| CHAPTER XV.
ANOMALOUS TYPES AND INSTANCES OF
DISEASE. Anomalies and Curiosities of Medicine | ||
15. CHAPTER XV.
ANOMALOUS TYPES AND INSTANCES OF
DISEASE.
Tumors.—In discussing tumors and similar growths no attempt will be made to describe in detail the various types. Only the anomalous instances or examples, curious for their size and extent of involvement, will be mentioned. It would be a difficult matter to decide which was the largest tumor ever reported. In reviewing literature so many enormous growths are recorded that but few can be given here. Some of the large cystic formations have already been mentioned; these are among the largest tumors. Scrotal tumors are recorded that weighed over 200 pounds; and a limb affected with elephantiasis may attain an astonishing size. Delamater is accredited with a report of a tumor that weighed 275 pounds, the patient only weighing 100 pounds at death. [15.1] Benign tumors will be considered first.
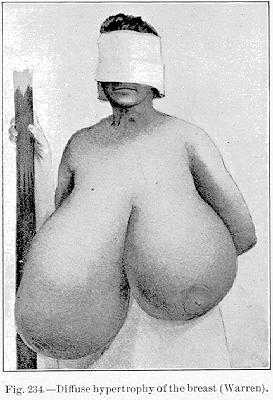
Pure adenoma of the breast is a rare growth. Gross was able to collect but 18 examples; but closely allied to this condition is what is known as diffuse hypertrophy of the breast. In some parts of the world, particularly in India and Africa, long, dependent breasts are signs of beauty. On the other hand we learn from Juvenal and Martial that, like ourselves, the Greeks detested pendant and bulky breasts, the signs of beauty being elevation, smallness, and regularity of contour. In the Grecian images of Venus the breasts are never pictured as engorged or enlarged. The celebrated traveler Chardin says that the Circassian and Georgian women have the most beautiful breasts in the world; in fact the Georgians are so jealous of the regular contour and wide interval of separation of their breasts that they refuse to nourish their children in the natural manner.
The amount of hypertrophy which is sometimes seen in the mammæ is extraordinary. Borellus *[841] remarks that he knew of a woman of ordinary size, each of whose mammæ weighed about 30 pounds, and she supported them in bags hung about her neck. Durston [15.2] reports a case of sudden onset of hypertrophy of the breast causing death. At the postmortem it was found that the left breast weighed 64 pounds and the right 40 pounds. Boyer successfully removed two breasts at an interval of twenty-six days between the two operations. The mass excised was one-third of the total body-weight.
felt hardened movable masses, the size of oranges. Microscopic examination showed the growth to be a diffused intracanalicular fibroma. A peculiar case was presented before the Faculty at Montpellier. [15.5] The patient was a young girl of fifteen and a half years. After a cold bath, just as the menses were appearing, it was found that the breasts were rapidly increasing in size; she was subsequently obliged to leave service on account of their increased size, and finally the deformity was so great as to compel her to keep from the public view. The circumference of the right breast was 94 cm. and of the left 105 cm.; the pedicle of the former measured 67 cm. and of the latter 69 cm.; only the slightest vestige of a nipple remained. Removal was advocated, as applications of iodin had failed; but she would not consent to operation.
Diffuse hypertrophy of the breast is occasionally seen in the male subject. In one case reported from the Westminster Hospital in London, a man of sixty, after a violent fall on the chest, suffered enormous enlargement of the mammæ, and afterward atrophy of the testicle and loss of sexual desire.
The names goiter, struma, and bronchocele are applied indiscriminately to all tumors of the thyroid gland; there are, however, several distinct varieties among them that are true adenoma, which, therefore, deserves a place here. According to Warren, [15.6] Wölfler gives the following classification of thyroid tumors: 1. Hypertrophy of the thyroid gland, which is a comparatively rare disease; 2. Fetal adenoma, which is a formation of gland tissue from the remains of fetal structures in the gland; 3. Gelatinous
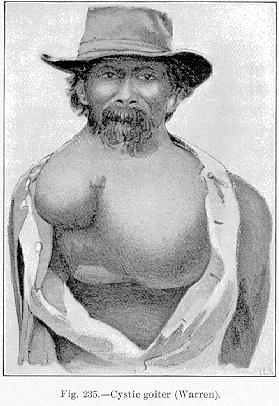
Fig. 235.—Cystic goiter (Warren).
[Description: Drawing of cystic goiter on male]
or interacinous adenoma, which consists in an enlargement of the acini by an accumulation of colloid material, and an increase in the interacinous tissue by a growth of round cells. It is this latter form in which cysts are frequently found. The accompanying illustration (Fig. 235) pictures an extreme ease of cystic goiter shown by Warren. A strange feature of tumors of the thyroid is that pressure-atrophy and flattening of the trachea do not take place in proportion to the size of the tumor. A small tumor of the middle lobe of the gland, not larger that a hen's egg, will do more damage to the trachea than will a large tumor, such as that shown by Senn, [15.7] after Bruns
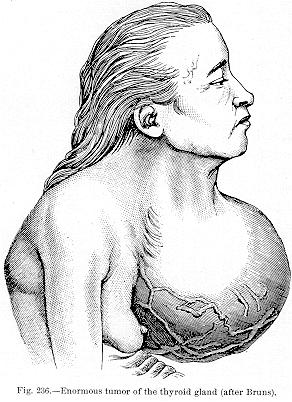
Fig. 236.—Enormous tumor of the thyroid gland (after
Bruns).
[Description: Drawing of tumor]
in the treatment of tumors of the thyroid gland.
Fibromata.—One of the commonest seats of fibroma is the skin. Multiple fibromata of the skin sometimes occur in enormous numbers and cover the whole surface of the body; they are often accompanied by pendulous tumors of enormous size. Virchow called such tumors fibroma molluscum. Figure 237 represents a case of multiple fibromata of the skin shown by Octerlony. Pode [15.8] mentions a somewhat similar case in a man of fifty-six, under the care of Thom. The man was pale and emaciated, with anxious expression, complaining of a tumor which he described as a "wishing-mark.'' On examination he was found to be covered with a number of small tumors, ranging in
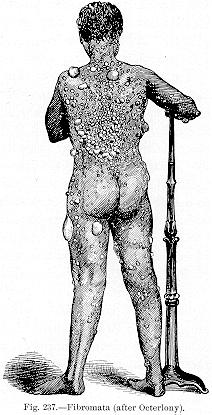
Fig. 237.—Fibromata (after Octerlony).
[Description: Drawing of rear view of man with fibromata]

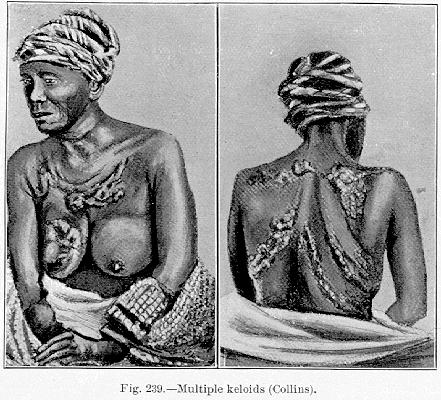
Keloids are fibromata of the true skin, which may develop spontaneously or in a scar. Although the distinction of true and false keloid has been made, it is generally discarded. According to Hebra a true typical keloid is found once in every 2000 cases of skin-disease. It is, however, particularly the false keloid, or keloid arising from cicatrices, with which we have mostly to deal. This tumor may arise from a scar in any portion of the body, and at any age. There seems to be a disposition in certain families and individuals to keloid-formations, and among negroes keloids are quite common, and often of remarkable size and conformation. The form of injury causing the cicatrix is no factor in the production of keloid, the sting of an insect, the prick of a needle, and even the wearing of ear-rings having been frequent causes of keloid-formations among the negro race. Collins [15.9] describes a negress of ninety (Fig. 239), born of African parents, who exhibited multiple keloids produced by diverse injuries. At fourteen she was burned over her breasts by running against a shovelful of hot coals, and several months later small tumors appeared, which never suppurated. When a young girl a tumor was removed from the front of her neck by operation, and cicatricial tumors then spread like a band encircling one-half her neck. There were keloids over her scapulæ, which followed the application of blisters. On her back, over, and following the direction of the ribs, were growths attributed to the wounds caused by a flogging. This case was quite remarkable for the predisposition shown to keloid at an early age, and the variety of factors in causation.
About 1867 Duhring had under his observation at the Philadelphia Hospital a negro whose neck was encircled by enormous keloids, which, although black, otherwise resembled tomatoes. A photograph of this remarkable case (Fig. 240) was published in Philadelphia in 1870. [15.10]
A lipoma is a tumor consisting of adipose tissue. When there is much fibrous tissue in the tumor it is much firmer, and is known as a fibro-lipoma. Brander [15.11] describes a young native of Manchuria, North China, from whom he removed a fibro-lipoma weighing 50 pounds. The growth had progressively enlarged for eleven years, and at the time of extirpation hung as an enormous mass from beneath the left scapula. In operating the tumor had to be swung on a beam (Fig. 241). The hemorrhage was slight and the patient was discharged in five days.
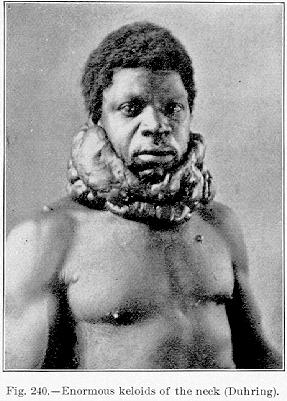
Fig. 240.—Enormous keloids of the neck (Duhring).
[Description: Photograph of man with keloids on neck]
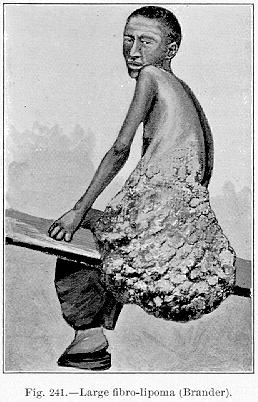
Fig. 241.—Large fibro-lipoma (Brander).
[Description: Drawing of fibro-lipoma]
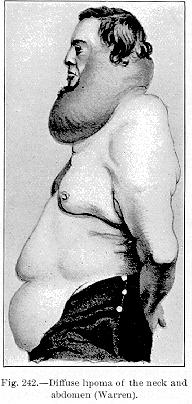
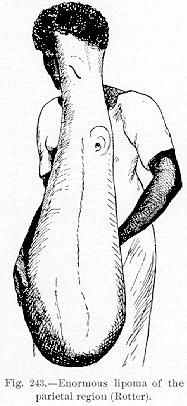
Fig. 243.—Enormous lipoma of the
parietal region (Rotter).
[Description: Drawing of lipoma]
Diffuse lipoma, occurring in the neck, often gives the patient a grotesque and peculiar appearance (Fig. 242). It is generally found in men addicted to the use of alcohol, and
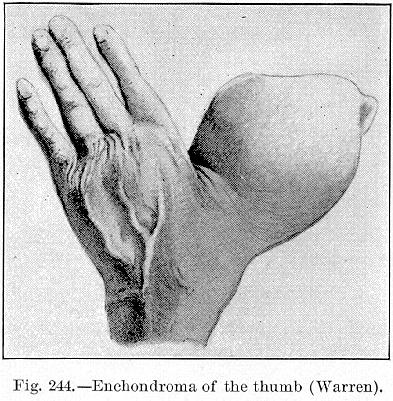
Fig. 244.—Enchondroma of the thumb (Warren).
[Description: Drawing of enchondroma of the thumb]
occurs between thirty-five and forty-five years of age; in no case has general obesity been described. In one of Madelung's cases a large lobe extended downward over the clavicle. The growth has been found between the larynx and the pharynx. Black [15.12] reports a remarkable case of fatty tumor in a child one year and five months old which filled the whole abdominal cavity, weighing nine pounds and two ounces. Chipault [15.13] mentions a case of lipoma of the parietal region, observed by Rotter. This monstrous growth (Fig. 243) was three feet three inches long, descending to the knees. It had its origin in the left parietal region, and was covered by the skin of the whole left side of
the face and forehead. The left ear was plainly visible in the upper third of the growth.
Chondroma, or enchondroma, is a cartilaginous tumor occurring principally
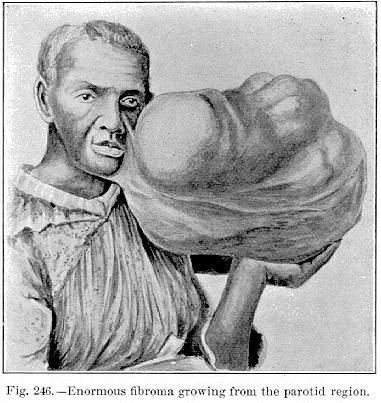
Fig. 246—Enormous fibroma growing from the parotid region.
