| CHAPTER XII.
SURGICAL ANOMALIES OF THE THORAX AND
ABDOMEN. Anomalies and Curiosities of Medicine | ||
12. CHAPTER XII.
SURGICAL ANOMALIES OF THE THORAX AND
ABDOMEN.
Injuries of the lung or bronchus are always serious, but contrary to the general idea, recovery after extensive wound of the lung is quite a common occurrence. Even the older writers report many instances of remarkable recoveries from lung-injuries, despite the primitive and dirty methods of treatment. A review of the literature previous to this century shows the names of Arcæus, Brunner, Collomb, Fabricius Hildanus, Vogel, Rhodius, Petit, Guérin, Köler, Peters, Flebbe, and Stalpart, *[750] as authorities for instances of this nature. In one of the journals *[108] there is a description of a man who was wounded by a broad-sword thrust in the mediastinum. After death it was found that none of the viscera were wounded, and death was attributed to the fact that the in-rush of air counterbalancing the pressure within the lungs left them to their own contractile force, with resultant collapse, obstruction to the circulation, and death. It is said that Vesalius demonstrated this condition on the thorax of a pig.
Gooch *[382] gives an instance of a boy of thirteen who fell from the top of a barn upon the sharp prow of a plough, inflicting an oblique wound from the axilla to below the sternum, slightly above the insertion of the diaphragm. Several ribs were severed, and the left thoracic cavity was wholly exposed to view, showing the lungs, diaphragm, and pericardium all in motion. The lungs soon became gangrenous, and in this horrible state the patient lived twelve days. One of the curious facts noticed by the ancient writers was the amelioration of the symptoms caused by thoracic wounds after hemorrhage from other locations; and naturally, in the treatment of such injuries, this circumstance was used in advocacy of depletion. Monro speaks of a gentleman who was wounded in a duel, and who had all the symptoms of hemothorax; his condition was immediately relieved by the evacuation of a considerable quantity of bloody matter with the urine. Swammerdam records a similar case, and Fabricius ab Aquapendente noticed a case in which the opening in the thorax showed immediate signs of improvement after the patient voided large quantities of bloody urine. Glandorp also calls attention to the foregoing facts. Nicolaus Novocomensis narrates the details of the case of one of his friends, suffering from a penetrating wound of the
There is an extraordinary recovery reported [12.1] in a boy of fifteen who, by falling into the machinery of an elevator, was severely injured about the chest. There were six extensive lacerations, five through the skin about six inches long, and one through the chest about eight inches long. The 3d, 4th, 5th, and 6th ribs were fractured and torn apart, and about an inch of the substance of the 4th rib was lost. Several jagged fragments were removed; a portion of the pleura, two by four inches, had been torn away, exposing the pericardium and the left lung, and showing the former to have been penetrated and the latter torn. The lung collapsed completely, and for three or four months no air seemed to enter it, but respiration gradually returned. The lacerated integument could only be closed approximately by sutures. It is worthy of remark that, although extremely pale, the patient complained of but little pain, and exhibited only slight symptoms of shock. The pleural cavity subsequently filled with a dirty serum, but even this did not interfere with the healing of the wound and the restoration of the lung; the patient recovered without lateral curvature.
Bartholf reports a case of rapid recovery after perforating wound of the lung. The pistol-ball entered the back 1 1/2 inches to the right of the spinous process of the 6th dorsal vertebra, and passed upward and very slightly inward toward the median line. Its track could be followed only 1 1/4 inches. Emphysema appeared fifteen minutes after the reception of the wound, and soon became pronounced throughout the front and side of the neck, a little over the edge of the lower jaw, and on the chest two inches below the sternum and one inch below the clavicle. In four hours respiration became very frequent, short, and gasping, the thoracic walls and the abdomen scarcely moving. The man continued to improve rapidly, the emphysema disappeared on the seventh day, and eighteen days after the reception of the wound he was discharged. There was slight hemorrhage from the wound at the time, but the clot dried and closed the wound, and remained there until it was removed on the morning of his discharge, leaving a small, dry, white cicatrix.
