| CHAPTER XIII.
SURGICAL ANOMALIES OF THE GENITOURINARY
SYSTEM. Anomalies and Curiosities of Medicine | ||
13. CHAPTER XIII.
SURGICAL ANOMALIES OF THE GENITOURINARY
SYSTEM.
Wounds of the kidney may be very severe without causing death, and even one entire kidney may be lost without interfering with the functions of life. Marvand,[13.1] the Surgeon-Major of an Algerian regiment, reports the case of a young Arab woman who had been severely injured in the right lumbar region by a weapon called a "yataghan,'' an instrument which has only one cutting edge. On withdrawing this instrument the right kidney was extruded, became strangulated between the lips of the wound, and caused considerable hemorrhage. A ligature was put around the base of the organ, and after some weeks the mass separated. The patient continued in good health the whole time, and her urinary secretion was normal. She was discharged in two months completely recovered. Price [13.2] mentions the case of a groom who was kicked over the kidney by a horse, and eighteen months later died of dropsy. Postmortem examination showed traces of a line of rupture through the substance of the gland; the preparation was deposited in St. George's Hospital Museum in London. The case is singular in that this man, with granular degeneration of the kidney, recovered from so extensive a lesion, and, moreover, that he remained in perfect health for over a year with his kidney in a state of destructive disease. Borthwick [13.3] mentions a dragoon of thirty who was stabbed by a sword-thrust on the left side under the short rib, the sword penetrating the pelvis and wounding the kidney. There was no hemorrhage from the external wound, nor pain in the spermatic cord or testicle. Under expectant treatment the man recovered. Castellanos [13.4] mentions a case of recovery from punctured wound of the kidney by a knife that penetrated the tubular and cortical substance, and entered the pelvis of the organ. The case was peculiar in the absence of two symptoms, viz., the escape of urine from the wound, and retraction of the corresponding testicle. Dusenbury [13.5] reports the case of a corporal in the army who was wounded on April 6, 1865, the bullet entering both the liver and kidney. Though there was injury to both these important organs, there was no impairment of the patient's health, and he recovered.
Ward [13.8] mentions a case of ruptured kidney, caused by a fall of seven feet, the man recovering after appropriate treatment. Vernon [13.9] reports a case of serious injury to the kidney, resulting in recovery in nine weeks. The patient fell 40 feet, landing on some rubbish and old iron, and received a wound measuring six inches over the right iliac crest, through which the lower end of the right kidney protruded; a piece of the kidney was lost. The case was remarkable because of the slight amount of hemorrhage.
Nephrorrhaphy is an operation in which a movable or floating kidney is fixed by suture through its capsule, including a portion of kidney-substance, and then through the adjacent lumbar fascia and muscles. The ultimate results of this operation have been most successful.
Nephrolithotomy is an operation for the removal of stone from the kidney. The operation may be a very difficult one, owing to the adhesions and thickening of all the perinephric tissues, or to the small size or remote location of the stone.
There was a recent exhibition in London, *[619] in which were shown the results of a number of recent operations on the kidney. There was one-half of a kidney that had been removed on account of a rapidly-growing sarcoma from a young man of nineteen, who had known of the tumor for six months; there was a good recovery, and the man was quite well in eighteen months afterward. Another specimen was a right kidney removed at St. Bartholomew's Hospital. It was much dilated, and only a small amount of the kidney-substance remained. A calculus blocked the ureter at its commencement. The patient was a woman of thirty-one, and made a good recovery. From the Middlesex Hospital was a kidney containing a uric acid calculus which was successfully removed from a man of thirty-five. From the Cancer Hospital at Brompton there were two kidneys which had been removed from a man and a woman respectively, both of whom made a good recovery. From the King's College Hospital there was a kidney with its pelvis enlarged and occupied by a large calculus, and containing little secreting substance, which was removed from a man of forty-nine, who recovered. These are only a few of the examples of this most interesting collection. Large calculi of the kidney are mentioned in Chapter XV.
Rupture of the ureter is a very rare injury. Poland [13.10] has collected
There are a few recorded cases of uncomplicated wounds of the ureters. The only well authenticated case in which the ureter alone was divided is the historic injury of the Archbishop of Paris, [13.11] who was wounded during the Revolution of 1848, by a ball entering the upper part of the lumbar region close to the spine. Unsuccessful attempts were made to extract the ball, and as there was no urine in the bladder, but a quantity escaping from the wound, a diagnosis of divided ureter was made. The Archbishop died in eighteen hours, and the autopsy showed that the ball had fractured the transverse process of the 3d lumbar vertebra, and divided the cauda equina just below its origin; it had then changed direction and passed up toward the left kidney, dividing the ureter near the pelvis, and finally lodged in the psoas muscle.
It occasionally happens that the ureter is wounded in the removal of uterine, ovarian, or other abdominal tumors. In such event, if it is impossible to transplant to the bladder, the divided or torn end should be brought to the surface of the loin or vagina, and sutured there. In cases of malignant growth, the ureter has been purposely divided and transplanted into the bladder. Penrose, [13.12] assisted by Baldy, has performed this operation after excision of an inch of the left ureter for carcinomatous involvement. The distal end of the ureter was ligated, and the proximal end implanted in the bladder according to Van Hook's method, which consists in tying the lowered end of the ureter, then making a slit into it, and invaginating the upper end into the lower through this slit. A perfect cure followed. Similar cases have been reported by Kelly, Krug, and Bache Emmet. [13.13] Reed [13.14] reports a most interesting series in which he has successfully transplanted ureters into the rectum.
Ureterovaginal fistulæ following total extirpation of the uterus, opening of pelvic abscesses, or ulcerations from foreign bodies, are repaired by an operation termed by Bazy of Paris ureterocystoneostomy, and suggested by him as a substitute for nephrectomy in those cases in which the renal organs are unaffected. In the repair of such a case after a vaginal hysterectomy Mayo [13.15] reports a successful reimplantation of the ureter into the bladder.
Stricture of the ureter is also a very rare occurrence except as a result of compression of abdominal or pelvic new growths. Watson [13.16] has, however, reported two cases of stricture, in both of which a ureter was nearly or quite
A remarkable procedure recently developed by gynecologists, particularly by Kelly of Baltimore, is catheterization and sounding of the ureters. McClellan [13.17] records a case of penetration of the ureter by the careless use of a catheter.