[Description: Drawing of fibroma]
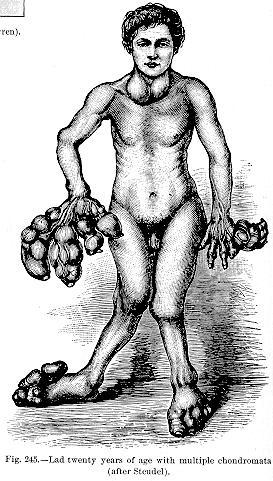
Figure 244 represents an enchondroma of the thumb. Multiple enchondromata (Fig. 245) are most peculiar, and may attain enormous sizes. Whittaker [15.14] describes a farmer of forty who exhibited peculiar tumors of the fingers, which he calls multiple osteoecchondromata. His family history was negative. He stated that at an early age he received a stroke of lightning, which rendered him unconscious for some time. He knows of nothing else that could be in possible relation with his present condition. Nine months after this accident there was noticed an enlargement of the middle joint of the little finger, and about the same time an enlargement on the middle finger. Gradually all the joints of the right hand became involved. The enlargement increased so that at the age of twelve they were
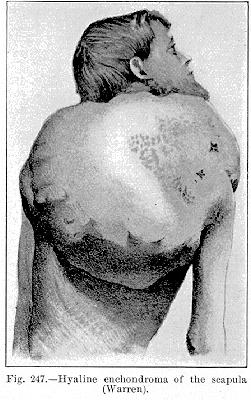
Fig. 247.—Hyaline enchondroma of the scapula
(Warren).
[Description: Drawing of hyaline enchondroma]
of the size of walnuts, and at this time the patient began to notice the same process developing in the left hand.
One of the most frequent of the fibro-cartilaginous tumors is the "mixed cartilaginous'' tumor of Paget, which grows in the interstitial tissues of the parotid gland, and sometimes attains enormous size. Matas [15.15] presented the photograph of a negress having an enormous fibroma growing from the left parotid region (Fig. 246); and there is a photograph of a similar case in the Mütter Museum of the College of Physicians, Philadelphia.
The hyaline enchondroma is of slow growth, but may at times assume immense proportions, as is shown in the accompanying illustration (Fig. 247), given by Warren, of a patient in whom the growth was in the scapula.
In 1824 there is quoted [15.16] the description of a peculiar growth which, though not definitely described, may be spoken of here. It was an enormous encysted tumor, springing from the clavicle of a Veronese nobleman. Contrary to general expectations it was successfully removed by Portalupi, a surgeon of Venice. It weighed 57 pounds, being 20 1/2 inches long and 30 inches in circumference. It is said this tumor followed the reception of a wound.
Among the benign bone tumors are exostoses—homologous outgrowths differing from hypertrophies, as they only involve a limited part of the circumference. When developmental, originating in childhood, the outgrowths may be found on any part of the skeleton, and upon many and
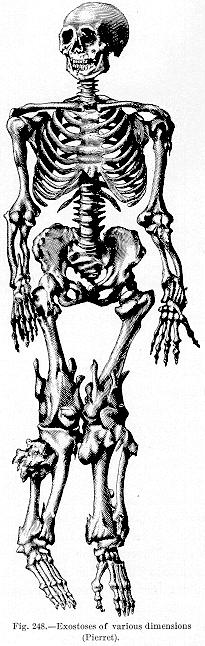
generally symmetric parts at the same time, as is shown in Figure 248.
Barwell [15.17] had a case of a girl with 38 exostoses. Erichsen [15.18] mentions a young man of twenty-one with 15 groups of symmetric exostoses in various portions of the body; they were spongy or cancellous in nature.
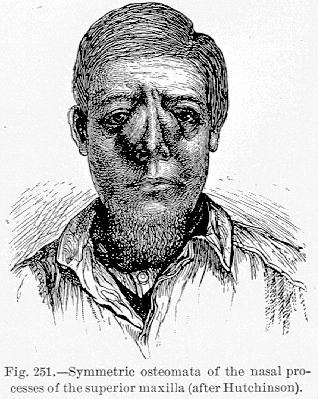
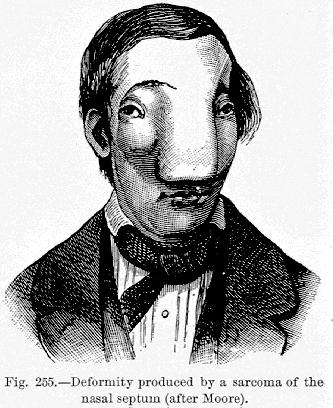
Macland of the French navy [15.20] describes an affection of the bones) of the
face known as anakhrē or goundron (gros-nez). It is so common that about one per cent. of the natives of certain villages on the Ivory Coast, West Africa, are subject to it. As a rule the earliest symptoms in childhood are: more or less persistent headache, particularly frontal, sanguineous and purulent discharge from the nostrils, and the formation of symmetric swellings the size of an almond in the region of the nasal processes of the superior maxilla. The cartilage does not seem to be involved, and, although it is not so stated, the nasal duct appears to remain intact.
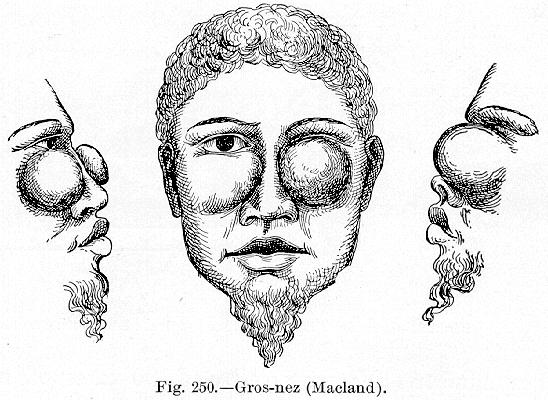
Fig. 250.-Gros-nez (Macland).
[Description: Drawing of gros-nez]
The headache and discharge continue for a year, and the swelling continually increases through life, although the symptoms gradually disappear, the
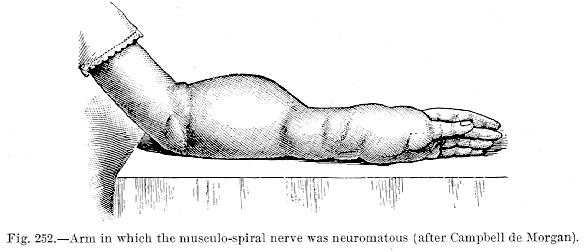
Among neuromata, multiple neurofibroma is of considerable interest, chiefly for the extent of general involvement. According to Senn, Heusinger records the case of a sailor of twenty-three in whom all the nerves were affected by numerous nodular enlargements. Not a nerve in the entire body was found normal. The enlargement was caused by increase in the connective tissue, the axis-cylinders being normal. In this case there was neither pain nor tenderness
Prudden reports the case of a girl of twenty-five who, during convalescence from variola, became paraplegic, and during this time multiple neuromata appeared. At the postmortem more than a thousand tumors were found affecting not only the peripheral branches and the sympathetic, but also the cranial nerves and the pneumogastric. Under the microscope these tumors showed an increase in the interfascicular as well as perivascular fibers, but the nerve-fibers were not increased in size
or number. Virchow collected 30 cases of multiple neurofibromata. In one case he found 500, in another from 800 to 1000 tumors.
Plexiform neuroma is always congenital, and is found most frequently in the temporal region, the neck, and the sides of the face, but almost any part of the body may be affected. Christôt reports two cases in which the
Neuroma of the vulva is a pathologic curiosity. Simpson reports a case
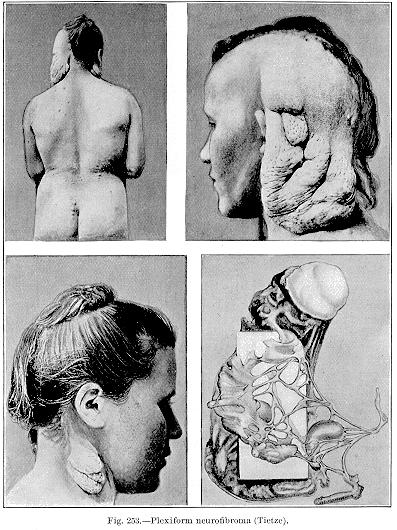
Fig. 253—Plexiform neurofibroma (Tietze).
[Description: Four views of plexiform neurofibroma]
in which the tumor was a painful nodule situated near the urinary meatus. Kennedy mentions an instance in which the tumor appeared as extremely tender tubercles.
Tietze [15.21] describes a woman of twenty-seven who exhibited a marked type of plexiform neurofibroma (Fig. 253). The growth was simply excised and recovery was promptly effected.
Harlan [15.22] reports a most extraordinary epithelioma of
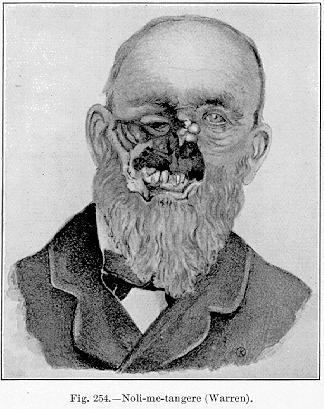
Fig. 254.—Noli-me-tangere (Warren).
[Description: Drawing of man with noli-me-tangere]
the orbit in a boy of about five years (Plate 9). It followed enucleation, and attained the size depicted in a few months.
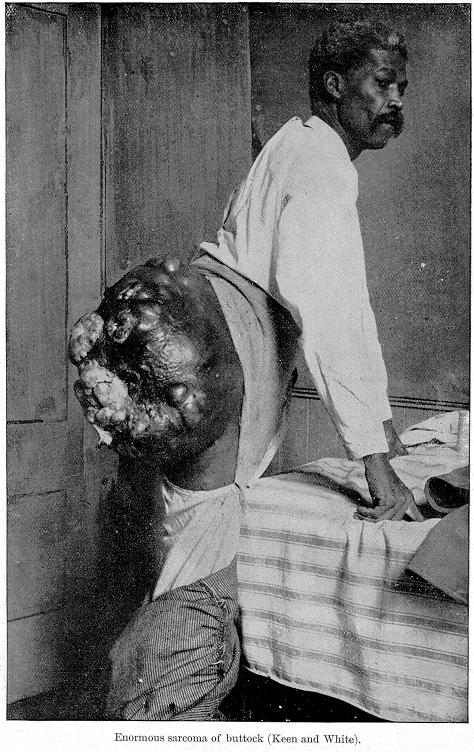
Sarcomata, if allowed full progress, may attain great size. Plate 10 shows an enormous sarcoma of the buttocks in an adult negro. Fascial sarcomata are often seen of immense size. Senn shows a tumor of this variety which was situated between the scapulæ.
Schwimmer records a curious case of universal small sarcomata over the whole body of a teacher of the age of twenty-one, in the Hungarian lowlands. The author called the disease sarcomata pigmentosum diffusum multiplex.
The bones are a common seat of sarcomatous
growths, the tumor in this instance being called osteosarcoma. It may affect any bone, but rarely involves an articulation; at times it skips the joint and goes to the neighboring bone.
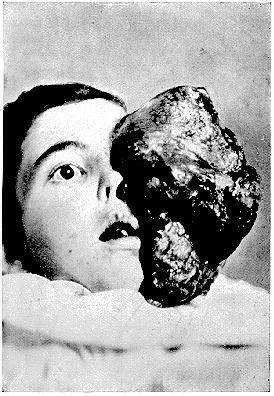
PLATE 9.
[Description: Photograph of epithelioma of the orbit]
Epithelioma of the orbit (Harlan).
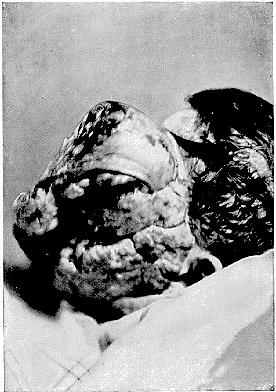
PLATE 9.
[Description: Photograph of epithelioma of the orbit]
Epithelioma of the orbit (Harlan).
Tiffany [15.23] reports several interesting instances of sarcoma, one in a white female of nineteen following a contusion of tibia. The growth had all the clinical history of an osteosarcoma of the tibia, and was amputated and photographed after removal (Fig. 256). In another case, in a white male of
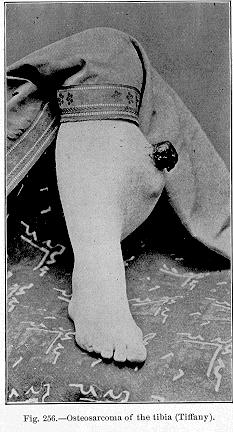
Fig. 256.—Osteosarcoma of the tibia (Tiffany).
[Description: Photograph of leg with osteosarcoma]

Fig. 257.—Sarcoma of the thigh (Tiffany).
[Description: Photograph of sarcoma of the thigh]
thirty, the same author successfully performed a hip-amputation for a large sarcoma of the left femur. The removed member was sent entire to the Army Medical Museum at Washington (Fig. 257).
The fatality and incurability of malignant growths has done much to stimulate daring and marvelous operations in surgery. The utter hopelessness of the case justifies almost any means of relief, and many of the visceral operations, resections of functional organs, and extraordinary amputations that were never dreamed of in the early history of medicine are to-day not only feasible and justifiable, but even peremptorily demanded.
