered a subluxation of the 4th cervical vertebra. It slowly resumed the normal position by the elasticity of the intervertebral fibrocartilage, and there was complete recovery in ten days. Lazzaretto [10.225] reports the history of the case of a seaman whose atlas was dislocated by a blow from a falling sail-yard. The dislocation was reduced and held by adhesive strips, and the man made a good recovery. Vanderpool of Bellevue Hospital, N. Y., [10.226] describes a fracture of the odontoid process caused by a fall on the back of the head; death, however, did not ensue until six months later. According to Ashhurst, [10.227] Philips, the elder Cline, Willard Parker, Bayard, Stephen Smith, May, and several other surgeons, have recorded complete recovery after fracture of the atlas and axis. The same author also adds that statistic investigation shows that as large a proportion as 18 per cent. of injuries of the cervical vertebræ occurring in civil practice, recover. However, the chances of a fatal issue in injuries of the vertebræ vary inversely with the distance of the point of injury from the brain. Keen has recorded a case in which a conoidal ball lodged in the body of the third cervical vertebra, from which it was extracted six weeks later. The paralysis, which, up to the time of extraction, had affected all four limbs, rapidly diminished. In about five weeks after the removal of the bullet nearly the entire body of the 3d cervical vertebra, including the anterior half of the transverse process and vertebral foremen, was spontaneously discharged. Nearly eight years afterward Keen saw the man still living, but with his right shoulder and arm diminished in size and partly paralyzed.
Doyle [10.228] reports a case of dislocated neck with recovery. During a runaway the patient was thrown from his wagon, and was soon after found on the roadside apparently dead. Physicians who were quickly summoned from the immediate neighborhood detected faint signs of life; they also found a deformity of the neck, which led them to suspect dislocation. An ambulance was called, and without any effort being made to relieve the deformity the man was placed in it and driven to his home about a mile distant. The jolting
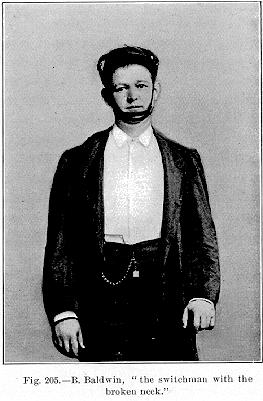
went on without development of any serious symptoms. At the time of report he appeared in the best of health and was quite able to attend to his daily avocations. Doyle appends to his report the statement that among 394 cases embraced in Ashhurst's statistics, in treatment of dislocations in the cervical region, the mortality has been nearly four times greater when constitutional or general treatment has been relied on exclusively than when attempts had been made to reduce the dislocation by extension, rotation, etc. Doyle strongly advocates attempts at reduction in such cases.
Figure 205 represents a photograph of Barney Baldwin, a switchman of the Louisville and Nashville Railroad, who, after recovery from cervical dislocation, exhibited himself about the country, never appearing without his suspensory apparatus.
According to Thorburn, [10.230] Hilton had a patient who lived fourteen years with paraplegia due to fracture of the 5th, 6th, and 7th cervical vertebræ. Shaw is accredited with a case in which the patient lived fifteen months, the fracture being above the 4th cervical vertebra.