Injuries of the Bladder.—Rupture of the bladder may result from violence without any external wound (such as a fall or kick) applied to the abdomen. Jones [13.18] reports a fatal case of rupture of the bladder by a horse falling on its rider. In this case there was but little extravasation of urine, as the vesical aperture was closed by omentum and bowel. Assmuth reports two cases of rupture of the bladder from muscular action. Morris [13.19] cites the history of a case in which the bladder was twice ruptured: the first time by an injury, and the second time by the giving way of the cicatrix. The patient was a man of thirty-six who received a blow in the abdomen during a fight in a public house on June 6, 1879. At the hospital his condition was diagnosed and treated expectantly, but he recovered perfectly and left the hospital July 10, 1879. He was readmitted on August 4, 1886, over seven years later, with symptoms of rupture of the bladder, and died on the 6th. The postmortem showed a cicatrix of the bladder which had given way and caused the patient's death.
Rupture of the bladder is only likely to happen when the organ is distended, as when empty it sinks behind the pubic arch and is thus protected from external injury. The rupture usually occurs on the posterior wall, involving the peritoneal coat and allowing extravasation of urine into the peritoneal cavity, a condition that is almost inevitably fatal unless an operation is performed. Bartels collected the data of 98 such cases, only four recovering. When the rent is confined to the anterior wall of the bladder the urine escapes into the pelvic tissues, and the prognosis is much more favorable. Bartels collected 54 such cases, 12 terminating favorably. When celiotomy is performed for ruptured bladder, in a manner suggested by the elder Gross, the mortality is much less. Ashhurst collected the reports of 28 cases thus treated, ten of which recovered—a mortality of 64.2 per cent. Ashhurst remarks that he has seen an extraperitoneal rupture of the anterior wall of the bladder caused by improper use of instruments, in the case of retention of urine due to the presence of a tight urethral stricture.
There are a few cases on record in which the bladder has been ruptured by distention from the accumulation of urine, but the accident is a rare one, the urethra generally giving way first. Coats [13.20] reports two cases of uncomplicated rupture of the bladder. In neither case was a history of injury obtainable.
Gunshot Wounds of the Bladder.—Jackson [13.22] relates the remarkable recovery of a private in the 17th Tennessee Regiment who was shot in the pelvis at the battle of Mill Springs or Fishing Creek, Ky. He was left supposedly mortally wounded on the field, but was eventually picked up, and before receiving any treatment hauled 164 miles, over mountainous roads in the midst of winter and in a wagon without springs. His urine and excretions passed out through the wounds for several weeks and several pieces of bone came away. The two openings eventually healed, but for twenty-two months he passed pieces of bone by the natural channels.
Eve [13.23] records the case of a private in the Fifth Tennessee Cavalry who was shot in the right gluteal region, the bullet penetrating the bladder and making its exit through the pubis. He rode 30 miles, during which the urine passed through the wound. Urine was afterward voided through the left pubic opening, and spicules of bone were discharged for two years afterward; ultimate recovery ensued.
Barkesdale [13.24] relates the history of the case of a Confederate soldier who was shot at Fredericksburg in the median line of the body, 1 1/2 inches above the symphysis, the wound of exit being in the median line at the back, 1/2 inch lower down. Urine escaped from both wounds and through the urethra. There were no bad symptoms, and the wounds healed in four weeks.
The bladder is not always injured by penetration of the abdominal wall, but may be wounded by penetration through the anus or vagina, or even by an instrument entering the buttocks and passing through the smaller sacrosciatic notch. Camper [13.25] records the case of a sailor who fell from a mast and struck upon some fragments of wood, one of which entered the anus and penetrated the bladder, the result being a rectovesical fistula. About a year later the man consulted Camper, who unsuccessfully attempted
Couper [13.28] reports a fatal case of stab-wound of the buttocks, in which the knife passed through the lesser sacrosciatic notch and entered the bladder close to the trigone. The patient was a man of twenty-three, a seaman, and in a quarrel had been stabbed in the buttocks with a long sailor's knife, with resultant symptoms of peritonitis which proved fatal. At the autopsy it was found that the knife had passed through the gluteal muscles and divided part of the great sacrosciatic ligament. It then passed through the small sacrosciatic notch, completely dividing the pudic artery and nerve, and one vein, each end being closed by a clot. The knife entered the bladder close to the trigone, making an opening large enough to admit the index finger. There were well-marked evidences of peritonitis and cellulitis.
Old-time surgeons had considerable difficulty in extracting arrow-heads from persons who had received their injuries while on horseback. Conrad Gesner records an ingenious device of an old surgeon who succeeded in extracting an arrow which had resisted all previous attempts, by placing the subject in the very position in which he was at the time of reception of the wound. The following noteworthy case shows that the bladder may be penetrated by an arrow or bullet entering the buttocks of a person on horseback. Forwood [13.29] describes the removal of a vesical calculus, the nucleus of which was an iron arrow-head, as follows: "Sitimore, a wild Indian, Chief of the Kiowas, aged forty-two, applied to me at Fort Sill, Indian Territory, August, 1869, with symptoms of stone in the bladder. The following history was elicited: In the fall of 1862 he led a band of Kiowas against the Pawnee Indians, and was wounded in a fight near Fort Larned, Kansas. Being mounted and leaning over his horse, a Pawnee, on foot and within a
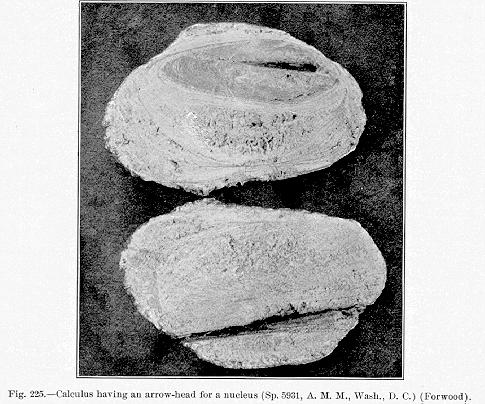
in the accompanying photograph (Fig. 225), showing a cross-section of the calculus with the arrow-head in situ.