Abbe [15.25] shows a peculiar aneurysmal varix of the finger in a boy of nine (Fig. 258). When a babe the patient had, on the dorsum of the little finger, a small nevus, which was quiescent for many years. He received a deep cut at the base of the thumb, and immediately after this accident the nevus began to enlarge

Fig. 258.—Aneurysmal varix of hand (Abbe).
[Description: Drawing of aneurysmal varix of hand]
rapidly. But for the local aneurysmal thrill at the point of the scar the condition would have been diagnosed as angioma, but as a bruit could be heard over the entire mass it was called an aneurysmal varix, because it was believed there was a connection between a
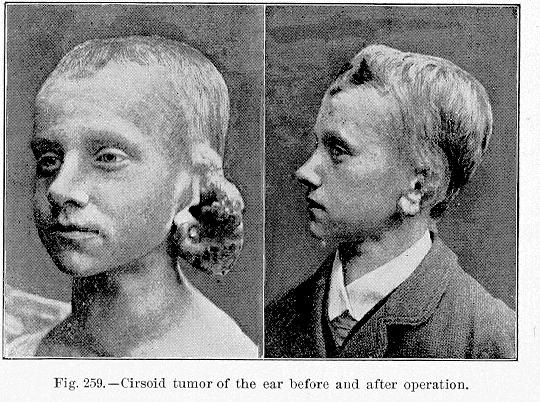
rather large artery and a vein close to the mass. There is a curious case reported [15.26] of cirsoid tumor of the ear of a boy of thirteen. Figure 259 shows the appearance before and after operation.
Relative to the size of an aneurysm, Warren [15.29] reported a case of the abdominal aorta which commenced at the origin of the
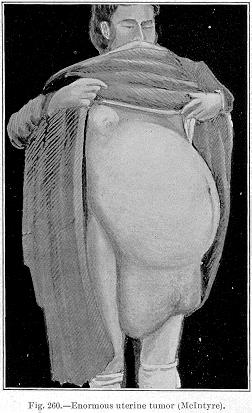
Fig. 260.—Enormous uterine tumor (McIntyre).
[Description: Drawing of uterine tumor]
celiac axis and passed on to the surfaces of the psoas and iliac muscles, descending to the middle of the thigh The total length of the aneurysm was 19 inches, and it measured 18 inches in circumference.
A peculiar sequence of an aortic aneurysm is perforation of the sternum or rib. Webb [15.30] mentions an Irish woman who died of aneurysm of the aorta, which had perforated the sternum, the orifice being plugged by a large clot. He quotes 17 similar cases which he has collected as occurring from
Large Uterine Tumors.—Before the meeting of the American Medical Association held in Washington, D. C., 1891, McIntyre [15.31] reported a case of great interest. The patient, a woman of thirty-eight, five feet 5 1/2 inches in height, coarse, with masculine features, having hair on her upper lip and chin, and weighing 199 1/2 pounds, was found in a poor-house in Trenton, Missouri, on November 26, 1890, suffering from a colossal growth of the abdomen. The accompanying illustration is from a photograph which was taken at the time of the first interview (Fig. 260). The measurements made at the time were as follows: circumference at the largest part, just below the umbilicus, 50 inches; circumference just below the mammæ, 35 inches; from the xiphoid cartilage to the symphysis pubis, 32 inches, not including the appendum, which is shown in the picture. Percussion suggested a fluid within a sac. The uterus was drawn up to the extent of from 12 to 14 inches. The woman walked with great difficulty and with a waddling gait, bending far backward the better to keep "the center of gravity within the base,'' and to enable her to sustain the
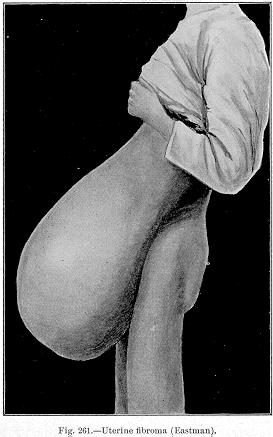
Fig. 261.—Uterine fibroma (Eastman).
[Description: Drawing of uterine fibroma]
enormous weight of the abdomen. She was compelled to pass her urine while standing. Attempts had been made six and two years before to tap this woman, but only a few drops of blood followed several thrusts of a large trocar. A diagnosis was made of multilocular ovarian cyst or edematous myoma of the uterus, and on the morning of December 7, 1890, an operation was performed. An incision 14 inches in length was first made in the linea alba, below the umbilicus, and afterward extended up to the xiphoid cartilage. The hemorrhage from the abdominal wall was very free, and the enormously distended vessels required the application of a
It is quite possible for a fibrocyst of the uterus to attain an enormous size, equaling the ovarian cysts. Stockard [15.34] describes an instance of this nature in a negress of fifty, the mother of several children. About twelve years before a cyst in the right iliac region was tapped. The
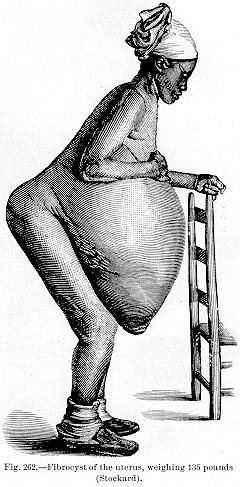
woman presented the following appearance (Fig. 262): The navel hung below her knees, and the skin near the umbilicus resembled that of an elephant. The abdomen in its largest circumference measured 68 inches, and 27 inches from the ensiform cartilage to the umbilicus. The umbilicus was five inches in diameter and three inches in length. Eight gallons and seven pints of fluid were removed by tapping, much remaining. The whole tumor weighed 135 pounds. Death from exhaustion followed on the sixth day after the tapping.
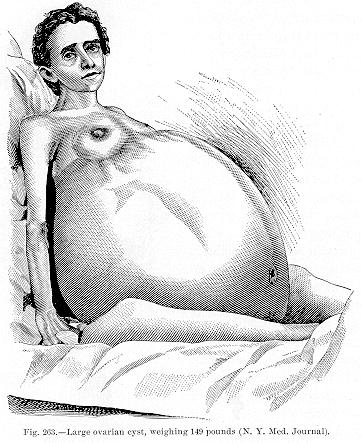
150 pounds. Morand *[575] speaks of an ovarian cyst from which, in ten months, 427 pounds of fluid were withdrawn. There are old records of tubal cysts weighing over 100 pounds. Normand [15.38] speaks of an ovary degenerating into a scirrhous mass weighing 55 pounds. Among recent operations Briddon [15.39] describes the removal of an ovarian cyst which weighed 152 pounds, death resulting. Helmuth [15.40] mentions an ovarian cyst from which, in 12 tappings,
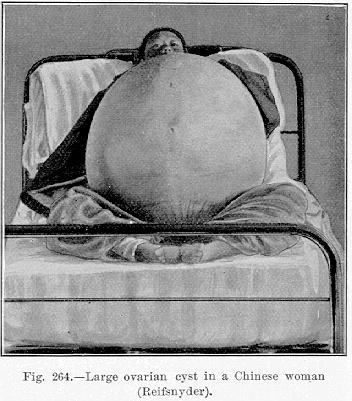
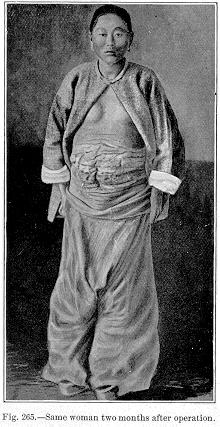
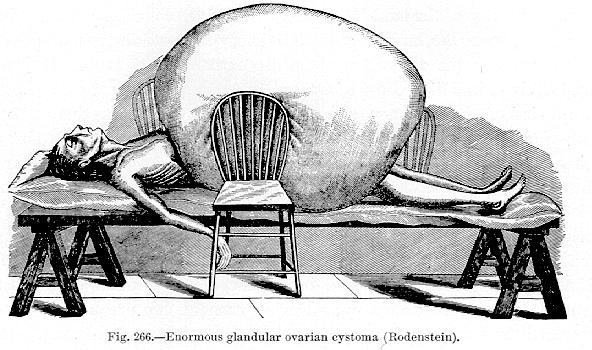
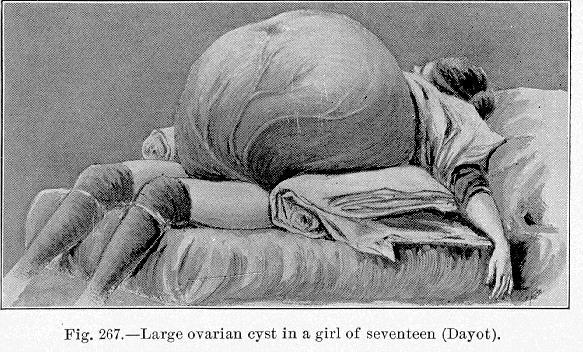
the woman two months after the operation, when the girth was reduced to normal. Stone [15.43] performed ovariotomy on a girl of fifteen, removing a tumor weighing 81 1/2 pounds. Ranney [15.44] speaks of the successful removal of a unilocular tumor weighing 95 pounds; and Wall [15.45] tells of a death after removal of an ovarian tumor of the same weight. Rodenstein [15.46] portrays (Fig. 266) the appearance of a patient of forty-five after death from an enormous glandular ovarian cystoma. The tumor was three feet high, covered the breasts, extended to the knees, and weighed 146 pounds. Kelly speaks of a cyst weighing 116 pounds; Keith [15.47] one of 89 1/2 pounds; Gregory, [15.48] 80 pounds; Boerstler, [15.49] 65 pounds; Bixby, [15.50] 70 pounds; and Alston [15.51] a tumor of 70 pounds removed in the second operation of ovariotomy.
Cullingworth [15.53] of St. Thomas Hospital, London, successfully removed from a girl of sixteen an ovarian cyst weighing over 80 pounds. The patient was admitted to the hospital April 30, 1895. She gave a history of a single menstruation, which took place in March or April, 1893, and said that in the latter month she noticed that she was growing large. She was tapped at Christmas, 1893, when a large quantity of fluid was removed, and again in February, 1894, and a third time in May, 1894, but without useful results. For the previous six months she had been almost entirely bedridden because of the great size of the tumor. There were no symptoms referring to the bladder and rectum. At the time she entered the hospital she was much emaciated, the eyes were sunken, and her cheeks had a livid hue. The chest was thin and the lower ribs
were everted; dulness began at the lower border of the 3d cartilage, and the apex-beat was best felt in the third space. Liver-dulness began at the 4th rib cartilage in the nipple line. The abdomen was enormously distended, and covered by large veins running from below upward to the thorax. About 3 1/2 inches above the umbilicus there was a sulcus with its convexity downward. There was dulness over the whole abdomen, except at the sides parallel with the lumbar spines, and a resonant band over the stomach. The greatest girth was 54 1/2 inches. By vaginal examination the cervix was found to be pulled up and obliterated; the anterior vaginal wall was bulged downward by the tumor. On May 3d
septa between the cysts were broken down with the fingers. The pedicle was rather small and was tied in the usual way, and the tumor was removed. Its seat of origin was the left ovary. The right ovary and the uterus were healthy, but poorly developed. The tumor weighed between 80 and 90 pounds,—the
patient having weighed 170 pounds on the night before the operation and 79 1/2 pounds a week after the operation. Alarming symptoms of collapse were present during the night after the operation, but the patient responded to stimulation by hypodermic injections of 1/20 grain of strychnin and of brandy, and after the first twenty-four hours the recovery was uninterrupted.
In the records of enormous dropsies much material of interest is to be found, and a few of the most interesting cases on record will be cited. In the older times, when the knowledge of the etiology and pathology of dropsies was obscure, we find the records of the most extraordinary cases. Before the Royal Society, in 1746, Glass of Oxford [15.54] read the report of a case of preternatural size of the abdomen, and stated that the dropsy was due to the absence of one kidney. The circumference of the abdomen was six feet four inches, and the distance from the xiphoid to the os pubis measured four feet 1/2 inch. In this remarkable case 30 gallons of fluid were drawn off from the abdomen after death. Bartholinus [15.55] mentions a dropsy of 120 pounds; and Gockelius one of 180 pounds; there is recorded [15.56] an instance of a dropsy of 149 pounds. There is an old record [15.57] of a woman of fifty who had suffered from ascites for thirty years. She had been punctured 154 times, and each time about 20 pints were drawn off. During each of two pregnancies she was punctured three or four times; one of her children was still living. It has been said *[462] that there was a case in Paris of a person who was punctured 300 times for ascites. Scott [15.58] reports a case of ascites in which 928 pints of water were drawn off in 24 successive tappings, from February, 1777, to May, 1778. Quoted by Hufeland, Van Wy mentions 1256 pounds of fluid being drawn from the abdomen of a woman in five years. Kaltschmid [15.59] describes a case of ascites in which, in 12 paracenteses, 500 pounds of fluid were removed. In 1721 Morand reported two cases of ascites in one of which, by the means of 57 paracenteses, 970 pounds of fluid were drawn off in twenty-two months. In the other case 1708 pounds of fluid issued in ten months. There is a record of 484 pounds of "pus'' being discharged during a dropsy. [15.60]
The Philosophical Transactions contain the account of a case of hydronephrosis in which there were 240 pounds of water in the sac. There are several cases on record in which ovarian dropsies have weighed over 100 pounds; and Blanchard mentions a uterine dropsy of 80 pounds.