In speaking of foreign bodies in the larynx and trachea, the first to be considered will be liquids. There is a case on record [10.231] of an infant who was eating some coal, and being discovered by its mother was forced to rapidly swallow some water. In the excitement, part of the fluid swallowed fell into the trachea, and death rapidly ensued. It is hardly necessary to mention the instances in which pus or blood from ruptured abscesses entered the trachea and caused subsequent asphyxiation. A curious instance is
The presence of a foreign body in the larynx is at all times the cause of distressing symptoms, and, sometimes, a substance of the smallest size will cause death. There is a curious accident recorded [10.233] that happened to a young man of twenty-three, who was anesthetized in order to extract a tooth. A cork had been placed between the teeth to keep the mouth open. The tooth was extracted but slipped from the forceps, and, together with the cork, fell into the pharynx. The tooth was ejected in an effort at vomiting, but the cork entered the larynx, and, after violent struggles, asphyxiation caused death in an hour. The autopsy demonstrated the presence of the cork in the larynx. A somewhat analogous case, though not ending fatally, was reported by Hertz [10.234] of a woman of twenty-six, who was anesthetized for the extraction of the right second inferior molar. The crown broke off during the operation, and immediately after the extraction she had a fit of coughing. About fifteen days later she experienced pain in the lungs. Her symptoms increased to the fifth week, when she became so feeble as to be confined to her bed. A body seemed to be moving in the trachea, synchronously with respiration. At the end of the fifth week the missing crown of the tooth was expelled after a violent fit of coughing; the symptoms immediately ameliorated, and recovery was rapid thereafter. Aronsohn [10.235] speaks of a child who was playing with a toy wind-instrument, and in his efforts to forcibly aspirate air through it, the child drew the detached reed into the respiratory passages, causing asphyxiation. At the autopsy the foreign body was found at the superior portion of the left bronchus. There are other cases in which, while sucking oranges or lemons, seeds have been aspirated; and there is a case in which, in a like manner, the claw of a crab was drawn into the air-passages. There are two cases mentioned [10.236] in which children playing with toy balloons, which they inflated with their breath, have, by inspiration, reversed them and
A curious accident is that in which a foreign body thrown into the air and caught in the mouth has caused immediate asphyxiation. Suetonius *[754] transmits the history of a young man, a son of the Emperor Claudius, who, in sport, threw a small pear into the air and caught it in his mouth, and, as a consequence, was suffocated. Guattani *[563] cites a similar instance of a man who threw up a chestnut, which, on being received in the mouth, lodged in the air-passages; the man died on the nineteenth day. Brodie reported the classic observation of the celebrated engineer, Brunel, who swallowed a piece of money thrown into the air and caught in his mouth. It fell into the open larynx, was inspired, causing asphyxiation, but was removed by inversion of the man's body.
Sennert says that Pope Adrian IV. died from the entrance of a fly into his respiratory passages; and Remy and Gautier record instances of the penetration of small fish into the trachea. There are, again, instances of leeches in this location.
Occasionally the impaction of artificial teeth in the neighborhood of the larynx has been unrecognized for many years. Lennox Browne [10.237] reports the history of a woman who was supposed to have either laryngeal carcinoma or phthisis, but in whom he found, impacted in the larynx, a plate with artificial teeth attached, which had remained in this position twenty-two months unrecognized and unknown. The patient, when questioned, remembered having been awakened in the night by a violent attack of vomiting, and finding her teeth were missing assumed they were thrown away with the ejections. From that time on she had suffered pain and distress in breathing and swallowing, and became the subject. of progressive emaciation. After the removal of the impacted plate and teeth she soon regained her health. Paget [10.238] speaks of a gentleman who for three months, unconsciously, carried at the base of the tongue and epiglottis, very closely fitted to all the surface on which it rested, a full set of lost teeth and gold palate-plate. From the symptoms and history it was suspected that he had swallowed his set of false teeth, but, in order to prevent his worrying, he was never informed of this suspicion, and he never once suspected the causes of his symptoms.
Wrench [10.239] mentions a case illustrative of the extent to which imagination
There is a curious case of a man drowned near Portsmouth. [10.240] After the recovery of his body it was seen that his false teeth were impacted at the anterior opening of the glottis, and it was presumed that the shock caused by the plunge into the cold water had induced a violent and deep inspiration which carried the teeth to the place of impaction.
Perrin [10.241] reports a case of an old man of eighty-two who lost his life from the impaction of a small piece of meat in the trachea and glottis. In the Musée Valde-Grâce is a prepared specimen of this case showing the foreign body in situ (Fig. 206). In the same museum Perrin has also deposited a preparation from the body of a man of sixty-two, who died from the entrance of a morsel of beef into the respiratory passages.

Fig. 206.—Foreign body in
trachea and glotis.
[Description: Drawing of blocked trachea]
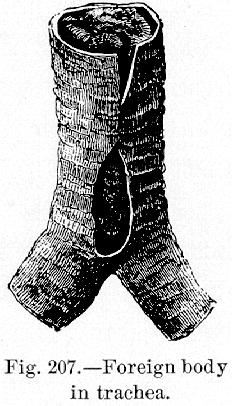
Fig. 207.—Foreign body
in trachea.