Loss of Lung-tissue.—The old Amsterdam authority, Tulpius, *[842] has recorded a case in which a piece of lung of about three fingers' breadth protruded through a large wound of the lung under the left nipple. This wound received no medical attention for forty-eight hours, when the protruding portion of lung was thought to be dead, and was ligated and cut off; it weighed about three ounces. In about two weeks the wound healed with the lung adherent to it and this condition was found six years later at the necropsy of this individual. Tulpius quoted Celaus and Hippocrates as authorities for the surgical treatment of this case. In 1787 Bell gave an account of a case in which a large portion of the lung protruded and was strangulated by the
Tait [12.3] claims that surgical treatment, as exemplified by Biondi's experiment in removing portions of lung from animals, such as dogs, sheep, cats, etc., is not practical; he adds that his deductions are misleading, as the operation was done on healthy tissue and in deep and narrow-chested animals. Excision of diseased portions of the lung has been practised by Krönlein (three cases), Ruggi of Bologna (two cases), Block, Milton, Weinlechner; one of Krönlein's patients recovered and Milton's survived four months, but the others promptly succumbed after the operation. Tuffier [12.4] is quoted as showing a patient, aged twenty-nine, upon whom, for beginning tuberculosis, he had performed pneumonectomy four years before. At the operation he had removed the diseased area at the apex of the right lung, together with sound tissue for two cm. in every direction. Tuffier stated that the result of his operation had been perfectly successful and the patient had shown no suspicious symptoms since.
Rupture of the Lung Without Fracture.—It is quite possible for the lung to be ruptured by external violence without fracture of the ribs; there are several such cases on record. The mechanism of this rare and fatal form of injury has been very aptly described by Gosselin as due to a sudden pressure exerted on the thoracic wall at the moment of full inspiration, there being a spasm of the glottis or obstruction of the larynx, in consequence of which the lung bursts. An extravasation of air occurs, resulting in the development of emphysema, pneumothorax, etc. Subsequently pleurisy, pneumonia, or even pus in the pleural cavity often result. Hemoptysis is a possible, but not a marked symptom. The mechanism is identical with that of the bursting of an inflated paper bag when struck by the hand. Other observers discard this theory of M. Gosselin and claim that the rupture is due to direct pressure, as in the cases in which the heart is ruptured without fracture of the ribs. The theory of Gosselin would not explain these cardiac ruptures from external violence on the thoracic walls, and, therefore, was rejected by some. Paré, Morgagni, Portal, Hewson Smith, Dupuytren, Laënnec, and others mention this injury. Gosselin reports two cases terminating in recovery. Ashurst reports having seen three cases, all of which terminated fatally before the fifth day; he has collected the histories of 39
Pyle [12.5] reports a case successfully treated, as follows:—
" Lewis W., ten years old, white, born in Maryland, and living now in the District of Columbia, was brought in by the Emergency Hospital ambulance, on the afternoon of November 10th, with a history of having been run over by a hose-cart of the District Fire Department. The boy was in a state of extreme shock, having a weak, almost imperceptible pulse; his respirations were shallow and rapid, and his temperature subnormal. There were no signs of external injury about his thoracic cavity and no fracture of the ribs could be detected, although carefully searched for; there was marked emphysema; the neck and side of the face were enormously swollen with the extravasated air; the tissues of the left arm were greatly infiltrated with air, which enabled us to elicit the familiar crepitus of such infiltration when an attempt at the determination of the radial pulse was made. Consciousness was never lost. There were several injuries to the face and scalp; and there was hemorrhage from the nose and mouth, which was attributed to the fact that the patient had fallen on his face, striking both nose and lip. This was confirmed subsequently by the absence of any evidences of hemoptysis during the whole period of convalescence. The saliva was not even blood-streaked; therefore, it can be said with verity that there was no hemoptysis. Shortly after admission the patient reacted to the stimulating treatment, his pulse became stronger, and all evidences of threatened collapse disappeared. He rested well the first night and complained of no pain, then or subsequently. The improvement was continuous. The temperature remained normal until the evening of the fifth day, when it rose to 102.2°, end again, on the evening of the sixth, to 102.3°. This rise was apparently without significance as the patient at no time seemed disturbed by it. On the eighth day the temperature again reached the normal and has since remained there. The boy is apparently well now, suffers no inconvenience, and has left the hospital, safe from danger and apparently free from any pulmonary embarrassment. He uses well-developed diaphragmatic breathing which is fully sufficient.''
Pollock [12.6] reports the case of a boy of seven, whose lung was ruptured by a four-wheeled cab which ran over him. He was discharged well in thirty-two days. Bouilly [12.7] speaks of recovery in a boy of seventeen, after a rupture of the lung without fracture. There are several other interesting cases of recovery on record.