As quoted by Chelius, *[265] both Hennen and Cline relate cases in which men have been shot through the skirts of the jacket, the ball penetrating the abdomen above the tuberosity of the ischium, and entering the bladder, and the men have afterward urinated pieces of clothing, threads, etc., taken in by the ball. In similar cases the bullet itself may remain in the bladder and cause the formation of a calculus about itself as a nucleus, as in three cases mentioned by McGuire of Richmond, or the remnants of cloth or spicules of bone may give rise to similar formation.
In cases in which there is a fistula of the bladder the subject may live for some time, in some cases passing excrement through the urethra, in others, urine by the anus. These cases seem to have been of particular interest to the older writers, and we find the literature of the last century full of examples. Benivenius, Borellus, the Ephemerides, Tulpius, Zacutus Lusitanus, and others speak of excrement passing through the penis; and there are many cases of vaginal anus recorded. Langlet cites an instance in which the intestine terminated in the bladder. Arand *[154] mentions recovery after atresia of the anus with passage of excrement from the vulva. Bartholinus, the Ephemerides, Fothergill, [13.32] de la Croix, [13.33] Riedlin, *[683] Weber, and Zacutus Lusitanus mention instances in which gas was passed by the penis and urethra. Camper [13.34] records such a case from ulcer of the neighboring or connecting intestine; Frank, from cohesion and suppuration of the rectum; Marcellus Donatus, [13.35] from penetrating ulcer of the rectum; and Petit, [13.36] from communication of the rectum and bladder in which a cure was effected by the continued use of the catheter for the evacuation of urine.
Flatus through the vagina, vulva, and from the uterus is mentioned by Bartholinus, the Ephemerides, Meckel, Mauriceau, Paullini, Riedlin, Trnka, and many others in the older literature. Dickinson [13.37] mentions a Burmese male child, four years old, who had an imperforate anus and urethra, but who passed feces and urine successfully through an opening at the base
In the older literature it was not uncommon to find accounts of persons passing worms from the bladder, no explanations being given to account for their presence in this organ. Some of these cases were doubtless instances of echinococcus, trichinæ, or the result of rectovesical fistula, but Riverius [13.38] mentions an instance in which, after drinking water containing worms, a person passed worms in the urine. In the old Journal de physique de Rozier is an account of a man of forty-five who enjoyed good health, but who periodically urinated small worms from the bladder. They were described as being about 1 1/2 lines long, and caused no inconvenience. There is also mentioned [13.39] the case of a woman who voided worms from the bladder. Tupper [13.40] describes a curious case of a woman of sixty-nine who complained of a severe, stinging pain that completely overcame her after micturition. An ulceration of the neck of the bladder was suspected, and the usual remedies were applied, but without effect. An examination of the urine was negative. On recommendation of her friends the patient, before going to bed, steeped and drank a decoction of knot-grass. During the night she urinated freely, and claimed that she had passed a worm about ten inches long and of the size of a knitting-needle. It exhibited motions like those of a snake, and was quite lively, living five or six days in water. The case seems quite unaccountable, but there is, of course, a possibility that the animal had already been in the chamber, or that it was passed by the bowel. A rectovaginal or vesical fistula could account for the presence of this worm had it been voided from the bowel; nevertheless the woman adhered to her statement that she had urinated the worm, and, as confirmatory evidence, never complained of pain after passing the animal.
Foreign bodies in the bladder, other than calculi (which will be spoken of in Chapter XV.), generally gain entrance through one of the natural passages, as a rule being introduced, either in curiosity or for perverted satisfaction, through the urethra. Morand mentions an instance in which a long wax taper was introduced into the bladder through the urethra by a man. At the University Hospital, Philadelphia, White has extracted, by median cystotomy, a long wax taper which had been used in masturbation. The cystoscopic examination in this case was negative, and the man's statements were disbelieved, but the operation was performed, and the taper was found curled up and covered by mucus and folds of the bladder. It is not uncommon for needles, hair-pins, and the like to form nuclei for incrustations. Gross found three caudal vertebræ of a squirrel in the center of a vesical calculus taken from the bladder of a man of thirty-five. It was afterward elicited that the patient had practiced urethral masturbation with the tail of this animal. Morand *[563] relates the history of a man of sixty-two who introduced a sprig of wheat into his urethra for a supposed therapeutic purpose.
Among females, whose urethræ are short and dilatable, foreign bodies are often found in the bladder, and it is quite common for smaller articles of the toilet, such as hair-pins, to be introduced into the bladder, and there form calculi. Whiteside [13.46] describes a case in which a foreign body introduced into the bladder was mistaken for pregnancy, and giving rise to corresponding symptoms. The patient was a young girl of seventeen who had several times missed her menstruation, and who was considered pregnant. The abdomen was more developed than usual in a young woman. The breasts were voluminous, and the nipples surrounded by a somber areola. At certain periods after the cessation of menstruation, she had incontinence of urine, and had also repeatedly vomited. The urine was of high specific gravity, albuminous, alkaline, and exhaled a disagreeable odor. In spite of the signs of pregnancy already noted, palpitation and percussion did not show any augmentation in the size of the uterus, but the introduction of a catheter into the bladder showed the existence of a large calculus. Under chloroform the calculus and its nucleus were disengaged, and proved to be the handle of a tooth-brush, the exact size of which is represented in the accompanying illustration (Fig. 226). The handle was covered with calcareous deposits, and was tightly fixed in the bladder. At first the young woman would give no explanation for its presence, but afterward explained that she had several times used this instrument for relief in retention of urine, and one day it had fallen
There are peculiar cases of hair in the bladder, in which all history as to the method of entrance is denied, and which leave as the only explanation the possibility that the bladder was in communication with some dermoid cyst. Hamelin [13.49] mentions a case of this nature. It is said [13.50] that all his life Sir William Elliot was annoyed by passing hairs in urination. They would lodge in the urethra and cause constant irritation. At his death a

stone was taken from the bladder, covered with scurf and hair. Hall [13.51] relates the case of a woman of sixty, from whose bladder, by dilatation of the urethra, was removed a bundle of hairs two inches long, which, Hall says, without a doubt had grown from the vesical walls.