The Ephemerides contains an account of a case of hydrocephalus in which there were 24 pounds of fluid, and similar cases have been noted.
Elliotson [15.61] reports what he calls the largest quantity of pus from the liver on record. His patient was a man of thirty-eight, a victim of hydatid disease of the liver, from whom he withdrew one gallon of offensive material.
Ankylosis of the articulations, a rare and curious anomaly, has been seen in the human fetus by Richaud, Joulin, Bird, and Becourt. Ankylosis of all the joints, with muscular atrophy, gives rise to a condition that has been popularly termed "ossified man.'' A case of this nature is described, [15.62] the patient being a raftsman, aged seventeen, who suffered with inflammatory symptoms of the right great toe, which were followed in the next ten years by progressive involvement of all the joints of the extremities, and of the vertebræ and temporo-maxillary articulations, with accompanying signs of acute articular rheumatism. At the age of thirty-one the pains had subsided, leaving him completely disabled. All the joints except the fingers and toes had become ankylosed, and from nonusage the muscles had atrophied (Fig. 268). There were no dislocations, anesthesia, or bedsores, and the
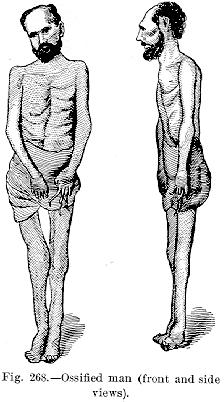
viscera were normal; there were apparently no gouty deposits, as an examination of the urine was negative
J. R. Bass, the well-known "ossified man'' of the dime museums, has been examined by many physicians, and was quite intelligent and cheerful in spite of his complete ankylosis. Figure 269 represents his appearance in 1887
Percy [15.63] speaks of a man named Simoore, born in 1752, who at the age of
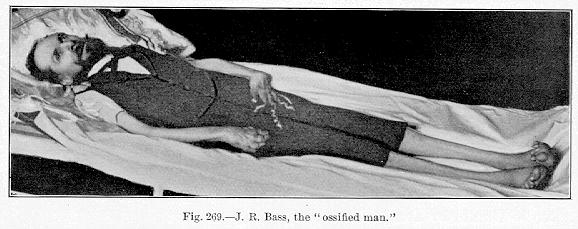
Fig. 269.—J. R. Bass, the "ossified man.''
[Description: Photograph of J. R. Bass]
fifteen was afflicted with ankylosis of all the joints, and at different angles He was unable to move even his jaw, and his teeth had to be extracted in order to supply him with nourishment. Even his ribs were ankylosed; his chest
An ossified man has been recently found and exhibited to the Paris Academy of Medicine. He is a Roumanian Jew of thirty who began to ossify twelve years ago, first up the right side of his back, then down the left side. He has hardened now to the nape of the neck, his head is turned to the left, and the jaws are ankylosed. He can still move his arms and legs a little with great difficulty.
Akin to the foregoing condition is what is known as petrifaction or ossification of portions of the living human body other than the articulations. Of the older writers Hellwigius, *[414] Horstius, *[423] and Schurig [15.64] speak of petrifaction of the arm. In the Philosophical Transactions there was a case recorded in which the muscles and ligaments were so extensively converted into bone that all the joints were fixed, even including the vertebræ, head, and lower jaw. In a short time this man was, as it were, one single bone from his head to his knees, the only joints movable being the right wrist and knee. For over a century there has been in the Trinity College at Dublin the skeleton of a man who died about 20 miles from the city of Cork. The muscles about the scapula, and the dorsum of the ilium (the glutei) were converted into great masses of bone, equal to the original muscles in thickness and bulk. Half of the muscles of the hips and thighs were converted into bone, and for a long time this specimen was the leading curiosity of the Dublin Museum. [15.65] In the Isle of Man, some years ago, there was a case of ossification which continued progressively for many years. Before death this man was reduced to almost a solid mass of bony substance. With the exception of one or two toes his entire frame was solidified. He was buried in Kirk Andreas Churchyard, and his grave was strictly guarded against medical men by his friends, but the body was finally secured and taken to Dublin by Dr. McCartney. [15.66]
Calculi.—In reviewing the statistics of vesical calculi, the strangest anomalies in their size and weight have been noticed. Among the older writers the largest weights have been found. Le Cat speaks of a calculus weighing over three pounds, and Morand is accredited with having seen a
Multiple Vesical Calculi.—Usually the bladder contains a single calculus, but in a few instances a large number of stones have been found to coexist. According to Ashhurst, the most remarkable case on record is that of the aged Chief Justice Marshal, from whose bladder Dr. Physick of Philadelphia is said to have successfully removed by lateral lithotomy more than 1000 calculi. Macgregor mentions a case in which 520 small calculi coexisted with a large one weighing 51 ounces. *[174] There is an old record of 32 stones having been removed from a man of eighty-one, a native of Dantzic, 16 of which were as large as a pigeon's egg. Kelly [15.81] speaks of 228 calculi in the bladder of a man of seventy-three, 12 being removed before death. The largest weighed 111 grains. Goodrich [15.82] took 96 small stones from the bladder of a lad. Among the older records of numerous calculi Burnett mentions 70; Desault, over 200; the Ephemerides, 120; Weickman, over 100; Fabricius Hildanus, 2000 in two years; and there is a remarkable case of 10,000 in all issuing from a young girl. [15.83] Greenhow [15.84] mentions 60 stones removed from the bladder. An older issue of The Lancet contains an account of lithotrity performed on the same patient 48 times.
Occasionally the calculi are discharged spontaneously. Trioen *[784] mentions the issue of a calculus through a perineal aperture, and there are many similar cases on record. There is an old record of a stone weighing five ounces being passed by the penis. [15.85] Schenck mentions a calculus perforating the bladder and lodging in the groin. Simmons [15.86] reports a case in which a calculus passed through a fistulous sore in the loins without any concomitant passage of urine through the same passage. Vosberg [15.87] mentions a calculus in a patent urachus; and calculi have occasionally been known to pass from the umbilicus. Gourges [15.88] mentions the spontaneous excretion of a five-ounce calculus; and Thompson [15.89] speaks of the discharge of two calculi of enormous size.
Of the extravresical calculi some are true calculi, while others are simply the result of calcareous or osseous degeneration. Renal and biliary calculi are too common to need mention here. There are some extraordinary calculi taken from a patient at St. Bartholomew's Hospital and deposited in the museum of that institution. The patient was a man of thirty-eight. In the
At the University College Hospital, London, there are exhibited 485 gall-stones that were found postmortem in a gall-bladder. Vanzetti reports [15.91] the removal of a preputial calculus weighing 224 grams. Phillipe [15.92] mentions the removal of a calculus weighing 50 grams from the prepuce of an Arab boy of seven. Croft [15.93] gives an
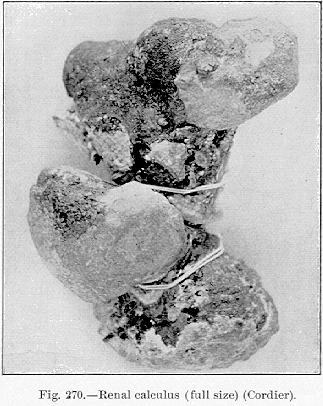
Fig 270.—Renal calculus (full size) (Cordier).
[Description: Photograph of renal calculus]
account of some preputial calculi removed from two natives of the Solomon Islands by an emigrant medical officer in Fiji. In one case 22 small stones were removed, and in the other a single calculus weighing one ounce 110 grains. Congenital phimosis is said to be very common among the natives of Solomon Islands.
In September, 1695, Bernard [15.94] removed two stones from the meatus urinarius of a man, after a lodgment of twenty years. Block [15.95] mentions a similar case, in which the lodgment had lasted twenty-eight years. Walton [15.96] speaks of a urethral calculus gradually increasing in size for fifty years. Ashburn [15.97] shows (Fig. 271) what he considers the largest calculus ever removed from the urethra. It was 2 1/8 inches long, and 1 1/4
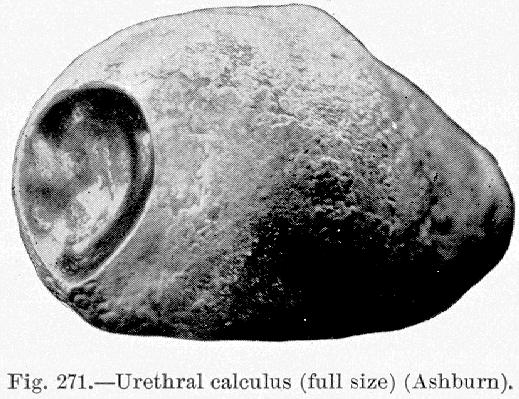
Fig.271.—Urethral calculus (full size) (Ashburn).
[Description: Drawing of urethral calculus]
inches in diameter; it was white on the outside, very hard, and was shaped and looked much like a potato. Its dry weight was 660 grains. At one end was a polished surface that corresponded with a similar surface on a smaller stone that lay against it; the latter calculus was shaped like a lima bean, and
Calcareous degeneration is seen in the ovary, and Peterman [15.99] speaks of a stone in the ovary. Uterine calculi are described by Cuevas [15.100] and Harlow; [15.101] the latter mentions that the calculus he saw was egg-shaped. There is an old chronicle of a stone taken from the womb of a woman near Trent, Somersetshire, at Easter, 1666, that weighed four ounces. The Ephemerides speaks of a calculus coming away with the menstrual fluid.
Stones in the heart are mentioned by medical writers, and it is said [15.102] that two stones as large as almonds were found in the heart of the Earl of Balcarres.
Morand [15.103] speaks of a calculus ejected from the mouth by a woman.
An old record says [15.104] that stones in the brain sometimes are the cause of convulsions. D'Héricourt reports the case of a girl who died after six months' suffering, whose pineal gland was found petrified, and the incredible size of a chicken's egg. Blasius, Diemerbroeck, and the Ephemerides, speak of stones in the location of the pineal gland.
Salivary calculi are well known; they may lodge in any of the buccal ducts. There is a record of the case [15.105] of a man of thirty-seven who suffered great pain and profuse salivation. It was found that he had a stone as large as a pigeon's egg under his tongue.
Umbilical calculi are sometimes seen, and Dean [15.106] reports such a case. There is a French record [15.107] of a case of exstrophy of the umbilicus, attended with abnormal concretions.
Aetius, Marcellus Donatus, Scaliger, and Schenck mention calculi of the eyelids.
There are some extraordinary cases of retention and suppression of urine on record. Actual retention of urine, that is, urinary secretion passed into the bladder, but retention in the latter viscus by inanition, stricture, or other obstruction, naturally cannot continue any great length of time without mechanically rupturing the vesical walls; but suppression of urine or absolute anuria may last an astonishingly extended period. Of the cases of retention of urine, Féréol [15.108] mentions that of a man of forty-nine who suffered absolute retention of urine for eight days, caused by the obstruction of a uric acid calculus. Cunyghame [15.109] reports a case of mechanic obstruction of the flow of urine for eleven days. Trapenard speaks of retention of urine for seven days. Among the older writers Bartholinus *[189] mentions ischuria lasting fourteen days; Cornarius, fourteen days; Rhoclius, fifteen days; the Ephemerides, ten, eleven, and twelve days. Croom [15.110] notes a case of retention of
The accumulation of urine in cases of ischuria is sometimes quite excessive. De Vilde [15.112] speaks of 16 pints teeing drawn off. Mazoni cites a case in which 15 pounds of urine were retained; and Wilson [15.113] mentions 16 pounds of urine being drawn off. Frank [15.114] reports instances in which both 12 and 30 pounds of urine were evacuated. There is a record at the beginning of this century [15.115] in which it is stated that 31 pounds of urine were evacuated in a case of ischuria.
Following some toxic or thermic disturbance, or in diseased kidneys, suppression of urine is quite frequently noticed. The older writers report some remarkable instances: Haller *[397] mentions a case lasting twenty-two weeks; Domonceau, [15.116] six months; and Marcellus Donatus, *[306] six months.
Whitelaw [15.117] describes a boy of eight who, after an attack of scarlet fever, did not pass a single drop of urine from December 7th to December 20th when two ounces issued, after vesication over the kidneys. On January 2d two ounces more were evacuated, and no more was passed until the bowel acted regularly. On January 5th a whole pint of urine passed; after that the kidneys acted normally and the boy recovered. It would be no exaggeration to state that this case lasted from December 5th to January 5th, for the evacuations during this period were so slight as to be hardly worthy of mention.