There are instances of spontaneous rupture of the lung, from severe cough. Hicks [12.8] speaks of a child of ten months suffering with a severe cough
Complete penetration or transfixion of the thoracic cavity is not necessarily fatal, and some marvelous instances of recovery after injuries of this nature, are recorded. Eve [12.10] remarks that General Shields was shot through the body by a discharge of a cannon at Cerro Gordo, and was given up as certain to die. The General himself thought it was grape-shot that traversed his chest. He showed no signs of hemoptysis, and although in great pain, was able to give commands after reception of the wound. In this case, the ball had evidently entered within the right nipple, had passed between the lungs, through the mediastinum, emerging slightly to the right of the spine. Guthrie [12.11] has mentioned a parallel instance of a ball traversing the thoracic cavity, the patient completely recovering after treatment. Girard, Weeds, Meacham, Bacon, Fryer and others [12.12] report cases of perforating gunshot wounds of the chest with recovery.
Sewell [12.13] describes a case of transfixion of the chest in a youth of eighteen. After mowing and while carrying his scythe home, the patient accidentally fell on the blade; the point passed under the right axilla, between the 3d and 4th right ribs, horizontally through the chest, and came out through corresponding ribs of the opposite side, making a small opening. He fell to the ground and lay still until his brother came to his assistance; the latter with great forethought and caution carefully calculated the curvature of the scythe blade, and thus regulating his direction of tension, successfully withdrew the instrument. There was but little hemoptysis and the patient soon recovered. Chelius [12.14] records an instance of penetration of the chest by a carriage shaft, with subsequent recovery. Hoyland [12.15] mentions a man of twenty-five who was discharging bar-iron from the hold of a ship; in a stooping position, preparatory to hoisting a bundle on deck, he was struck by one of the bars which pinned him to the floor of the hold, penetrating the thorax, and going into the wood of the flooring to the extent of three inches, requiring the combined efforts of three men to extract it. The bar had entered posteriorly between the 9th and 10th ribs of the left side, and had traversed the thorax in an upward and outward direction, coming out anteriorly between the 5th and 6th ribs, about an inch below and slightly external to the nipple. There was little constitutional disturbance, and the man was soon discharged cured. Brown [12.16] records a case of impalement in a boy of fourteen. While running to a fire, he struck the point of the shaft of a carriage, which passed through his left chest, below the nipple. There was, strangely, no hemorrhage, and no symptoms of so severe an injury; the boy recovered.
There is deposited in the Museum of the Royal College of Surgeons in
In the same museum, near to this spike, is the portion of a shaft of the carriage which passed through the body of a gentleman who happened to be standing near the vehicle when the horse plunged violently forward, with the result that the off shaft penetrated his body under the left arm, and came out from under the right arm, pinning the unfortunate man to the stable door. Immediately after the accident the patient walked upstairs and got in bed; his recovery progressed uninterruptedly, and his wounds were practically healed at the end of nine weeks; he is reported to have lived eleven years after this terrible accident.
In the Indian Medical Gazette [12.17] there is an account of a private of thirty-five, who was thrown forward and off his horse while endeavoring to mount. He fell on a lance which penetrated his chest and came out through the scapula. The horse ran for about 100 yards, the man hanging on and trying to stop him. After the extraction of the lance the patient recovered. Longmore [12.18] gives an instance of complete transfixion by a lance of the right side of the chest and lung, the patient recovering. Ruddock [12.19] mentions cases of penetrating wounds of both lungs with recovery.
There is a most remarkable instance of recovery after major thoracic wounds recorded by Brokaw. [12.20] In a brawl, a shipping clerk received a thoracic wound extending from the 3d rib to within an inch of the navel, 13 1/2 inches long, completely severing all the muscular and cartilaginous structures, including the cartilages of the ribs from the 4th to the 9th, and wounding the pleura and lung. In addition there was an abdominal wound 6 1/2 inches long, extending from the navel to about two inches above Poupart's ligament, causing almost complete intestinal evisceration. The lung was partially collapsed. The cartilages were ligated with heavy silk, and the hemorrhage checked by ligature and by packing gauze in the inter-chondral spaces. The patient speedily recovered, and was discharged in a little over a month, the only disastrous result of his extraordinary injuries being a small ventral hernia.