Retention of Foreign Bodies in the Pelvis.—It is a peculiar fact that foreign bodies which once gain entrance to the pelvis may be tolerated in this location for many years. Baxter [13.52] describes a man who suffered an injury from a piece of white board which entered his pelvis, and remained in position for sixteen and a half years; at this time a piece of wood 7 1/2 inches
Rupture of the Male Urethra.—The male urethra is occasionally ruptured in violent coitus. Frank *[351] and the Philosophical Transactions [13.55] are among the older authorities mentioning this accident. In Frank's case there was hemorrhage from the penis to the extent of five pounds. Colles [13.56] mentions a man of thirty-eight, prone to obesity, and who had been married two months, who said that in sexual congress he had hurt himself by pushing his penis against the pubic bone, and added that he had a pain that felt as though something had broken in his organ. The integuments of the penis became livid and swollen and were extremely painful. His urine had to be drawn by a catheter, and by the fifth day his condition was so bad that an incision was made into the tumor, and pus, blood, urine, and air issued. The patient suffered intense rigors, his abdomen became tympanitic, and he died. Postmortem examination revealed the presence of a ruptured urethra.
Watson [13.57] relates an instance of coitus performed en postillon by a man while drunk, with rupture of the urethra and fracture of the corpus spongiosum only. Loughlin mentions a rupture of the corpus spongiosum during coitus. Frank *[351] cites a curious case of hemorrhage from a fall while the penis was erect. It is not unusual to find ruptured urethræ following traumatism, and various explanations are given for it in the standard works on surgery.
Fracture of the Penis.—A peculiar accident to the penis is fracture, which sometimes occurs in coitus. This accident consists in the laceration of the corpora cavernosa, followed by extensive extravasation of blood into the erectile tissue. It has also occurred from injury inflicted accidentally or maliciously, but always happening when the organ was erect. An annoying sequel following this accident is the tendency to curvature in erection, which is sometimes so marked as to interfere with coitus, and even render the patient permanently impotent. *[845]
There is an account [13.58] of a laborer of twenty-seven who, in attempting to micturate with his penis erect, pressed it downward with considerable force and fractured the corpora cavernosa. Veazie [13.59] relates a case of fracture of the corpora cavernosa occurring in coitus. During the act the female suddenly withdrew, and the male, following, violently struck the pubes, with the resultant injury. Recovery ensued. M'Clellan [13.60] speaks of removing the
The Transactions of the South Carolina Medical Association [13.61] contain an account of a negro of sixty who had urethral stricture from gonorrhea and who had been treated for fifteen years by caustics. The penis was seven inches in circumference around the glans, and but little less near the scrotum. The glans was riddled with holes, and numerous fistulæ existed on the inferior surface of the urethra, the meatus being impermeable. So great was the weight and hypertrophy that amputation was necessary. John Hunter speaks of six strictures existing in one urethra at one time; Lallemand of seven; Bolot of eight; Ducamp of five; Boyer thought three could never exist together; Leroy D'Etoilles found 11, and Rokitansky met with four.
Sundry Injuries to the Penis.—Fabricius Hildanus *[334] mentions a curious case of paraphimosis caused by violent coitus with a virgin who had an extremely narrow vagina. Joyce [13.62] relates a history of a stout man who awoke with a vigorous erection, and feeling much irritation, he scratched himself violently. He soon bled copiously, his shirt and underlying sheets and blankets being soaked through. On examination the penis was found swollen, and on drawing back the foreskin a small jet of blood spurted from a small rupture in the frenum. The authors have knowledge of a case in which hemorrhage from the frenum proved fatal. The patient, in a drunken wager, attempted to circumcise himself with a piece of tin, and bled to death before medical aid could be summoned. It sometimes happens that the virile member is amputated by an animal bite. Paullini *[620] and Celliez [13.63] mention amputation of the penis by a dog-bite. Morgan [13.64] describes a boy of thirteen who was feeding a donkey which suddenly made a snap at him, unfortunately catching him by the trousers and including the penis in one of the folds. By the violence of the bite the boy was thrown to the ground, and his entire prepuce was stripped off to the root as if it had been done by a knife. There was little hemorrhage, and the prepuce was found in the trousers, looking exactly like the finger of a glove. Morgan stated that this was the third case of the kind of which he had knowledge. Bookey [13.65] records a case in which an artilleryman was seized by the penis by an infuriated horse, and the two crura were pulled out entire.
Amputation of the penis is not always followed by loss of the sexual power and instinct, but sometimes has the mental effect of temporarily increasing the desire. Haslam [13.66] reports the case of a man who slipped on the greasy deck of a whaler, and falling forward with great violence upon a large knife used to cut blubber, completely severed his penis, beside inflicting a wound in the abdomen through which the intestines protruded. After recovery
Norris [13.67] gives an account of a private who received a gunshot wound of the penis while it was partly erect. The wound was acquired at the second battle of Fredericksburg. The ball entered near the center of the glans penis, and taking a slightly oblique direction, it passed out of the right side of the penis 1 1/2 inches beyond the glans; it then entered the scrotum, and after striking the pelvis near the symphysis, glanced off around the innominate bone, and finally made its exit two inches above the anus. The after-effects of this injury were incontinence of urine, and inability to assume the erect position.
Bookey [13.68] cites the case of six wounds from one bullet with recovery. The bullet entered the sole and emerged from the dorsum of the foot. It then went through the right buttock and came out of the groin, only to penetrate the dorsum of the penis and emerge at the upper part of the glans. Rose [13.69] speaks of a case in which a man had his clothes caught in machinery, drawing in the external genital organs. The testicles were found to be uninjured, but the penis was doubled out of sight and embedded in the scrotum, from whence it was restored to its natural position and the man recovered.
Nélaton [13.70] describes a case of luxation of the penis in a lad of six who fell from a cart. Nélaton found the missing member in the scrotum, where it had been for nine days. He introduced Sir Astley Cooper's instrument for tying deeply-seated arteries through a cutaneous tube, and conducting the hook under the corporus cavernosum, seized this crosswise, and by a to-and-fro movement succeeded in replacing the organ.
Moldenhauer [13.71] describes the case of a farmer of fifty-seven who was injured in a runaway accident, a wheel passing over his body close to the abdomen. The glans penis could not be recognized, since the penis in toto had been torn from its sheath at the corona, and had slipped or been driven into the inguinal region. This author quotes Stromeyer's case, [13.72] which was that of a boy of four and a half years who was kicked by a horse in the external genital region. The sheath was found empty of the penis, which had been driven into the perineum.