Lemery [15.118] reports observation of a monk who during eight years vomited periodically instead of urinating in a natural way. Five hours before vomiting he experienced a strong pain in the kidneys. The vomitus was of dark-red color, and had the odor of urine. He ate little, but drank wine copiously, and stated that the vomiting was salutary to him, as he suffered more when he missed it.
Bryce [15.119] records a case of anuria of seventeen days' standing. Butler [15.120] speaks of an individual with a single kidney who suffered suppression of urine for thirteen days, caused by occlusion of the ureter by an inspissated thrombus. Dubuc [15.121] observed a case of anuria which continued for seventeen days before the fatal issue. Fontaine [15.122] reports a case of suppression of urine for twenty-five days. Nunneley [15.123] showed the kidneys of a woman who did not secrete any urine for a period of twelve days, and during this time she had not exhibited any of the usual symptoms of uremia. Peebles [15.124] mentions a case of suspension of the functions of the kidneys more than once for five weeks, the patient exhibiting neither coma, stupor, nor vomiting. Oke [15.125]
The most persistent constipation may exist for weeks, or even months, with fair health. The fact seemed to be a subject of much interest to the older writers. De Cabalis [15.127] mentions constipation lasting thirty-seven days; Caldani, sixty-five days; Lecheverel, [15.128] thirty-four days; and Pomma [15.129] eight months; Sylvaticus, thirty months; Baillie, [15.130] fifteen weeks; Blanchard, *[213] six weeks; Smetius, *[730] five mouths; Trioen, *[784] three months; Devilliers, [15.131] two years; and Gignony, [15.132] seven years. Riveriusf *[687] mentions death following constipation of one month, and says that the intestines were completely filled. Moosman [15.133] mentions death from the same cause in sixty days. Frank speaks of constipation from intestinal obstructions lasting for three weeks, and Manget mentions a similar case lasting three months.
Early in the century Révolat reported in Marseilles an observation of an eminently nervous subject addicted to frequent abuse as regards diet, who had not had the slightest evacuation from the bowel for six months. A cure was effected in this case by tonics, temperance, regulation of the diet, etc. In Tome xv. of the Commentaries of Leipzig there is an account of a man who always had his stercoral evacuations on Wednesdays, and who suffered no evil consequences from this abnormality. This state of affairs had existed from childhood, and, as the evacuations were abundant and connected, no morbific change or malformation seemed present. The other excretions were slightly in excess of the ordinary amount. There are many cases of constipation on record lasting longer than this, but none with the same periodicity and without change in the excrement. Tommassini [15.134] records the history of a man of thirty, living an ordinary life, who became each year more constipated. Between the ages of twenty and twenty-four the evacuations were gradually reduced to one in eight or ten days, and at the age of twenty-six, to one every twenty-two days. His leanness increased in proportion to his constipation, and at thirty his appetite was so good that he ate as much as two men. His thirst was intense, but he secreted urine natural in quantity and quality. Nothing seemed to benefit him, and purgatives only augmented his trouble. His feces came in small, hard balls. His tongue was always in good condition, the abdomen not enlarged, the pulse and temperature normal.
Emily Plumley was born on June 11,1850, with an imperforate anus, and lived one hundred and two days without an evacuation. During the whole
Fleck [15.137] reports the case of a Dutchman who, during the last two years, by some peculiar innervation of the intestine, had only five or six bowel movements a year. In the intervals the patient passed small quantities of hard feces once in eight or ten days, but the amount was so small that they constituted no more than the feces of one meal. Two or three days before the principal evacuation began the patient became ill and felt uncomfortable in the back; after sharp attacks of colic he would pass hard and large quantities of offensive feces. He would then feel better for two or three hours, when there would be a repetition of the symptoms, and so on until he had four or five motions that day. The following day he would have a slight diarrhea and then the bowels would return to the former condition. The principal fecal accumulations were in the ascending and transverse colon and not only could be felt but seen through the abdominal wall. The patient was well nourished and had tried every remedy without success. Finally he went to Marienbad where he drank freely of the waters and took the baths until the bowel movements occurred once in two or three days.
There is a record [15.138] of a man who stated that for two years he had not passed his stool by the anus, but that at six o'clock each evening he voided feces by the mouth. His statement was corroborated by observation. At times the evacuation took place without effort, but was occasionally attended with slight pain in the esophagus and slight convulsions. Several hours before the evacuation the abdomen was hard and distended, which appearance vanished in the evening. In this case there was a history of an injury in the upper iliac region.
The first accurate ideas in reference to elephantiasis arabum are given by Rhazes, Haly-Abas, and Avicenna, and it is possibly on this account that the disease received the name elephantiasis arabum. The disease was afterward noticed by Forestus, Mercurialis, Kaempfer, Ludoff, and others. In 1719 Prosper Alpinus wrote of it in Egypt, and the medical officers of the French army that invaded Egypt became familiar with it; since then the disease has been well known.
Alard relates as a case of elephantiasis that of a lady of Berlin, mentioned in the Ephemerides of 1694, who had an abdominal tumor the lower part of which reached to the knees. In this case the tumor was situated in the skin and no vestige of disease was found in the abdominal cavity and no sensible alteration had taken place in the veins. Delpech quotes a similar case of elephantiasis
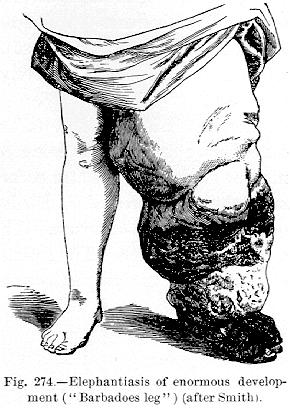
Lymphedema, or elephantiasis arabum, is a condition in which, in the substance of a limb or a part, there is diffused dilatation of the lymphatics, with lymphostasis. Such a condition results when there is obstruction of so large a number of the ducts converging to the root of the extremity or part that but little relief through collateral trunks is possible. The affected part becomes swollen and hardened, and sometimes attains an enormous size. It is neither reducible by position nor pressure. There is a corresponding dilatation and multiplication of the blood-vessels with the connective-tissue hypertrophy. The muscles waste, the skin becomes coarse and hypertrophied. The swollen
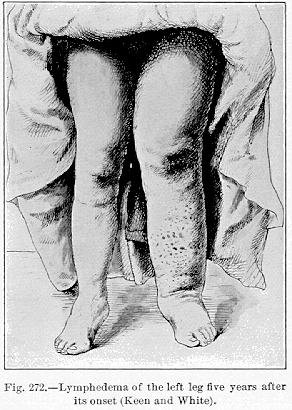
limb presents immense lobulated masses, heaped up at different parts, separated from one another by deep sulci, which are especially marked at the flexures of the joints. Although elephantiasis is met with in all climates, it is more common in the tropics, and its occurrence has been repeatedly demonstrated in these localities to be dependent on the presence in the lymphatics of the filaria sanguinis hominis. The accompanying illustration (Fig. 272) *[845] shows the condition of the limb of a girl of twenty-one, the subject of lymphedema, five years after the inception of the disease. The changes in the limb were as yet
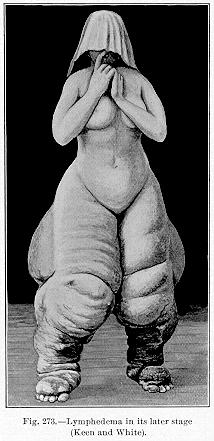
in its most aggravated form, a condition rarely observed in this country. As an example of the change in the weight of a person after the inception of this disease, we cite a case reported by Griffiths. [15.139] The patient was a woman of fifty-two who, five years previous, weighed 148 pounds. The elephantoid change was below the waist, yet at the time of report the woman weighed 387 pounds. There was little thickening of the skin. The circumference of the calf was 28 inches; of the thigh, 38 inches; and of the abdomen, 80 inches; while that of the arm was only 15 inches.
The condition commonly
known as "Barbadoes leg'' (Fig. 274) is a form of elephantiasis deriving its name from its relative frequency in Barbadoes.
Elephantiasis seldom attacks the upper extremities. Of the older cases Rayer reports four collected by Alard. In one case the hard and permanent swelling of the arm occurred after the application of a blister; in another the arm increased so that it weighed more than 200 Genoese pounds, 40 of which consisted of serum. The swellings of the arm and forearm resembled a distended bladder. The arteries, veins, and nerves had not undergone any alteration, but the lymphatics were very much dilated and loaded with lymph.
The third case was from Fabricius Hildanus, and the fourth from Hendy. Figure 276 represents a remarkable elephantoid change in the hand of an elderly German woman. Unfortunately there is no medical description of the case on record, but the photograph is deemed worthy of reproduction.
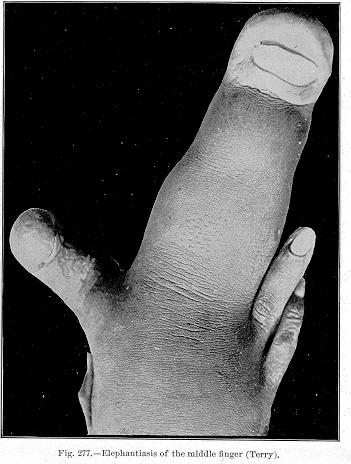
Terry [15.140] describes a French mulatto girl of eleven whose left hand was enormously increased in weight and consistency, the chief enlargement being in the
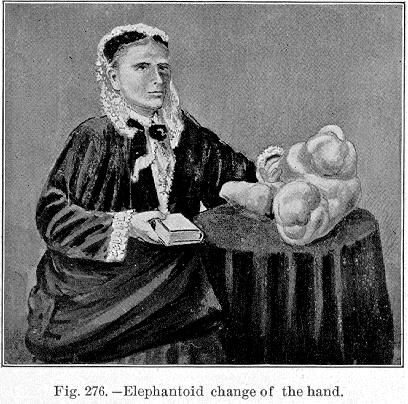
Fig. 276.—Elephantoid change of the hand.
[Description: Drawing of eleophantoid change in the hand]
middle finger, which was 6 1/2 inches long, and 5 1/2 inches about the nail, and 8 1/2 around the base of the finger. The index finger was two inches thick and four inches long, twisted and drawn, while the other fingers were dwarfed. The elephantiasis in this case slowly and gradually increased in size until the hand weighed 3 1/2 pounds. The skin of the affected finger, contrary to the general appearance of a part affected with elephantiasis, was of normal color, smooth, shiny, showed no sensibility, and the muscles had undergone fatty degeneration. It was successfully amputated in August, 1894. The accompanying illustration (Fig. 277) shows a dorsal view of the affected hand.
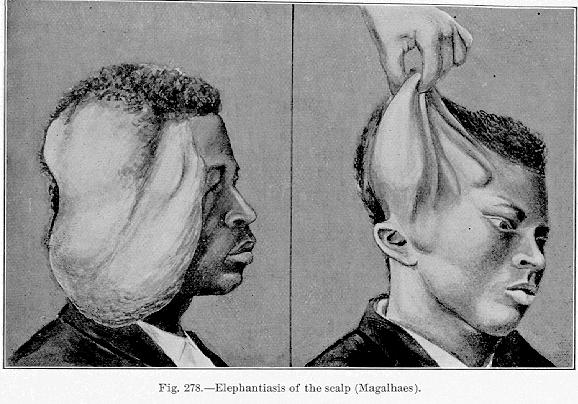
Magalhaes of Rio Janeiro [15.141] reports a very interesting case of elephantiasis of the scalp, representing dermatolysis, in which the fold of hypertrophied skin fell over the face like the hide of an elephant (Fig. 278), somewhat similar in appearance to the "elephant-man.'' Figure 279 represents a somewhat
Elephantiasis of the face sometimes only attacks it on one side. Such a case was reported by Alard, in which the elephantiasis seems to have been complicated with eczema of the ear. Willier, also quoted by Alard, describes a remarkable case of elephantiasis of the face. After a debauch this patient experienced violent pain in the left cheek below the zygomatic arch; this soon extended under the chin, and the submaxillary glands enlarged and became painful; the face swelled and became erythematous, and the patient experienced nausea and slight
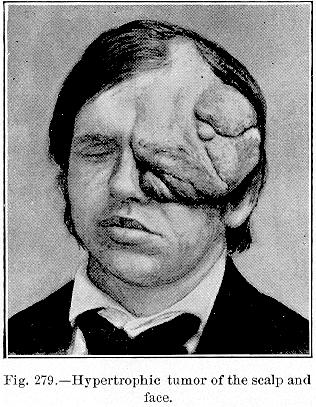
Fig. 279.—Hypertrophic tumor of the scalp and
face.
[Description: Drawing of hypertrophic tumor]
chills. At the end of six months there was another attack, after which the patient perceived that the face continued puffed. This attack was followed by several others, the face growing larger and larger. In similar cases tumefaction assumes enormous proportions, and Schenck [15.142] speaks of a man whose head exceeded that of an ox in size, the lower part of the face being entirely covered with the nose, which had to be raised to enable its unhappy owner to breathe.