[Description: Drawing of blocked trachea]
At the postmortem a mobile mass of food about the size of a hazel-nut was found at the base of the larynx at the glossoepiglottic fossa. About the 5th ring of the trachea the caliber of this organ was obstructed by a cylindric alimentary bolus about six inches long, extending almost to the bronchial division (Fig. 207). Ashhurst shows a fibrinous cast, similar to that found in croup, caused by a foreign body removed by Wharton, together with a shawl-pin, from a patient at the Children's Hospital seven hours after the performance of tracheotomy. Search for the foreign body at the time of the operation was prevented by profuse hemorrhage.
The ordinary instances of foreign bodies in the larynx and trachea are so common that they will not be mentioned here. Their variety is innumerable and it is quite possible for more than two to be in the same location simultaneously. In his treatise on this subject Gross says that he has seen two, three, and even four substances simultaneously or successively penetrate the
The Medical Press and Circular [10.243] finds in an Indian contemporary some curious instances of misapplied ingenuity on the part of certain habitual criminals in that country. The discovery on a prisoner of a heavy leaden bullet about 3/4 inch in diameter led to an inquiry as to the object to which it was applied. It was ascertained that it served to aid in the formation of a pouch-like recess at the base of the epiglottis. The ball is allowed to slide down to the desired position, and it is retained there for about half an hour at a time. This operation is repeated many times daily until a pouch the desired size results, in which criminals contrive to secrete jewels, money, etc., in such a way as to defy the most careful search, and without interfering in any way with speech or respiration. Upward of 20 prisoners at Calcutta were found to be provided with this pouch-formation. The resources of the professional malingerer are exceedingly varied, and testify to no small amount of cunning. The taking of internal irritants is very common, but would-be in-patients very frequently overshoot the mark and render recovery impossible. Castor-oil seeds, croton beans, and sundry other agents are employed with this object in view, and the medical officers of Indian prisons have to be continually on the lookout for artificially induced diseases that baffle diagnosis and resist treatment. Army surgeons are not altogether unfamiliar with these tricks, but compared with the artful Hindoos the British soldier is a mere child in such matters.
Excision of the larynx has found its chief indication in carcinoma, but has been employed in sarcoma, polyp), tuberculosis, enchondroma, stenosis, and necrosis. Whatever the procedure chosen for the operation, preliminary tracheotomy is a prerequisite. It should be made well below the isthmus of the thyroid gland, and from three to fifteen days before the laryngectomy. This affords time for the lungs to become accustomed to the new manner of breathing, and the trachea becomes fixed to the anterior wall of the neck.
Powers and White [10.244] have gathered 69 cases of either total or partial extirpation of the larynx, to which the 240 cases collected and analyzed by Eugene Kraus, in 1890, have been added. The histories of six new cases are given. Of the 309 operations, 101, or 32 per cent. of the patients, died within the first eight weeks from shock, hemorrhage, pneumonia, septic infection, or exhaustion. The cases collected by these authors show a decrease in the death ratio in the total excision,—29 per cent. as against 36 per cent. in the Kraus tables. The mortality in the partial operation is increased, being 38 per cent. as opposed to 25 per cent. Cases reported as free from the disease before the lapse of three years are of little value, except in that they diminish, by so much, the operative death-rate. Of 180 laryugectomies for carcinoma prior to January 1, 1892, 72, or 40 per cent., died as a result of the operation; 51 of