Raven [13.73] mentions a case of spontaneous retraction of the penis in a man of twenty-seven. While in bed he felt a sensation of coldness in the penis, and on examination he found the organ (a normal-sized one) rapidly retracting or shrinking. He hastily summoned a physician, who found that
Injuries of the penis and testicles self-inflicted are grouped together and discussed in Chapter XIV.
As a rule, spontaneous gangrene of the penis has its origin in some intense fever. Partridge [13.74] describes a man of forty who had been the victim of typhus fever, and whose penis mortified and dried up, becoming black and like the empty finger of a cast-off glove; in a few days it dropped off. Boyer [13.75] cites a case of edema of the prepuce, noticed on the fifteenth day of the fever, and which was followed by gangrene of the penis. Rostan [13.76] mentions gangrene of the penis from small-pox. Intermittent fever has been cited as a cause. [13.77] Koehler [13.78] reports a fatal instance of gangrene of the penis, caused by a prostatic abscess following gonorrhea. In this case there was thrombosis of the pelvic veins. Hutchinson [13.79] mentions a man who, thirty years before, after six days' exposure on a raft, had lost both legs by gangrene. At the age of sixty-six he was confined to bed by subacute bronchitis, and during this period his whole penis became gangrenous and sloughed off. This is quite unusual, as gangrene is usually associated with fever; it is more than likely that the gangrene of the leg was not connected with that of the penis, but that the latter was a distinct after-result. Possibly the prolonged exposure at the time he lost his legs produced permanent injury to the blood-vessels and nerves of the penis. There is a case on record in which, in a man of thirty-seven, gangrene of the penis followed delirium tremens, and was attributed to alcoholism. [13.80] Quoted by Jacobson, *[445] Troisfontaines records a case of gangrene of the skin and body of the penis in a young man, and without any apparent cause. Schutz [13.81] speaks of regeneration of the penis after gangrenous destruction.
Gangrene of the penis does not necessarily hinder the performance of marital functions. Chance [13.82] mentions a man whose penis sloughed off, leaving only a nipple-like remnant. However, he married four years later, and always lived in harmony with his wife. At the time of his death he was the father of a child, subsequent to whose birth his wife had miscarried, and at the time of report she was daily expecting to be again confined.
Willett [13.83] relates the instance of a horseman of thirty-three who, after
Priapism is sometimes seen as a curious symptom of lesion of the spinal cord. In such cases it is totally unconnected with any voluptuous sensation and is only found accompanied by motor paralysis. It may occur spontaneously immediately after accident involving the cord, and is then probably due to undue excitement of the portion of the cord below the lesion, which is deprived of the regulating influence of the brain. Priapism may also develop spontaneously at a later period, and is then due to central irritation from extravasation into the substance of the cord, or to some reflex cause. It may also occur from simple concussion, as shown by a case reported by Le Gros Clark. Pressure on the cerebellum is supposed to account for cases of priapism observed in executions and suicides by hanging. There is an instance recorded of an Italian "castrate'' who said he provoked sexual pleasure by partially hanging himself. He accidentally ended his life in pursuance of this peculiar habit. The facts were elicited by testimony at the inquest.
There are, however, in literature, records of long continued priapism in which either the cause is due to excessive stimulation of the sexual center or in which the cause is obscure or unknown. There may or may not be accompanying voluptuous feelings. The older records contain instances of continued infantile priapism caused by the constant irritation of ascarides and also records of prolonged priapism associated with intense agony and spasmodic cramps. Zacutus Lusitanus *[831] speaks of a Viceroy of India who had a long attack of stubborn priapism without any voluptuous feeling. Gross refers to prolonged priapism, and remarks that the majority of cases seem to be due to excessive coitus.
Moore [13.84] reports a case in a man of forty who had been married fifteen years, and who suffered spasmodic contractions of the muscles of the penis after an incomplete coitus. This pseudopriapism continued for twenty-three days, during which time he had unsuccessfully resorted to the application of cold, bleeding, and other treatment; but on the twenty-sixth day, after the use of bladders filled with cold water, there was a discharge from the urethra of a glairy mucus, similar in nature to that in seminal debility. There was then complete relaxation of the organ. During all this time the man slept very little, only occasionally dozing. Donne [13.85] describes an athletic laborer of twenty-five who received a wound from a rifle-ball penetrating the cranial parietes immediately in the posterior superior angle of the parietal bone, and a few lines from the lambdoid suture. The ball did not make egress, but passed posteriorly downward. Reaction was established on the third day, but the inflammatory symptoms influenced the genitalia. Priapism began
Salzer [13.87] presents an interesting paper on priapism which was quoted in The Practitioner of London. Salzer describes one patient of forty-six who awoke one morning with a strong erection that could not be reduced by any means. Urine was voided by jerks and with difficulty, and only when the subject was placed in the knee and elbow position. Despite all treatment this condition continued for seven weeks. At this time the patient's spleen was noticed to be enormously enlarged. The man died about a year after the attack, but a necropsy was unfortunately refused. Salzer, in discussing the theories of priapism, mentions eight cases previously reported, and concludes, that such cases are attributable to leukemia. Kremine believes that continued priapism is produced by effusion of blood into the corpora cavernosa, which is impeded on its return. He thinks it corresponds to bleeding at the nose and rectum, which often occurs in perfectly healthy persons. Longuet regards the condition of the blood in leukemia as the cause of such priapism, and considers that the circulation of the blood is retarded in the smaller vessels, while, owing to the great increase in the number of white corpuscles, thrombi are formed. Neidhart and Matthias conclude that the origin of this condition might be sought for in the disturbance of the nerve-centers. After reviewing all these theories, Salzer states that in his case the patient was previously healthy and never had suffered the slightest hemorrhage in any part, and he therefore rejects the theory of extravasation. He is inclined to suppose that the priapism was due to the stimulation of the nervi erigentes, brought about either by anatomic change in the nerves themselves, or by pressure upon them by enlarged lumbar glands, an associate condition of leukemia.