Rayer cites two instances in which elephantiasis of the breast enlarged these organs to such a degree that they hung to the knees. Salmuth [15.143] speaks of a woman whose breasts increased to such a size that they hung down to her knees. At the same time she had in both axillæ glandular tumors as large as the head of a fetus. Borellus *[841] also quotes the case of a woman whose breasts became so large that it was necessary to support them by straps, which passed over the shoulders and neck.
Elephantiasis is occasionally seen in the genital regions of the female (Fig. 280), but more often in the scrotum of the male, in which location it

Fig. 280.—Elephantiasis of the labia
(Scanzoi).
[Description: Drawing of elephantiasis of the labia]
produces enormous tumors, which sometimes reach to the ground and become so heavy as to prevent locomotion. This condition is curious in the fact that
There are several old accounts of scrotal tumors which have evidently been elephantoid in conformation. In the Ephemerides in 1692 there was mentioned a tumor of the scrotum weighing 200 pounds. In the West Indies it was reported that rats have been known to feed on these enormous tumors, while the deserted subjects lay in a most helpless condition. Larrey mentioned a case of elephantiasis of the scrotum in which the tumor weighed over 200 pounds. Sir Astley Cooper removed a tumor of 56 pounds weight from a Chinese laborer. It extended from beneath the umbilicus to the anterior border of the anus; it had begun in the prepuce ten years previously. [15.144] Clot-Bey [15.145] removed an elephantoid tumor of the scrotum weighing 80 pounds, performing castration at the same time. Alleyne [15.146] reports a case of elephantiasis, in which he successfully removed a tumor of the integuments of the scrotum and penis weighing 134 pounds.
Bicet [15.147] mentions a curious instance of elephantiasis of the penis and scrotum which had existed for five years. The subject was in great mental misery and alarm at his unsightly condition. The parts of generation were completely buried in the huge mass. An operation was performed in which all of the diseased structures that had totally unmanned him were removed, the true organs of generation escaping inviolate. Thebaud [15.148] mentions a tumor of the scrotum, the result of elephantiasis, which weighed 63 1/2 pounds. The weight was ascertained by placing the tumor on the scales, and directing the patient to squat over them without resting any weight of the body on the scales. This man could readily feel his penis, although his surgeons could not do so. The bladder was under perfect control, the urine flowing over a channel on the exterior of the scrotum, extending 18 inches from the meatus. Despite his infirmity this patient had perfect sexual desire, and occasional erections and emissions. A very interesting operation was performed with a good recovery.
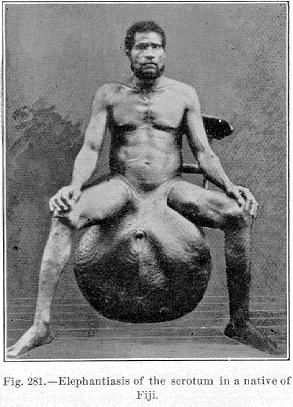
Partridge [15.149] reports an enormous scrotal tumor which was removed from a Hindoo of fifty-five, with subsequent recovery of the subject. The tumor weighed 111 1/2 pounds. The ingenious technic of this operation is well worth perusal by those interested. Goodman [15.150] successfully removed an elephantiasis of the scrotum from a native Fiji of forty-five. The tumor weighed 42 pounds, without taking into consideration the weight of the fluid
Figure 281 is taken from a photograph loaned to the authors by Dr. James Thorington. The patient was a native of Fiji, and was successfully operated on, with preservation of the testes. The tumor, on removal, weighed 120 pounds.
W. R. Browne, Surgeon-General, reports from the Madras General Hospital an operation on a patient of thirty-five with elephantoid scrotum of six years' duration. The proportions of the scrotum were as follows: Horizontally the circumference was six feet 6 1/2 inches, and vertically the circumference was six feet ten inches. The penis was wholly hidden, and the urine passed from an opening two feet 5 1/2 inches from the pubis. The man had complete control of his bladder, but was unable to walk. The operation for removal occupied one hour and twenty minutes, and the tumor removed weighed 124 3/4 pounds. Little blood was lost on account of an elastic cord tied about the neck of the tumor. and secured by
straps to a leather waist-belt. Recovery was prompt. Cody [15.151] speaks of the successful removal of a scrotal tumor weighing 56 pounds.
Fenger [15.152] describes a case of the foregoing nature in a German of twenty-three, a resident of Chicago. The growth had commenced eight years previously, and had progressively increased. There was no pain or active inflammation, and although the patient had to have especially constructed trousers he never ceased his occupation as a driver. The scrotum was represented by a hairless tumor weighing 22 pounds, and hanging one inch below the knees. No testicles or penis could be made out. Fenger removed the tumor, and the man was greatly improved in health. There was still swelling of the inguinal glands on both sides, but otherwise the operation
The statistics of this major operation show a surprisingly small mortality. Fayrer operated on 28 patients with 22 recoveries and six deaths, one from shock and five from pyemia The same surgeon collected 193 cases, and found the general mortality to be 18 per cent. According to Ashhurst, Turner, who practiced as a medical missionary in the Samoan Islands, claims to have operated 136 times with only two deaths. McLeod, Fayrer's successor in India, reported 129 cases with 23 deaths.
Early in this century Rayer described a case of elephantiasis in a boy of seventeen who, after several attacks of erysipelas, showed marked diminution of the elephantoid change; the fact shows the antagonism of the streptococcus erysipelatis to hypertrophic and malignant processes.
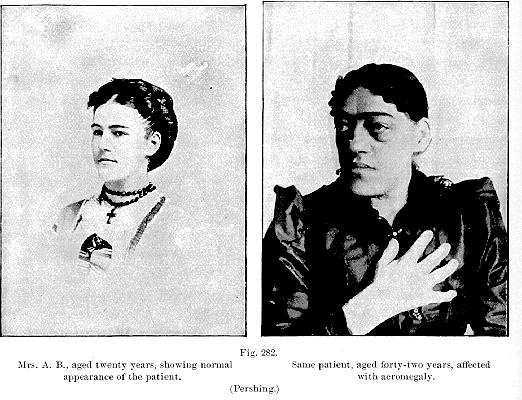
Acromegaly is a term introduced by Marie, and signifies large extremities. It is characterized by an abnormally large development of the extremities and of the features of the face,—the bony as well as the soft parts. In a well-marked case the hands and feet are greatly enlarged, but not otherwise deformed, and the normal functions are not disturbed. The hypertrophy involves all the tissues, giving a curious spade-like appearance to the hands. The feet are similarly enlarged, although the big toe may be relatively much larger. The nails also become broad and large. The face increases in volume and becomes elongated, in consequence of the hypertrophy of the superior and inferior maxillary bones. The latter often projects beyond the upper teeth. The teeth become separated, and the soft parts increase in size. The nose is large and broad, and the skin of the eyelids and ears is enormously hypertrophied. The tongue is greatly hypertrophied. The disease is of long duration, and late in the history the bones of the spine and thorax may acquire great deformity. As we know little of the influences and sources governing nutrition, the pathology and etiology of acromegaly are obscure. Marie regards the disease as a systemic dystrophy analogous to myxedema, due to a morbid condition of the pituitary body, just as myxedema is due to disease of the thyroid. In several of the cases reported the squint and optic atrophy and the amblyopia have pointed to the pituitary body as the seat of a new growth of hypertrophy. Pershing [15.153] shows a case of this nature (Fig. 282). The enlargement of the face and extremities was characteristic, and the cerebral and ocular symptoms pointed to the pituitary body as the seat of the lesion. Unverricht, Thomas, and Ransom *[843] report cases in which the ocular lesions, indicative of pituitary trouble, were quite prominent. Of 22 cases collected by Tamburini [15.154] 19 showed some change in the pituitary body, and in the remaining three cases either the diagnosis was uncertain or the disease was
Hersman [15.156] reports an interesting case of progressive enlargement of the
hands in a clergyman of fifty. Since youth he had suffered with pains in the joints. About three years before the time of report he noticed enlargement
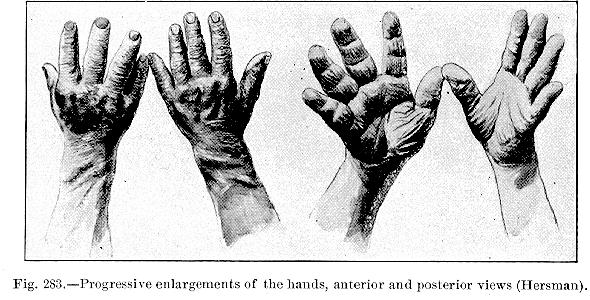
of the phalangeal joint of the third finger of the right hand. A short time later the whole hand became gradually involved and the skin assumed a darker
Chiromegaly is a term that has been applied by Charcot and Brissaud to the pseudoacromegaly that sometimes occurs in syringomyelia. Most of the cases that have been reported as a combination of these two diseases are now thought to be only a syringomyelia. A recent case is reported by Marie. *[789] In this connection it is interesting to notice a case of what might be called acute symptomatic transitory pseudoacromegaly, reported by Potovski: [15.157] In an insane woman, and without ascertainable cause, there appeared an enlargement of the ankles, wrists, and shoulders, and later of the muscles, with superficial trophic disturbances that gradually disappeared. The author excludes syphilis, tuberculosis, rheumatism, gout, hemophilia, etc., and considers it to have been a trophic affection of cerebral origin. Cases of pneumonia osteoarthropathy simulating acromegaly have been reported by Korn [15.158] and Murray. [15.159]
Megalocephaly, or as it was called by Virchow, leontiasis ossea, is due to a hypertrophic process in the bones of the cranium. The cases studied by Virchow were diffuse hyperostoses of the cranium. Starr [15.160] describes what he supposes to be a case of this disease, and proposes the title megalocephaly as preferable to Virchow's term, because the soft parts are also included in the hypertrophic process. A woman of fifty-two, married but having no children, and of negative family history, six years before the time of report showed the first symptoms of the affection, which began with formication in the finger-tips. This gradually extended to the shoulders, and was attended with some uncertainty of tactile sense and clumsiness of movement, but actual anesthesia had never been demonstrated. This numbness had not invaded the trunk or lower extremities, although there was slight uncertainty in the gait. There had been a slowly progressing enlargement of the head, face, and neck, affecting the bone, skin, and subcutaneous tissues, the first to the greatest degree. The circumference of the neck was 16 inches; the horizontal circumference of the head was 24 inches; from ear to ear, over the vertex, 16 inches; and from the root of the nose to the occipital protuberance, 16 inches. The cervical vertebræ were involved, and the woman had lost five inches in height. It may be mentioned here that Brissaud and Meige noticed the same loss in height, only more pronounced, in a case of gigantism, the loss being more than 15 inches. In Starr's case the tongue was normal and there was no swelling of the thyroid.
Cretinism is an endemic disease among mountainous people who drink largely of lime water, and is characterized by a condition of physical, physiologic, and mental degeneracy and nondevelopment, and possibly goiter. The
A quotation under our observation credits Colonel Sykes with the following statistics of cretinism, which show how in some locations it may be a decided factor of population. In December, 1845, in a population of 2,558,349 souls (the locality not mentioned), there were 18,462 people with simple goiter. Of the cretins without goiter there were 2089. Of cretins with goiter there were 3909; and cretins in which goiter was not stated 962, making a total of 6960. Of these 2185 had mere animal instincts; 3531 possessed very small intellectual faculties; 196 were almost without any; 1048 not classified. Of this number 2483 were born of healthy and sane fathers; 2285 from healthy mothers; 961 from goitrous fathers; 1267 from goitrous mothers; 49 from cretin fathers; 41 from cretin mothers; 106 from cretin fathers with goiter; 66 from cretin mothers with goiter; 438 fathers and 405 mothers were not specified.
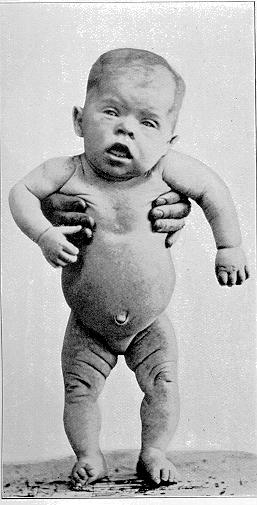
Sporadic cretinism, or congenital myzedema, is characterized by a congenital absence of the thyroid, diminutiveness of size, thickness of neck, shortness of arms and legs, prominence of the abdomen, large size of the face, thickness of the lips, large and protruding tongue, and imbecility or idiocy (Fig. 284). It is popularly believed that coitus during intoxication is the cause of this condition. Osler [15.161] was able to collect 11 or 12 cases in this country. The diagnosis is all-important, as the treatment by the thyroid extract produces the most noteworthy results. There are several remarkable
Myxedema proper is a constitutional condition due to the loss of the function of the thyroid gland. The disease was first described by Sir William Gull as a cretinoid change, and later by William Ord of London, who suggested the name. It is characterized clinically by a mxyedematous condition of the subcutaneous tissues and mental failure, and anatomically by atrophy of the thyroid gland. The symptoms of myxedema, as given by Ord, are marked increase in the general bulk of the body, a firm, inelastic swelling of the skin, which does not pit on pressure; dryness and roughness which tend, with swelling, to obliterate the lines of expression in the face; imperfect nutrition of the hair; local tumefaction of the skin and subcutaneous tissues, particularly in the supraclavicular region. The physiognomy is remarkably altered; the features are coarse and broad, the lips thick, the nostrils broad and thick, and the mouth enlarged. There is a striking slowness of thought and of movement; the memory fails, and conditions leading to incipient dementia intervene. The functions of the thoracic and abdominal organs seem to be normal,
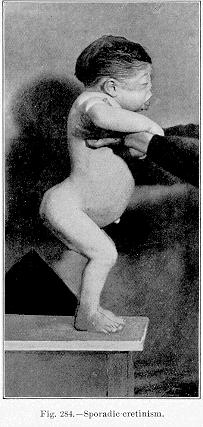
Fig. 284.—Sporadic cretinism.