There are some peculiar causes of diaphragmatic injuries on record, laughter, prolonged vomiting, excessive eating, etc., being mentioned. On the other hand, in his "Essay on Laughter (du Ris),'' Joubert quotes a case in which involuntary laughter was caused by a wound of the diaphragm; the laughter mentioned in this instance was probably caused by convulsive movements of the diaphragm, due to some unknown irritation of the phrenic nerve. Bremuse [12.21] gives an account of a man who literally split his diaphragm in two by the ingestion of four plates of potato soup, numerous cups of tea and milk, followed by a large dose of sodium bicarbonate to aid digestion. After this meal his stomach swelled to an enormous extent and tore the diaphragm on the right side, causing immediate death.
The diaphragm may be ruptured by external violence (a fall on the chest or abdomen), or by violent squeezing (railroad accidents, etc.), or according to Ashhurst, by spasmodic contraction of the part itself. If the injury is unaccompanied by lesion of the abdominal or thoracic viscera, the prognosis is not so unfavorable as might be supposed. Unless the laceration is extremely small, protrusion of the stomach or some other viscera into the thoracic cavity will almost invariably result, constituting the condition known as internal or diaphragmatic hernia. Paré *[618] relates the case of a Captain who was shot through the fleshy portion of the diaphragm, and though the wound was apparently healed, the patient complained of a colicky pain. Eight months afterward the patient died in a violent paroxysm of this pain. At the postmortem by Guillemeau, a man of great eminence and a pupil of Paré, a part of the colon was found in the thorax, having passed through a wound in the diaphragm. Gooch *[382] saw a similar case, but no history of the injury could be obtained. Bausch [12.22] mentions a case in which the omentum, stomach, and pancreas were found in the thoracic cavity, having protruded through an extensive opening in the diaphragm. Muys, Bonnet, Blancard, Schenck, Sennert, Fantoni, and Godefroy record instances in which, after rupture of the diaphragm, the viscera have been found in the thorax; there are many modern cases on record. Internal hernia through the diaphragm is mentioned by Cooper, Bowles, Fothergill, Monro, Ballonius, Derrecagiax, and Schmidt. Sir Astley Cooper [12.23] mentioned a case of hernia ventriculi from external violence, wherein the diaphragm was lacerated without any fracture
Postempski [12.24] successfully treated a wound of the diaphragm complicated with a wound of the omentum, which protruded between the external opening between the 10th and 11th ribs; he enlarged the wound, forced the ribs apart, ligated and cut off part of the omentum, returned its stump to the abdomen, and finally closed both the wound in the diaphragm and the external wound with sutures. Quoted by Ashhurst, Hunter recorded a case of gunshot wound, in which, after penetrating the stomach, bowels, and diaphragm the ball lodged in the thoracic cavity, causing no difficulty in breathing until shortly before death, and even then the dyspnea was mechanical—from gaseous distention of the intestines.
Peritonitis in the thoracic cavity is a curious condition which may be brought about by a penetrating wound of the diaphragm. In 1872 Sargent communicated to the Boston Society for Medical Improvement an account of a postmortem examination of a woman of thirty-seven, in whom he had observed major injuries twenty years before. At that time, while sliding down some hay from a loft, she was impaled on the handle of a pitchfork which entered the vagina, penetrated 22 inches, and was arrested by an upper left rib, which it fractured; further penetration was possibly prevented by the woman's feet striking the floor. Happily there was no injury to the bladder, uterus, or intestines. The principal symptoms were hemorrhage from the vagina and intense pain near the fractured rib, followed by emphysema. The pitchfork-handle was withdrawn, and was afterward placed in the museum of the Society, the abrupt bloody stain, 22 inches from the rounded end, being plainly shown. During twenty years the woman could never lie on her right side or on her back, and for half of this time she spent most of the night in the sitting position. Her last illness attracted little attention because her life had been one of suffering. After death it was found that the cavity in the left side of the chest was entirely filled with abdominal viscera. The opening in the diaphragm was four inches in diameter, and through it had passed the stomach, transverse colon, a few inches of the descending colon, and a considerable portion of the small intestines. The heart was crowded to the right of the sternum and was perfectly healthy, as was also the right lung. The left lung was compressed to the size of a hand. There were marked signs of peritonitis, and in the absence of sufficient other symptoms, it could be said that this woman had died of peritonitis in the left thoracic cavity.