Bruce [13.89] mentions the case of an Irishman of fifty-five who, without apparent cause, was affected with a painful priapism which lasted six weeks, and did not subside even under chloroform. Booth [13.90] mentions a case of priapism in a married seaman of fifty-five, due to local inflammation about the muscles, constricting the bulb of the penis. The affection lasted five weeks, and was extremely painful. There was a similar case of priapism which lasted for three weeks, and was associated with hydrocele in a man of forty-eight. [13.91]
Injuries of the testicle and scrotum may be productive of most serious issue. It is a well-known surgical fact that a major degree of shock accompanies a contusion of this portion of the body. In fact, Chevers *[266] states that the sensitiveness of the testicles is so well known in India, that there are cases on record in which premeditated murder has been effected by Cossiah women, by violently squeezing the testicles of their husbands. He also mentions another case in which, in frustrating an attempt at rape, death was caused in a similar manner. Stalkartt [13.92] describes the case of a young man who, after drinking to excess with his paramour, was either unable, or indifferent in gratifying her sexual desire. The woman became so enraged that
Avulsion of the male external genitalia is not always accompanied by serious consequences, and even in some cases the sexual power is preserved. Knoll [13.93] described a case in 1781, occurring in a peasant of thirty-six who fell from a horse under the wheels of a carriage. He was first caught in the revolving wheels by his apron, which drew him up until his breeches were entangled, and finally his genitals were torn off. Not feeling much pain at the time, he mounted his horse and went to his house. On examination it was found that the injury was accompanied with considerable hemorrhage. The wound extended from the superior part of the pubes almost to the anus; the canal of the urethra was torn away, and the penis up to the neck of the bladder. There was no vestige of either the right scrotum or testicle. The left testicle was hanging by its cord, enveloped in its tunica vaginalis. The cord was swollen and resembled a penis stripped of its integument. The prostate was considerably contused. After two months of suffering the patient recovered, being able to evacuate his urine through a fistulous opening that had formed. In ten weeks cicatrization was perfect. In his "Memoirs of the Campaign of 1811,'' Larrey describes a soldier who, while standing with his legs apart, was struck from behind by a bullet. The margin of the sphincter and, the skin of the perineum, the bulbous portion of the urethra, some of the skin of the scrotum, and the right testicle were destroyed. The spermatic cord was divided close to the skin, and the skin of the penis and prepuce was torn. The soldier was left as dead on the field, but after four months' treatment he recovered.
Madden [13.94] mentions a man of fifty who fell under the feet of a pair of horses, and suffered avulsion of the testicles through the scrotum. The organs were mangled, the spermatic cord was torn and hung over the anus, and the penis was lacerated from the frenum down. The man lost his testicles, but otherwise completely recovered. Brugh [13.95] reports an instance of injury to the genitalia in a boy of eighteen who was caught in a threshing-machine. The skin of the penis and scrotum, and the tissue from the pubes and inguinal region were torn from the body. Cicatrization and recovery were complete. Brigham [13.96] cites an analogous case in a youth of seventeen who was similarly caught in threshing machinery. The skin of the penis and the scrotum was entirely torn away; both sphincters of the anus were lacerated, and the perineum was divested of its skin for a space 2 1/2 inches wide. Recovery ensued, leaving a penis which measured, when flaccid, three inches long and 1 1/2 inches in diameter.
Gibbs [13.98] mentions a case in which the entire scrotum and the perineum, together with an entire testicle and its cord attached, and nearly all the integument of the penis were torn off, yet the patient recovered with preservation of sexual powers. The patient was a negro of twenty-two who, while adjusting a belt, had his coat (closely buttoned) caught in the shafting, and his clothes and external genitals torn off. On examination it was found that the whole scrotum was wrenched off, and also the skin and cellular tissue, from 2 1/2 inches above the spine of the pubes down to the edge of the sphincter ani, including all the breadth of the perineum, together with the left testicle with five inches of its cord attached, and all the integument and cellular covering of the penis except a rim nearly half an inch wide at the extremity and continuous with the mucous membrane of the prepuce. The right testicle was hanging by its denuded cord, and was apparently covered only by the tunica vaginalis as high up as the abdominal ring, where the elastic feeling of the intestines was distinctly perceptible. There was not more than half an ounce of blood lost. The raw surface was dressed, the gap in the perineum brought together, and the patient made complete recovery, with preservation of his sexual powers. Other cases of injuries to the external genital organs (self-inflicted) will be found in the next chapter.
The preservation of the sexual power after injuries of this kind is not uncommon. There is a case reported [13.99] of a man whose testicles were completely torn away, and the perineal urethra so much injured that micturition took place through the wound. After a tedious process the wound healed and the man was discharged, but he returned in ten days with gonorrhea, stating that he had neither lost sexual desire nor power of satisfaction. Robbins [13.100] mentions a man of thirty-eight who, in 1874, had his left testicle removed. In the following year his right testicle became affected and was also removed. The patient stated that since the removal of the second gland he had regular sexual desire and coitus, apparently not differing from that in which he indulged before castration. For a few months previous to the time of report the cord on the left side, which had not been completely extirpated, became extremely painful and was also removed.
Atrophy of the testicle may follow venereal excess, and according to Larrey, deep wounds of the neck may produce the same result, with the loss of the features of virility. Guthrie [13.101] mentions a case of spontaneous absorption of the testicle. According to Larrey, on the return of the French Army
In his description of the diseases of Barbadoes Hendy mentions several peculiar cases under his observation in which the scrotum sloughed, leaving the testicles denuded. Alix and Richter [13.102] mention a singular modification of rheumatic inflammation of the testicle, in which the affection flitted from one testicle to the other, and alternated with rheumatic pains elsewhere.
There is a case of retraction of the testicle reported [13.103] in a young soldier of twenty-one who, when first seen, complained of a swelling in the right groin. He stated that while riding bareback his horse suddenly plunged and threw him on the withers. He at once felt a sickening pain in the groin and became so ill that he had to dismount. On inspection an oval tumor was seen in the groin, tender to the touch and showing no impulse on coughing. The left testicle was in its usual position, but the right was absent. The patient stated positively that both testicles were in situ before the accident. An attempt at reduction was made, but the pain was so severe that manipulation could not be endured. A warm bath and laudanum were ordered, but unfortunately, as the patient at stool gave a sudden bend to the left, his testicle slipped up into the abdomen and was completely lost to palpation. Orchitis threatened, but the symptoms subsided; the patient was kept under observation for some weeks, and then as a tentative measure, discharged to duty. Shortly afterward he returned, saying that he was ill, and that while lifting a sack of corn his testicle came partly down, causing him great pain. At the time of report his left testicle was in position, but the right could not be felt. The scrotum on that side had retracted until it had almost disappeared; the right external ring was very patent, and the finger could be passed up in the inguinal canal; there was no impulse on coughing and no tendency to hernia.