Injuries destroying great portions of the face or jaw, but not causing death, are seldom seen, except on the battle-field, and it is to military surgery that we must look for the most striking instances of this kind. Ribes [10.245] mentions a man of thirty-three who, in the Spanish campaign in 1811, received an injury which carried away the entire body of the lower jaw, half of each ramus, and also mangled in a great degree the neighboring soft parts. He was transported from the field of battle, and, despite enormous hemorrhage and suppuration, in two months recovered. At the time of report the wounded man presented no trace of the inferior maxillary bone, but by carrying the finger along the side of the pharynx in the direction of the superior dental arch the coronoid apophyses could be recognized, and about six lines nearer the temporal extremity the ramus could be discovered. The tongue was missing for about one-third its length, and was thicker than natural and retracted on the hyoid bone. The sublingual glands were adherent to the under part of the tongue and were red and over-developed. The inferior parts of the cheeks were cicatrized with the lateral and superior regions of the neck, and with the base of the tongue and the hyoid bone. The tongue was free under and in front of the larynx. The patient used a gilded silver plate to fix the tongue so that deglutition could be carried on. He was not able to articulate sounds, but made himself understood through the intervention of this plate, which was fixed to a silver chin. The chin he used to maintain the tongue-plate, to diminish the deformity, and to retain the saliva, which was constantly dribbling on the neck (Fig. 208). The same author quotes the instance of a man of fifty, who, during the siege of Alexandria in 1801, was struck in the middle of his face, obliquely, by a cannonball, from below upward and from right to left. A part of the right malar bone, the two superior maxillary bones, the nasal bones, the cartilage, the vomer, the middle lamina of the ethmoid, the left maxillary bone, a portion of the left zygomatic arch, and a great portion of the inferior maxilla were carried away, or comminuted, and all the soft parts correspondingly lacerated. Several hours afterward this soldier was counted among the number of dead, but Larrey, the surgeon-in-chief of the army, with his typical vigilance and humanity, remarked that the patient gave signs of life, and that, despite the magnitude of his wound, he did not despair of his recovery. Those portions in which attrition was very great were removed, and the splinters of bone taken out, showing an enormous wound. Three months were
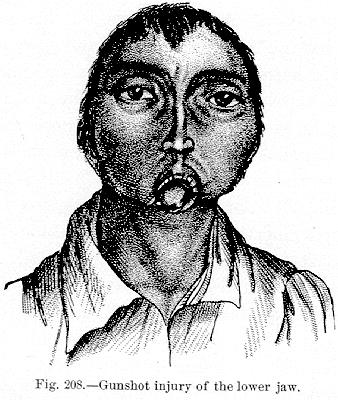
Fig. 208.—Gunshot injury of the lower jaw.
[Description: Drawing of man with injured jaw]

Fig. 209.—Gunshot injury of the face.
[Description: Drawing of gunshot wound of the face]
analogous instance of a gunner who had his whole lower jaw torn away by a shell, but who recovered and used an ingenious contrivance in the shape of a silver mask for remedying the loss of the parts. Steiner [10.247] mentions a wound from a cannon-ball, which carried away the left half of the inferior maxilla, stripping the soft parts as high as the malar, and on the left side of the neck to within 1 1/2 inches of the clavicle, laying bare the transverse processes of the 2d and 3d vertebræ, end exposing the external carotid and most of its branches.
It sometimes happens that a foreign body, such as the breech of a gun, may be imbedded for some time in the face, with subsequent safe removal. Keith [10.248] mentions an instance of the successful removal of the breech of a fowling-piece from the face, at the root of the nose, after a lodgment of four months; and Fraser [10.249] cites an analogous instance in which the breech
Before leaving accidents to the head and neck, a most curious case, cited by O'Neill, [10.251] will be briefly reviewed. A boy of twelve was entrusted to carry a new iron pot to the destination of its purchaser. Probably to facilitate transportation, the boy removed his hat and placed the pot obliquely on the back part of his head, but a sudden movement caused it to slip forward and downward over the head. Unavailing efforts were made at the time and after he reached home, to remove the pot from his head, but in vain, and he continued all the night greatly prostrated by fright, hunger, and thirst, together with the efforts at removal. The next morning he was taken to a neighboring blacksmith, who, by greasing one of his fingers, managed to insinuate it between the head and pot. Placing the other side of the pot against an anvil he struck over the location of his finger a quick, heavy tap with a hammer, and the pot fell to pieces. The little patient was much exhausted by all his treatment and want of sleep, and, in fact, could hardly have endured his situation much longer.
| CHAPTER X.
SURGICAL ANOMALIES OF THE HEAD AND
NECK. Anomalies and Curiosities of Medicine | ||