Extended tolerance of foreign bodies loose in the thoracic cavity has been noticed. Tulpins *[842] mentions a person who had a sponge shut up
Foreign Bodies in the Bronchi.—Walnut kernels, coins, seeds, beans, corks, and even sponges have been removed from the bronchi. In the presence of Sir Morrell Mackenzie, Johnston of Baltimore removed a toy locomotive from the subglottic cavity by tracheotomy and thyreotomy. The child had gone to sleep with the toy in his mouth and had subsequently swallowed it [12.28] Eldredge [12.29] presented a hopeless consumptive, who as a child of five had swallowed an umbrella ferrule while whistling through it, and who expelled it in a fit of coughing twenty-three years after. Eve of Nashville [12.30] mentions a boy who placed a fourpenny nail in a spool to make a whistle, and, by a violent inspiration, drew the nail deep into the left bronchus. It was removed by tracheotomy. Liston removed a large piece of bone from the right bronchus of a woman, and Houston tells of a case in which a molar tooth was lodged in a bronchus causing death on the eleventh day. Warren mentions spontaneous expulsion of a horse-shoe nail from the bronchus of a boy of two and one-half years. From Dublin, in 1844, Houston reports the case of a girl of sixteen who inhaled the wooden peg of a small fiddle and in a fit of coughing three months afterward expelled it from the lungs. In 1849 Solly communicated the case of a man who inhaled a pebble placed on his tongue to relieve thirst. On removal this pebble weighed 144 grains. Watson of Murfreesboro removed a portion of an umbrella rib from a trachea, but as he failed to locate or remove the ferrule, the case terminated fatally. Brigham [12.31] mentions a child of five who was seized with a fit of coughing while she had a small brass nail in her mouth; pulmonary phthisis ensued, and in one year she died. At the postmortem examination the nail was found near the bifurcation of the right bronchus, and, although colored black, was not corroded.
Marcacci [12.32] reported an observation of the removal of a bean from the bronchus of a child of three and a half years. The child swallowed the bean while playing, immediately cried, and became hoarse. No one having noticed the accident, a diagnosis of croup was made and four leeches were applied to the neck. The dyspnea augmented during the night, and there
Lapeyre [12.35] mentions an elderly gentleman who received a sudden slap on the back while smoking a cigarette, causing him to start and take a very deep inspiration. The cigarette was drawn into the right bronchus, where it remained for two months without causing symptoms or revealing its presence. It then set up a circumscribed pneumonia and cardiac dropsy which continued two months longer, at which time, during a violent fit of coughing, the cigarette was expelled enveloped in a waxy, mucus-like matter. Louis relates the case of a man who carried a louis-d'or in his lung for six and a half years.
There is a case on record [12.36] of a man who received a gunshot wound, the ball entering behind the left clavicle and passing downward and across to the right clavicle. Sometime afterward this patient expectorated two pieces of
Cardiac Injuries.—For ages it has been the common opinion relative to injuries of the heart that they are necessarily fatal and that, as a rule, death immediately follows their reception. Notwithstanding this current belief a careful examination of the literature of medicine presents an astounding number of cases in which the heart has been positively wounded, and the patients have lived days, months, and even recovered; postmortem examination, by revealing the presence of cicatrices in the heart, confirming the original diagnosis. This question is one of great interest as, in recent years, there has been constant agitation of the possibility of surgical procedures in cardiac as well as cerebral injuries. Del Vecchio [12.38] has reported a series of experiments on dogs with the conclusion that in case of wounds in human beings suture of the heart is a possible operation. In this connection he proposes the following operative procedure: Two longitudinal incisions to be made from the lower border of the 3d rib to the upper border of the 7th rib, one running along the inner margin of the sternum, the other about ten mm. inside the nipple-line. These incisions are joined by a horizontal cut made in the fourth intercostal space. The 4th, 5th, and 6th ribs and cartilages are divided and the outer cutaneous flaps turned up; pushing aside the pleura with the finger, expose the pericardium and incise it longitudinally; suture the heart-wound by interrupted sutures. Del Vecchio adds that Fischer has collected records of 376 cases of wounds of the heart with a mortality two to three minutes after the injury of 20 per cent. Death may occur from a few seconds to nine months after the accident. Keen and Da Costa [12.39] quote Del Vecchio, and, in comment on his observations, remark that death in cases of wound of the heart is due to pressure of effused blood in the pericardial sac, and, because this pressure is itself a cheek to further hemorrhage, there seems, as far as hemorrhage is concerned, to be rather a question whether operative interference may not be itself more harmful than beneficial. It might be added that the shock to the cardiac action might be sufficient to check it, and at present we would have no sure means of starting pulsation if once stopped. In heart-injuries, paracentesis, followed, if necessary, by incision of the pericardium, is advised by some surgeons.