A unique case of ectopia of the testicle in a man of twenty-four is given by Popoff. [13.104] The scrotum was normally developed, and the right testicle in situ. The left half of the scrotum was empty, and at the root of the penis there was a swelling the size of a walnut, covered with normal skin, and containing an oval body about four-fifths the size of the testicle, but softer in constituency. The patient claimed that this swelling had been present since childhood. His sexual power had been normal, but for the past six months he had been impotent. In childhood the patient had a small inguinal hernia, and Popoff thought this caused the displacement of the testicle.
Rupture of the spermatic arteries and veins has caused sudden death. Schleiser [13.106] is accredited with describing an instance in which a healthy man was engaged in a fray in the dark, and, suddenly crying out, fell into convulsions and died in five minutes. On examination the only injury found was the rupture of both spermatic arteries at the internal ring, produced by a violent pull on the scrotum and testicles by one of his antagonists. Shock was evidently a strong factor in this case. Fabricius Hildanus [13.107] gives a case of impotency due to lesions of the spermatic vessels following a burn. There is an old record [13.108] of an aged man who, on marrying, found that he had erections but no ejaculations. He died of ague, and at the autopsy it was found that the verumontanum was hard and of the size of a walnut and that the ejaculatory ducts contained calculi about the size and shape of peas.
Hydrocele is a condition in which there is an abnormal quantity of fluid in the tunica vaginalis. It is generally caused by traumatism, violent muscular efforts, or straining, and is much more frequent in tropic countries than elsewhere. It sometimes attains an enormous size. Leigh *[483] mentions a hydrocele weighing 120 pounds, and there are records of hydroceles weighing 40 [13.109] and 60 pounds. [13.110] Larrey speaks of a sarcocele in the coverings of the testicle which weighed 100 pounds. Mursinna *[577] describes a hydrocele which measured 27 inches in its longest and 17 in its transverse axis.
Tedford [13.111] gives a curious case of separation of the ovary in a woman of twenty-eight. After suffering from invagination of the bowel and inflammation of the ovarian tissue, an ovary was discharged through an opening in the sigmoid flexure, and thence expelled from the anus.
In discussing injuries of the vagina, the first to be mentioned will be a remarkable case reported by Curran. [13.112] The subject was an Irish girl of twenty. While carrying a bundle of clothes that prevented her from seeing objects in front of her, she started to pass over a stile, just opposite to which a goat was lying. The woman wore no underclothing, and in the ascent her body was partially exposed, and, while in this enforced attitude, the goat,
Trompert [13.113] mentions a case of rupture of the vagina by the horn of a bull. There is a case recorded in the Pennsylvania Hospital Reports *[623] of a girl of nineteen who jumped out of a second-story window. On reaching the ground, her foot turned under her as she fell. The high heel of a French boot was driven through the perineum one inch from the median line, midway between the anus and the posterior commissure of the labia majora. The wound extended into the vagina above the external opening, in which the heel, now separated from the boot, projected, and whence it was removed without difficulty. This wound was the only injury sustained by the fall.
Beckett [13.114] records a case of impalement in a woman of forty-five who, while attempting to obtain water from a hogshead, fell with one limb inside the cistern, striking a projecting stave three inches wide and 1/2 inch thick. The external labia were divided, the left crus of the clitoris separated, the nymphæ lacerated, and the vaginal wall penetrated to the extent of five inches; the patient recovered by the fourth week.
Homans [13.115] reports recovery from extensive wounds acquired by a negress who fell from a roof, striking astride an upright barrel. There was a wound of the perineum, and penetration of the posterior wall of the vagina, with complete separation of the soft parts from the symphysis pubis, and extrusion of the bladder.
Howe [13.116] reports a case of impalement with recovery in a girl of fifteen who slid down a hay-stack, striking a hay-hook which penetrated her perineum and passed into her body, emerging two inches below the umbilicus and one inch to the right of the median line.
Injuries of the vagina may be so extensive as to allow protrusion of the intestines, and some horrible cases of this nature are recorded. In The Lancet for 1873 [13.117] there is reported a murder or suicide of this description. The woman was found with a wound in the vagina, through which the intestines, with clean-cut ends, protruded. Over 7 1/2 feet of the intestines had been cut off in three pieces. The cuts were all clean and carefully separated from the mesentery. The woman survived her injuries a whole week, finally
There is a case of death from a ruptured clitoris reported by Gutteridge. [13.119] The woman was kicked while in a stooping position and succumbed to a profuse hemorrhage, estimated to be between three and four pounds, and proceeding from a rupture of the clitoris.
Discharge of Vaginal Parietes.—Longhi [13.120] describes the case of a woman of twenty-seven, an epileptic, with metritis and copious catamenia twice a month. She was immoderately addicted to drink and sexual indulgence, and in February, 1835, her menses ceased. On May 8th she was admitted to the hospital with a severe epileptic convulsion, and until the 18th remained in a febrile condition, with abdominal tenderness, etc. On the 21st, while straining as if to discharge the contents of the rectum, she felt a voluminous body pass through the vagina, and fancied it was the expected fetus. After washing this mass it was found to be a portion of the vaginal parietes and the fleshy body of the neck of the uterus. The woman believed she had miscarried, and still persisted in refusing medicine. Cicatrization was somewhat delayed; immediately on leaving the hospital she returned to her old habits, but the pain and hemorrhage attending copulation was so great that she had finally to desist. The vagina, however, gradually yielding, ceased to interfere with the gratification of her desires. Toward the end of June the menses reappeared and flowed with the greatest regularity. The portions discharged are preserved in the Milan Hospital.