[Description: Photograph of child with sporadic cretinism]
and death is generally due to some intercurrent disease, possibly tuberculosis. A condition akin to myxedema occurs after operative removal of the thyroid gland.
In a most interesting lecture Brissaud [15.163] shows the intimate relation between myxedema, endemic cretinism, sporadic cretinism, or myxedematous idiocy, and infantilism. He considers that they are all dependent upon an inherited or acquired deficiency or disease of the thyroid gland, and he presents cases illustrating each affection. Figure 285 shows a case of myxedema, one of myxedema in a case of arrested development—a transition case between myxedema
Cagots are an outcast race or clan of dwarfs in the region of the Pyrenees, and formerly in Brittany, whose existence has been a scientific problem since the sixteenth century, at which period they were known as Cagots, Gahets, Gafets, Agotacs, in France; Agotes or Gafos, in Spain; and Cacous, in Lower Brittany. Cagot meant the dog of a Goth; they were of supposed Gothic origin by some, and of Tartar origin by others. These people were formerly supposed to have been the descendants of lepers, or to have been the victims of leprosy themselves. From the descriptions there is a decided
difference between the Cagots and the cretins. In a recent issue of Cosmos a writer describes Cagots as follows:—
"They inhabit the valley of the Ribas in the northwestern part of the Spanish province now called Gerona. They never exceed 51 1/2 inches in height, and have short, ill-formed legs, great bellies, small eyes, flat noses, and pale, unwholesome complexions. They are usually stupid, often to the verge of idiocy, and much subject to goiter and scrofulous affections. The chief town of the Ribas Valley is Ribas, a place of 1500 inhabitants. about 800 feet above sea-level. The mountains rise about the town to a height of from 6000 to 8000 feet, and command an amazingly beautiful panorama of mountain, plain, and river, with Spanish cities visible upon the one side and French upon the other. The region is rich, both agriculturally

PLATE 11.
Case of infantile myxedema (West): the picture in the center represents the case after
six months' thyroid treatment; the picture on the right, after one
year's treatment.
[Description: Three photographs of an infant with myxedema]
"It is said that formal marriage is almost unknown among them. The women in some instances are employed in the village of Ribas as nurses for children, and as such are found tender and faithful. Before communication throughout the region was as easy as it is now, it was thought lucky to have one of these dwarfs in a family, and the dwarfs were hired out and even sold to be used in beggary in neighboring cities. There are somewhat similar dwarfs in other valleys of the Pyrenees, but the number is decreasing, and those of the Ribas Valley are reduced to a few individuals.''
Hiccough is a symptom due to intermittent, sudden contraction of the diaphragm. Obstinate cases are most peculiar, and sometimes exhaust the physician's skill. Symes divides these cases into four groups:—
(1) Inflammatory, seen particularly in inflammatory diseases of the viscera or abdominal membranes, and in severe cases of typhoid fever.
(2) Irritative, as in direct stimulus of the diaphragm in swallowing some very hot substance; local disease of the esophagus near the diaphragm, and in many conditions of gastric and intestinal disorder, more particularly those associated with flatus.
(3) Specific or idiopathic, in which there are no evident causes present; it is sometimes seen in cases of nephritis and diabetes.
(4) Neurotic, in which the primary cause is in the nervous system,—hysteria, epilepsy, shock, or cerebral tumors.
The obstinacy of continued hiccough has long been discussed. Osler calls to mind that in Plato's "Symposium'' the physician, Eryximachus, recommended to Aristophanes, who had hiccough from eating too much, either to hold his breath or to gargle with a little water; but if it still continued, "tickle your nose with something and sneeze, and if you sneeze once or twice even the most violent hiccough is sure to go.'' The attack must have been a severe one, as it is stated subsequently that the hiccough did not disappear until Aristophanes had excited the sneezing.
Among the older medical writers Weber speaks of singultus lasting for five days; Tulpius, *[842] for twelve days; Eller and Schenck, [15.164] for three months; Taranget, [15.165] for eight months; and Bartholinus, *[190] for four years.
At the present day it is not uncommon to read in the newspapers accounts of prolonged hiccoughing. These cases are not mythical, and are paralleled
Holston [15.166] reports a case of chronic singultus of seven years' standing. It had followed an attack of whooping-cough, and was finally cured apparently by the administration of strychnin. Cowan [15.167] speaks of a shoemaker of twenty-two who experienced an attack of constant singultus for a week, and then intermittent attacks for six years. Cowan also mentions instances of prolonged hiccough related by Heberden, Good, Hoffman, and Wartmouth. Barrett [15.168] is accredited with reporting a case of persistent hiccough in a man of thirty-five. Rowland [15.169] speaks of a man of thirty-five who hiccoughed for twelve years. The paroxysms were almost constant, and occurred once or twice a minute during the hours when the man was not sleeping. There was no noise with the cough. There is another case related in the same journal of a man who died on the fourth day of an attack of singultus, probably due to abscess of the diaphragm, which no remedy would relieve. Moore [15.170] records a case of a child, injured when young, who hiccoughed until about twenty years of age (the age at the time of report). Foot [15.171] mentions a lad of fifteen who, except when asleep, hiccoughed incessantly for twenty-two weeks, and who suffered two similar, but less severe, attacks in the summer of 1879, and again in 1880. The disease was supposed to be due to the habit of pressing the chest against the desk when at school. Dexter [15.172] reports a case of long-continued singultus in an Irish girl of eighteen, ascribed to habitual masturbation. There was no intermission in the paroxysm, which increased in force until general convulsions ensued. The patient said that the paroxysm could be stopped by firm pressure on the upper part of the external genital organs. Dexter applied firm pressure on her clitoris, and the convulsions subsided, and the patient fell asleep. They could be excited by firm pressure on the lower vertebræ. Corson [15.173] speaks of a man of fifty-seven who, after exposure to cold, suffered exhausting hiccough for nine days; and also records the case of an Irish servant who suffered hiccough for four months; the cause was ascribed to fright. Stevenson [15.174] cites a fatal instance of hiccough in a stone-mason of forty-four who suffered continuously from May 14th to May 28th. The only remedy that seemed to have any effect in this case was castor-oil in strong purgative doses.
Willard [15.175] speaks of a man of thirty-four who began to hiccough after an attack of pneumonia, and continued for eighty-six hours. The treatment consisted of the application of belladonna and cantharides plasters, bismuth, and lime-water, camphor, and salts of white hellebore inhaled through the nose in finest powder. Two other cases are mentioned by the same author. Gapper [15.176] describes the case of a young man who was seized with loud and distressing
Ranney [15.177] reports the case of an unmarried woman of forty-four who suffered from paroxysms of hiccough that persisted for four years. A peculiarity of this attack was that it invariably followed movements of the upper extremities. Tenderness and hyperesthesia over the spinous processes of the 4th, 5th, and 6th cervical vertebræ led to the application of the thermocautery, which, in conjunction with the administration of ergot and bromide, was attended with marked benefit, though not by complete cure. Barlow [15.178] mentions a man with a rheumatic affection of the shoulder who hiccoughed when he moved his joints. Barlow also recites a case of hiccough which was caused by pressure on the cicatrix of a wound in the left hand.
Beilby [15.179] reports a peculiar case in a girl of seventeen who suffered an anomalous affection of the respiratory muscle, producing a sound like a cough, but shriller, almost resembling a howl. It was repeated every five or six seconds during the whole of the waking moments, and subsided during sleep. Under rest and free purgation the patient recovered, but the paroxysms continued during prolonged intervals, and in the last six years they only lasted from twenty-four to forty-eight hours.
Parker [15.180] reports four rebellious cases of singultus successfully treated by dry cups applied to the abdomen. In each case it was necessary to repeat the operation after two hours, but recovery was then rapid. Tatevosoff reports a brilliant cure in a patient with chronic chest trouble, by the use of common snuff, enough being given several times to induce lively sneezing. Griswold [15.181] records a successful treatment of one case in a man of fifty, occurring after a debauch, by the administration of glonoin, 1/150 of a grain every three hours. Heidenhain [15.182] records a very severe and prolonged case caused, as shown later at the operation and postmortem examination, by carcinoma of the pancreas. The spasms were greatly relieved by cocain administered by the mouth, as much as 15 grains being given in twelve hours. Laborde and Lépine [15.183] report the case of a young girl who was relieved of an obstinate case of hiccough lasting four days by traction on her tongue. After the tongue had been held out of the mouth for a few minutes the hiccoughs ceased. Laborde referred to two cases of a similar character reported by Viand.
Anomalous Sneezing.—In the olden times sneezing was considered a good omen, and was regarded as a sacred sign by nearly all of the ancient peoples. This feeling of reverence was already ancient in the days of Homer. Aristotle inquired into the nature and origin of the superstition, somewhat profanely wondering why sneezing had been deified rather than coughing. The Greeks traced the origin of the sacred regard for sneezing to the
There are some curious cases of anomalous sneezing on record, some of which are possibly due to affections akin to our present "hay fever,'' while others are due to causes beyond our comprehension. The Ephemerides records a paroxysm of continual sneezing lasting thirty days. Bonet, *[216] Lancisi, *[475] Fabricius Hildanus, *[334] and other older observers speak of sneezing to death. Morgagni *[576] mentions death from congestion of the vasa cerebri caused by sneezing. The Ephemerides records an instance of prolonged sneezing which was distinctly hereditary.
Ellison [15.184] makes an inquiry for treatment of a case of sneezing in a white child of ten. The sneezing started without apparent cause and would continue 20 or 30 times, or until the child was exhausted, and then stop for a half or one minute, only to relapse again. Beilby [15.185] speaks of a boy of thirteen who suffered constant sneezing (from one to six times a minute) for one month. Only during sleep was there any relief. The patient recovered under treatment consisting of active leeching, purgation, and blisters applied behind the ear, together with the application of olive oil to the nostrils.
Lee [15.186] reports a remarkable case of yawning followed by sneezing in a girl of fifteen who, just before, had a tooth removed without difficulty. Half an hour afterward yawning began and continued for five weeks continuously. There was no pain, no illness, and she seemed amused at her condition. There was no derangement of the sexual or other organs and no account of an hysteric spasm. Potassium bromid and belladonna were administered for a few days with negative results, when the attacks of yawning suddenly turned to sneezing. One paroxysm followed another with scarcely an interval for speech. She was chloroformed once and the sneezing ceased, but was more violent on recovery therefrom. Ammonium bromid in half-drachm doses, with rest in bed for psychologic reasons, checked the sneezing. Woakes [15.187] presented a
A case of anomalous sneezing immediately prior to sexual intercourse is mentioned on page 511.
Hemophilia is an hereditary, constitutional fault, characterized by a tendency to uncontrollable bleeding, either spontaneous or from slight wounds. It is sometimes associated with a form of arthritis (Ogler). This hemorrhagic diathesis has been known for many years; and the fact that there were some persons who showed a peculiar tendency to bleed after wounds of a trifling nature is recorded in some of the earliest medical literature. Only recently, however, through the writings of Buel, Otto, Hay, Coates, and others, has the hereditary nature of the malady and its curious mode of transmission through the female line been known. As a rule the mother of a hemophile is not a "bleeder'' herself, but is the daughter of one. The daughters of a hemophile, though healthy and free from any tendency themselves, are almost certain to transmit the disposition to the male offspring. The condition generally appears after some slight injury in the first two years of life; but must be distinguished from the hemorrhagic affections of the new-born, which will be discussed later. The social condition of the family does not alter the predisposition; the old Duke of Albany was a "bleeder''; [15.188] and bleeder families are numerous, healthy looking, and have fine, soft skins.
The duration of this tendency, and its perpetuation in a family, is remarkable. The Appleton-Swain family of Reading, Mass., has shown examples for two centuries. Osler has been advised of instances already occurring in the seventh generation. Kolster [15.189] has investigated hemophilia in women, and reports a case of bleeding in the daughter of a hemophilic woman. He also analyzes 50 genealogic trees of hemophilic families, and remarks that Nasse's law of transmission does not hold true. In 14 cases the transmission was direct from the father to the child, and in 11 cases it was direct from the mother to the infant.