Realizing the fatality of injuries of the heart, in consequence of which almost any chance by operation should be quickly seized by surgeons rather than trust the lives of patients to the infinitesimal chance of recovery, it would seem that the profession should carefully consider and discuss the feasibility of any procedure in this direction, no matter how hypothetic.
Hall [12.40] states that his experience in the study of cardiac wounds, chiefly
Instances of Survival after Cardiac Injuries.—We briefly cite the principal interesting instances of cardiac injuries in which death has been delayed for some time, or from which the patient ultimately recovered.
Paré *[618] relates the case of a soldier who received a blow from a halberd, penetrating the left ventricle, and who walked to the surgeon's tent to have his wound dressed and then to his own tent 260 yards away. Diemerbroeck [12.41] mentions two instances of long survival after cardiac injuries, in one of which the patient ran 60 paces after receiving the wound, had complete composure of mind, and survived nine days. There is an instance [12.42] in which a man ran 400 paces after penetration of the left ventricle, and lived for five hours. Morand *[575] gives an instance of survival for five days after wound of the right ventricle. Saucerotte [12.43] speaks of survival for three days after injury to the heart.
Babington [12.44] speaks of a case of heart-injury, caused by transfixion by a bayonet, in which the patient survived nine hours. Other older cases are as
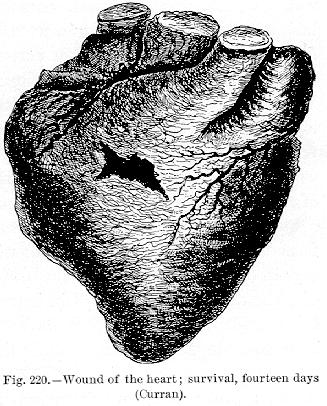
The Duc de Berri, heir to the French throne, who was assassinated in 1826, lived several hours with one of his ventricles opened. His surgeon, Dupuytren, was reprimanded for keeping the wound open with a probe introduced every two hours, but this procedure has its advocates at the present day. Randall [12.58] mentions a gunshot wound of the right ventricle which did not cause death until the sixty-seventh day. Grant [12.59] describes a wound in which a ball from a revolver entered a little to the right of the sternum, between the cartilages of the 5th and 6th ribs, and then entered the right ventricle about an inch from the apex. It emerged from the lower part, passed through the diaphragm, the cardiac end of the stomach, and lodged in the left kidney. The patient remained in a state of collapse fifteen hours after being shot, and with little or no nourishment lived twenty-six days. At the postmortem examination the wounds in the organs were found to be healed, but the cicatrices were quite evident. Bowling [12.60] gives a case of gunshot wound of the shoulder in which death resulted eleven weeks after, the bullet being found in the left venticle of the heart. Thompson [12.61] has reported a bayonet wound of the heart, after the reception of which the patient lived four days. The bayonet entered the ventricle about 1 1/2 inches from the left apex, traversing the left wall obliquely, and making exit close to the septum ventriculorum. Roberts [12.62] mentions a man who ran 60 yards and lived one hour after being shot through both lungs and the right auricle. Curran [12.63] mentions the case of a soldier who, in 1809, was wounded by a bullet which entered his body to the left of the sternum, between the 2d and 3d ribs. He was insensible a half hour, and was carried aboard a fighting ship crowded with sailors. There was little hemorrhage from his wound, and he survived fourteen days. At the postmortem examination some interesting facts were revealed. It was found that the right ventricle was transversely opened for about an inch, the ball having penetrated its anterior surface, near the origin of the pulmonary artery (Fig. 220). The ball was found loose in the pericardium, where it had fallen during the necropsy. There was a circular lacerated opening in the tricuspid valve, and the ball must have been in the right auricle during the
Hamilton [12.69] gives an instance of a shoemaker sixty-three years old who, while carrying a bundle, fell with rupture of the heart and lived several minutes. On postmortem examination an opening in the heart was found large enough to admit a blowpipe. Noble [12.70] speaks of duration of life for five and a half days after rupture of the heart; and there are instances on record in which life has been prolonged for thirteen hours [12.71] and for fifty-three hours [12.72] after a similar injury. Glazebrook [12.73] reports the case of a colored man of thirty, of powerful physique, who was admitted
to the Freedmen's Hospital, Washington, D. C., at 12.30 A.M., on February 5, 1895. Upon examination by the surgeons, an incised wound was discovered one inch above the left nipple, 3 1/4 inches to the left of the median line, the incision being 2 1/4 inches in length and its direction parallel with the 3d rib. The man's general condition was fairly good, and the wound was examined. It was impossible to trace its depth further than the 3d rib, although probing was resorted to; it was therefore considered a simple wound, and dressed accordingly. Twelve hours later symptoms of internal hemorrhage were noticed, and at 8 A. M., February 6th, the man died after surviving his injury thirty-two hours. A necropsy was held three hours after death, and an oblique incision 3/4 inch in