The injuries received during coitus have been classified by Spaeth as follows: Deep tears of the hymen with profuse hemorrhage; tears of the clitoris and of the urethra (in cases of atresia hymenis); vesicovaginal fistula; laceration of the vaginal fornices, posteriorly or laterally; laceration
Crandall [13.126] cites instances in which hemorrhage, immediately after coitus of the marriage-night, was so active as to almost cause death. One of his patients was married three weeks previously, and was rapidly becoming exhausted from a constant flowing which started immediately after her first coitus. Examination showed this to be a case of active intrauterine hemorrhage excited by coitus soon after the menstrual flow had ceased and while the uterus and ovaries were highly congested. In another case the patient commenced flooding while at the dinner table in the Metropolitan Hotel in New York, and from the same cause an almost fatal hemorrhage ensued. Hirst of Philadelphia has remarked that brides have been found on their marital beds completely covered with blood, and that the hemorrhage may have been so profuse as to soak through the bed and fall on the floor. Lacerations of the urethra from urethral coitus in instances of vaginal atresia or imperforate hymen may also excite serious hemorrhage.
Foreign Bodies in the Vagina.—The elasticity of the vagina allows the presence in this passage of the most voluminous foreign bodies. When we
When a foreign body remains in the vagina for a long time and if it is composed of material other than glass, it becomes influenced by the corrosive action of the vaginal secretion. For instance, Cloquet removed a foreign body which was incrusted in the vagina, and found the cork pessary which had formed its nucleus completely rotted. A similar instrument found by Gosselin [13.129] had remained in the vagina thirty-six years, and was incrustated with calcareous salts. Metal is always attacked by the vaginal secretions in the most marked manner. Cloquet mentions that at an autopsy of a woman who had a pewter goblet in her vagina, lead oxid was found in the gangrenous debris.
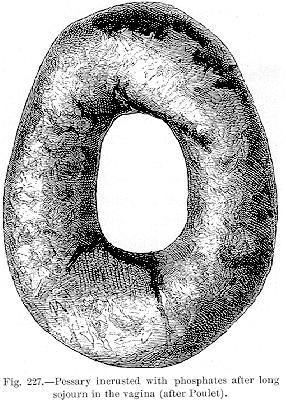
Long Retention of Pessaries, etc.—The length of time during which pessaries may remain in the vagina is sometimes astonishing. The accompanying illustration (Fig. 227) shows the phosphatic deposits and incrustations around a pessary after a long sojourn in the vagina. The specimen is in the Musée Dupoytren. Pinet mentions a pessary that remained in situ for twenty-five years. Gerould of Massilon, Ohio, reports a case in which a pessary had been worn by a German woman of eighty-four for more than fifty years. She had forgotten its existence until reminded of it by irritation some years before death. It was remarkable that when the pessary was removed it was found to have largely retained its original wax covering. Hurxthal [13.130] mentions the
There is an account [13.133] of a young girl addicted to onanism who died from the presence of a pewter cup in her vagina; it had been there fourteen months. Shame had led her to conceal her condition for all the period during which she suffered pain in the hypogastrium, and diarrhea. She had steadily refused examination. Bazzanella of Innsbruck removed a drinking glass from the vagina by means of a pair of small obstetric forceps. The glass had been placed there ten years previously by the woman's husband. Szigethy [13.134] reports the case of a woman of seventy-five who, some thirty years before, introduced into her vagina a ball of string previously dipped in wax. The ball was effectual in relieving a prolapsed uterus, and was worn with so little discomfort that she entirely forgot it until it was forced out of place by a violent effort. The ball was seven inches in circumference, and covered with mucus, but otherwise unchanged. Breisky *[664] is accredited with the report of a case of a woman suffering with dysmenorrhea, in whose vagina was found a cotton reel which had been introduced seven years before. The woman made a good recovery. Pearse [13.135] mentions a woman of thirty-six who had suffered menorrhagia for ten days, and was in a state of great prostration and suffering from strong colicky pains. On examination he found a silk-bobbin about an inch from the entrance, which the patient had introduced fourteen years before. She had already had attacks of peritonitis and hemorrhage, and a urethrovaginal fistula was found. The bobbin itself was black. This patient had been married twice, and had been cared for by physicians, but the existence of a body 3/4 inch long had never been noticed. Poulet quotes two curious cases: [13.136] in one a pregnant woman was examined by a doctor who diagnosticated carcinomatous degeneration of the neck of the uterus. Capuron, who was consulted relative to the case, did not believe that the state of the woman's health warranted the diagnosis, and on further examination the growth was found to have been a sponge which had previously been introduced by the woman into the vagina The other case, reported by Guyon, exemplified another error in diagnosis. The patient was a woman who suffered from continuous vaginal hemorrhage, and had been given extensive treatment without success. Finally, when the woman was in extreme exhaustion, an injection of vinegar-water was ordered, the use of which was followed by the expulsion from the vagina of a live leech of a species very abundant in the country. The hemorrhage immediately ceased and health returned.
There is a record [13.137] of a woman of twenty-eight who was suddenly surprised by some one entering her chamber at the moment she was introducing
Foreign bodies are generally introduced in the uterus either accidentally in vaginal applications, or for the purpose of producing abortion. Zuhmeister *[720] describes a case of a woman who shortly after the first manifestations of pregnancy used a twig of a tree to penetrate the matrix. She thrust it so strongly into the uterus that the wall was perforated, and the twig became planted in the region of the kidneys. Although six inches long and of the volume of a goose feather, this branch remained five months in the pelvis without causing any particular inconvenience, and was finally discharged by the rectum. Brignatelli [13.139] mentions the case of a woman who, in culpable practices, introduced the stalk of a reed into her uterus. She suffered no inconvenience until the next menstrual epoch which was accompanied by violent pains. She presented the appearance of one in the pains of labor. The matrix had augmented in volume, and the orifice of the uterine cervix was closed, but there was hypertrophy as if in the second or third month of pregnancy. After examination a piece of reed three cm. long was extracted from the uterus, its external face being incrusted with hard calcareous material. Meschede of Schwetz, Germany, mentions death from a hair-pin in the uterine cavity.
Crouzit [13.140] was called to see a young girl who had attempted criminal abortion by a darning-needle. When he arrived a fetus of about three months had already been expelled, and had been wounded by the instrument. It was impossible to remove the needle, and the placenta was not expelled for two days. Eleven days afterward the girl commenced to have pains in the inguinal region, and by the thirty-fifth day an elevation was formed, and the pains increased in violence. On the seventy-ninth day a needle six inches
| CHAPTER XIII.
SURGICAL ANOMALIES OF THE GENITOURINARY
SYSTEM. Anomalies and Curiosities of Medicine | ||