The hemorrhagic symptoms of bleeders may be divided into external bleedings, either spontaneous or traumatic; interstitial bleedings, petechiæ, and ecchymoses; and the joint-affections. The external bleedings are seldom spontaneous, and generally follow cuts, bruises, scratches, and often result seriously. A minor operation on a hemophile may end in death; so slight an operation as drawing a tooth has been followed by the most disastrous consequences.
Mackenzie [15.196] reports an instance of hemophilic purpura of the retina, followed by death. Harkin gives an account of vicarious bleeding from the under lip in a woman of thirty-eight. The hemorrhage occurred at every meal and lasted ten minutes. There is no evidence that the woman was of hemophilic descent.
Of 334 cases of bleeding in hemophilia collected by Grandidier, 169 were from the nose, 43 from the mouth, 15 from the stomach, 36 from the bowels, 16 from the urethra, 17 from the lungs, and a few from the skin of the head, eyelids, scrotum, navel, tongue, finger-tips, vulva, and external ear. Osler remarks that Professor Agnew knew of a case of a bleeder who had always bled from cuts and bruises above the neck, never from those below. The joint-affections closely resemble acute rheumatism. Bleeders do not necessarily die of their early bleedings, some living to old age. Oliver Appleton, the first reported American bleeder, died at an advanced age, owing to hemorrhage from a bed-sore and from the urethra. Fortunately the functions of menstruation and parturition are not seriously interfered with in hemophilia. Menstruation is never so excessive as to be fatal. Grandidier states that of 152 boy subjects 81 died before the termination of the seventh year. Hemophilia is rarely fatal in the first year.
Of the hemorrhagic diseases of the new-born three are worthy of note. In syphilis hæmorrhagica neonatorum the child may be born healthy, or just after birth there may appear extensive cutaneous extravasations with bleeding from the mucous surfaces and from the navel; the child may become deeply jaundiced. Postmortem examination shows extensive extravasations into the internal viscera, and also organic syphilitic lesions.
Winckel's disease, or epidemic hemoglobinuria, is a very fatal affection,
Apart from the common visceral hemorrhages, the results of injuries at birth, bleeding from one or more of the surfaces is a not uncommon event in the new-born, particularly in hospital-practice. According to Osler Townsend reports 45 cases in 6700 deliveries, the hemorrhage being both general and from the navel alone. Bleeding also occurs from the bowels, stomach, and mouth, generally beginning in the first week, but in rare instances it is delayed to the second or third. Out of 50 cases collected by Townsend 31 died and 19 recovered. The nature of the disease is unknown, and postmortem examination reveals no pathologic changes, although the general and not local nature of the affection, its self-limited character, the presence of fever, and the greater prevalence of the disease in hospitals, suggest an infectious origin (Townsend). Kent [15.197] speaks of a new-born infant dying of spontaneous hemorrhage from about the hips.
Infantile scurvy, or Barlow's disease, has lately attracted marked attention, and is interesting for the numerous extravasations and spontaneous hemorrhages which are associated with it. A most interesting collection of specimens taken from the victims of Barlow's disease were shown in London in 1895. *[619]
In an article on the successful preventive treatment of tetanus neonatorum, or the "scourge of St. Kilda,'' of the new-born, Turner [15.198] says the first mention of trismus nascentium or tetanus neonatorum was made by Rev. Kenneth Macaulay in 1764, after a visit to the island of St. Kilda in 1758. This gentleman states that the infants of this island give up nursing on the fourth or fifth day after birth; on the seventh day their gums are so clinched together that it is impossible to get anything down their throats; soon after this they are seized with convulsive fits and die on the eighth day. So general was this trouble on the island of St. Kilda that the mothers never thought of making any preparation for the coming baby, and it was wrapped in a dirty piece of blanket till the ninth or tenth day, when, if the child survived, the affection of the mother asserted itself. This lax method of caring for the infant, the neglect to dress the cord, and the unsanitary condition of the dwellings, make it extremely probable that the infection was through the umbilical cord. All cases in which treatment was properly carried out by competent nurses have survived. This treatment consisted in dressing the cord with iodoform powder and antiseptic wool, the breast-feeding of the baby from the first, and the administration of one-grain doses of potassium bromid at short intervals. The infant death-rate on the island of St. Kilda has, consequently,
Human Parasites.—Worms in the human body are of interest on account of the immense length some species attain, the anomalous symptoms which they cause, or because of their anomalous location and issue. According to modern writers the famous Viennese collection of helminths contains chains of tenia saginata 24 feet long. The older reports, according to which the tænia solium (i. e., generally the tænia saginata) grew to such lengths as 40, 50, 60, and even as much as 800 yards, are generally regarded as erroneous. The observers have apparently taken the total of all the fragments of the worm or worms evacuated at any time and added them, thus obtaining results so colossal that it would be impossible for such an immense mass to be contained in any human intestine.
The name solium has no relation to the Latin solus, or solium. It is quite possible for a number of tapeworms to exist simultaneously in the human body. Palm [15.199] mentions the fact of four tapeworms existing in one person; and Mongeal [15.200] has made observations of a number of cases in which several teniæ existed simultaneously in the stomach. David [15.201] speaks of the expulsion of five teniæ by the ingestion of a quantity of sweet wine. Cobbold [15.202] reports the case of four simultaneous tapeworms; and Aguiel [15.203] describes the case of a man of twenty-four who expelled a mass weighing a kilogram, 34.5 meters long, consisting of several different worms. Garfinkel *[812] mentions a case which has been extensively quoted, [15.204] of a peasant who voided 238 feet of tapeworms, 12 heads being found. Laveran [15.205] reports a case in which 23 teniæ were expelled in the same day. Greenhow [15.206] mentions the occurrence of two teniæ mediocanellata.
The size of a tapeworm in a small child is sometimes quite surprising. Even the new-born have exhibited signs of teniæ, and Haussmann [15.207] has discussed this subject. Armor [15.208] speaks of a fully-matured tapeworm being expelled from a child five days old. Kennedy [15.209] reports cases in which tapeworms have been expelled from infants five, and five and one-half months old. Heisberg [15.210] gives an account of a tapeworm eight feet in length which came from a child of two. Twiggs [15.211] describes a case in which a tapeworm 36 feet long was expelled from a child of four; and Fabre [15.212] mentions the expulsion of eight teniæ from a child. Occasionally the tapeworm is expelled from the mouth. Such cases are mentioned by Hitch [15.213] and Martel. [15.214] White [15.215] speaks of a tapeworm which was discharged from the stomach
The peculiar effects of a tapeworm are exaggerated appetite and thirst, nausea, headaches, vertigo, ocular symptoms, cardiac palpitation, and Mursinna [15.217] has even observed a case of trismus, or lockjaw, due to tænia solium. Fereol [15.218] speaks of a case of vertigo, accompanied with epileptic convulsions, which was caused by teniæ. On the administration of kousso three heads were expelled simultaneously. There is a record of an instance of cardiac pulsation rising to 240 per minute, which ceased upon the expulsion of a large tapeworm. [15.219] It is quite possible for the presence of a tapeworm to indirectly produce death. Garroway [15.220] describes a case in which death was apparently imminent from the presence of a tapeworm. Kisel [15.221] has recorded a fatal case of anemia, in a child of six, dependent on teniæ.
The number of ascarides or round-worms in one subject is sometimes enormous. Victor [15.222] speaks of 129 round-worms being discharged from a child in the short space of five days. Pole [15.223] mentions the expulsion of 441 lumbricoid worms in thirty-four days, and Fauconneau-Dufresne [15.224] has reported a most remarkable case in which 5000 ascarides were discharged in less than three years, mostly by vomiting. The patient made an ultimate recovery.
There are many instances in which the lumbricoid worms have pierced the intestinal tract and made their way to other viscera, sometimes leading to an anomalous exit. There are several cases on record in which the lumbricoid worms have been found in the bladder. Paré speaks of a case of this kind during a long illness; and there is mention [15.225] of a man who voided a worm half a yard long from his bladder after suppression of urine. The Ephemerides contains a curious case in which a stone was formed in the bladder, having for its nucleus a worm. Fontanelle presented to the Royal Academy of Medicine of Paris several yards of tapeworm passed from the urethra of a man of fifty-three. The following is a quotation from the British Medical Journal: [15.226] " I have at present a patient passing in his urine a worm-like body, not unlike a tapeworm as far as the segments and general appearance are concerned, the length of each segment being about 1/4 inch, the breadth rather less; sometimes 1 1/2 segments are joined together. The worm is serrated on the one side, each segment having 1 1/2 cusps. The urine pale, faintly acid at first, within the last week became almost neutral. There was considerable vesical irritation for the first week, with abundant mucus in the urine, specific gravity was 1010; there were no albumin nor tube-casts nor uric acid
Other cases of worms in the bladder are mentioned in Chapter XIII.
Mitra [15.227] speaks of the passage of round-worms through the umbilicus of an adult; and there is a case mentioned [15.228] in which round-worms about seven inches long were voided from the navel of a young child. Borgeois [15.229] speaks of a lumbricoid worm found in the biliary passages, and another in the air passages.
Turnbull [15.230] has recorded two cases of perforation of the tympanic membrane from lumbricoides. Dagan [15.231] speaks of the issue of a lumbricoid from the external auditory meatus. Laughton [15.232] reports an instance of lumbricoid in the nose. Rake [15.233] speaks of asphyxia from a round-worm. Morland [15.234] mentions the ejection of numerous lumbricoid worms from the mouth.
Worms have been found in the heart; and it is quite possible that in cases of trichinosis, specimens of the trichinæ may be discovered anywhere in the line of cardiac or lymphatic circulation. Quoted by Fournier, *[302] Lapeyronnie has seen worms in the pericardial sac, and also in the ventricle. There is an old record of a person dying of intestinal worms, one of which was found in the left ventricle. [15.235] à Castro and Vidal speak of worms in the aorta. Rake [15.236] reports a case of sudden death from round-worm; and Brown [15.237] has noted a similar instance.
The echinococcus is a tiny cestode which is the factor in the production of the well-known hydatid cysts which may be found in any part of the body. Delafield and Prudden report the only instance of multilocular echinococcus seen in this country. Their patient was a German who had been in this country five years. There are only about 100 of these cases on record, most of them being in Bavaria and Switzerland.
The filaria sanguinis hominis is a small worm of the nematode species, the adult form of which lives in the lymphatics, and either the adult or the prematurely discharged ova (Manson) block the lymph-channels, producing the conditions of hematochyluria, elephantiasis, and lymph-scrotum. The Dracunculus medinensis or Guinea-worm is a widely-spread parasite in parts of Africa and the West Indies. According to Osler several cases have occurred in the United States. Jarvis reports a case in a post-chaplain who had lived at Fortress Monroe, Va., for thirty years. Van Harlingen's patient, a man of forty-seven, had never lived out of Philadelphia, so that the worm must be included among the parasites infesting this country.
Curran [15.238] gives quite an exhaustive article on the disease called in olden times "eaten of worms,''—a most loathsome malady. Herod the Great, the Emperor Galerius, and Philip II. of Spain perished from it. In speaking of the Emperor Galerius, Dean Milman, in his "History of Latin Christianity,'' [15.239] says, "a deep and fetid ulcer preyed on the lower parts of his body and ate them away into a mass of living corruption.'' Gibbon, in his "Decline and Fall,'' [15.240] also says that "his (Galerius's) death was caused by a very painful and lingering disorder. His body, swelled by an intemperate course of life to an unwieldy corpulence, was covered with ulcers and devoured by immense swarms of those insects who have given their names to this most loathsome disease.'' It is also said that the African Vandal King, the Arian Huneric, died of the disease. Antiochus, surnamed the "Madman,'' [15.241] was also afflicted with it; and Josephus makes mention of it as afflicting the body of Herod the Great. The so-called "King Pym'' died of this "morbus pedicularis,'' but as prejudice and passion militated against him during his life and after his death, this fact is probably more rumor than verity. A case is spoken of by Curran, which was seen by an army-surgeon in a very aged woman in the remote parts of Ireland, and another in a female in a dissecting-room in Dublin. The tissues were permeated with lice which emerged through rents and fissures in the body.
Instances of the larvæ of the estrus or the bot-fly in the skin are not uncommon. In this country Allen [15.242] removed such larvæ from the skin of the neck, head, and arm of a boy of twelve. Bethune, Delavigne, Howship, Jacobs, Jannuzzi and others, report similar cases. These flesh-flies are called creophilæ, and the condition they produce is called myiosis. According to Osler, in parts of Central America, the eggs of a bot-fly, called the dermatobia, are not infrequently deposited in the skin, and produce a swelling very like the ordinary boil. Matas has described a case in which the estrus larvæ were found in the gluteal region. Finlayson of Glasgow has recently reported an interesting case in a physician who, after protracted constipation and pain in the back and sides, passed large numbers of the larvæ of the flower-fly, anthomyia cani-cularis, and there are other instances of myiosis interna from swallowing the larvæ of the common house-fly.
There are forms of nasal disorder caused by larvæ, which some native surgeons in India regard as a chronic and malignant ulceration of the mucous
| CHAPTER XV.
ANOMALOUS TYPES AND INSTANCES OF
DISEASE. Anomalies and Curiosities of Medicine | ||