Fourteen instances of gunshot wounds of the heart have been collected from U. S. Army reports, [12.76] in all of which death followed very promptly, except in one instance in which the patient survived fifty hours. In another case the patient lived twenty-six hours after reception of the injury, the conical pistol-ball passing through the anterior margin of the right lobe of the lung into the pericardium, through the right auricle, and again entered the right pleural cavity, passing through the posterior margin of the lower lobe of the right lung; at the autopsy it was found in the right pleural cavity. The left lung and cavity were perfectly normal. The right lung was engorged and somewhat compressed by the blood in the pleural cavity. The pericardium was much distended and contained from six to eight ounces of partially coagulated blood. There was a fibrinous clot in the left ventricle.
Nonfatal Cardiac Injuries.—Wounds of the heart are not necessarily fatal. Of 401 cases of cardiac injury collected by Fischer [12.77] there were as many as 50 recoveries, the diagnosis being confirmed in 33 instances by an autopsy in which there were found distinct signs of the cardiac injury. By a peculiar arrangement of the fibers of the heart, a wound transverse to one layer of fibers is in the direction of another layer, and to a certain extent, therefore, valvular in function; it is probably from this fact that punctured wounds of the heart are often attended with little or no bleeding.
There is a recent case [12.82] of a boy of fourteen, who was wounded in the heart by a pen-knife stab. The boy was discharged cured from the Middlesex Hospital, but three months after the reception of the injury he was taken ill and died. A postmortem examination showed that the right ventricle had been penetrated in a slanting direction; the cause of death was apoplexy, produced by the weakening and thinning of the heart's walls, the effect of the wound. Tillaux [12.83] reports the case of a man of sixty-five, the victim of general paralysis, who passed into his chest a blade 16 cm. long and 2 mm. broad. The wound of puncture was 5 cm. below the nipple and 2 cm. to the outside. The left side of the chest was emphysematous and ecchymosed. The heart-sounds were regular, and the elevation of the skin by the blade coincided with the ventricular systole. The blade was removed on the following day, and the patient gradually improved. Some thirteen months after he had expectoration of blood and pus and soon died. At the necropsy it was seen that the wound had involved both lungs; the posterior wall of the ventricle and the inferior lobe of the right lung were traversed from before backward, and from left to right, but the ventricular cavity was not penetrated. Strange to say, the blade had passed between the vertebral column and the esophagus, and to the right of the aorta, but had wounded neither of these organs.
O'Connor *[490] mentions a graduate of a British University who, with suicidal intent, transfixed his heart with a darning-needle. It was extracted by a pair of watchmaker's pliers. In five days the symptoms had all abated, and the would-be suicide was well enough to start for the Continent. Mühlig [12.84] was consulted by a mason who, ten years before, had received a blow from a stiletto near the left side of the sternum. The cicatrix was plainly visible, but the man said he had been able to perform his daily labors, although at the present time suffering from intense dyspnea and anasarca. A loud bellows-sound
Stelzner [12.85] mentions a young student who attempted suicide by thrusting a darning-needle into his heart. He complained of pain and dyspnea; in twenty-four hours his symptoms increased to such an extent that operation was deemed advisable on account of collapse. The 5th rib was resected and the pleural cavity opened. When the pericardial sac was incised, a teaspoonful of turbid fluid oozed out, and the needle was felt in an oblique position in the right ventricle. By pressure of a finger passed under the heart, the eye of the needle was pressed through the anterior wall and fixed on the operator's finger-nail. An attempt to remove by the forceps failed, as the violent movements of the heart drew the needle back into the cavity. About this stage of the operation an unfortunate accident happened—the iodoform tampon, which protected the exposed pleural cavity, was drawn into this cavity during a deep inspiration, and could not be found. Notwithstanding subsequent pneumothorax and extensive pleuritic effusion, the patient made a good recovery at the end of the fourth week and at the time of report it was still uncertain whether the needle remained in the heart or had wandered into the mediastinum. During the discussion which followed the report of this case, Hahn showed a portion of a knitting-needle which had been removed from the heart of a girl during life. The extraction was very slow in order to allow of coagulation along the course of the wound in the heart, and to guard against hemorrhage into the pericardial sac, which is so often the cause of death in punctured wounds of this organ. Hahn remarked that the pulse, which before the removal had been very rapid, sank to 90.
Marks [12.86] reports the case of a stab-wound penetrating the left 9th intercostal space, the diaphragm, pleura, pericardium, and apex of the heart. It was necessary to enlarge the wound, and, under an anesthetic, after removing one and one-half inches of the 9th and 10th ribs, the wound was thoroughly packed with iodoform gauze and in twenty-one days the patient recovered. Lavender [12.87] mentions an incised wound of the heart penetrating the right ventricle, from which the patient recovered. Purple [12.88] gives, an account of a recovery from a wound penetrating both ventricles. The diagnosis was confirmed by a necropsy nine years thereafter. Stoll [12.89] records a nonfatal injury to the heart.
Mastin [12.90] reports the case of a man of thirty-two who was shot by a 38-caliber
Mellichamp [12.91] speaks of a gunshot wound of the heart with recovery, and Ford [12.92] records an instance in which a wound of the heart by a buckshot was followed by recovery. O'Connor reports a case under his observation in which a pistol-ball passed through three of the four cavities of the heart and lodged in the root of the right lung. The patient, a boy of fifteen, died of the effects of cardiac disease three years and two months later. Bell mentions a case in which, six years after the receipt of a gunshot wound of the chest, a ball was found in the right ventricle. Christison [12.93] speaks of an instance in which a bullet was found in the heart of a soldier in Bermuda, with no apparent signs of an opening to account for its entrance. There is a case on record [12.94] of a boy of fourteen who was shot in the right shoulder, the bullet entering through the right upper border of the trapezius, two inches from the acromion process. Those who examined him supposed the ball was lodged near the sternal end of the clavicle, four or five inches from where it entered. In about six weeks the boy was at his labors. Five years later he was attacked with severe pneumonia and then first noticed tumultuous action of the heart which continued to increase after his recovery. Afterward the pulsation could be heard ten or 12 feet away. He died of another attack of pneumonia fifteen years later and the heart was found to be two or three times its natural size, soft and flabby, and, on opening the right ventricle, a bullet was discovered embedded in its walls. There was no scar of entrance discernible, though the pericardium was adherent. Biffi of Milan [12.95] describes the case of a lunatic who died in consequence of gangrene of the tongue from a bite in a paroxysm of mania. At the neoropsy a needle, six cm. in length, was found transfixing the heart, with which the relatives of the deceased said he had stabbed himself twenty-two months prior to his death. There is a collection of cases [12.96] in which bullets have been lodged in the heart from twenty to thirty years.
Balch [12.97] reports a case in which a leaden bullet remained twenty years in the walls of the heart. Hamilton [12.98] mentions an instance of gunshot wound
Garangeot mentions an aged Jesuit of seventy-two, who had in the substance of his heart a bone 4 1/2 inches long and possibly an inch thick. This case is probably one of ossification of the cardiac muscle; in the same connection Battolini says that the heart of Pope Urban VII. contained a bone shaped like the Arab T.
Among the older writers we frequently read of hairs, worms, and snakes being found in the cavities of the heart. The Ephemerides, Zacutus Lusitanus, Paré, Swinger, Riverius, and Senac are among the authorities who mention this circumstance. The deception was possibly due to the presence of loose and shaggy membrane attached to the endocardial lining of the heart, or in some cases to echinococci or trichine. A strange case of foreign body in the heart was reported [12.100] some time since in England. The patient had swallowed a thorn of the Prunus spinosa (Linn.), which had penetrated the esophagus and the pericardium and entered the heart. A postmortem examination one year afterward confirmed this, as a contracted cicatrix was plainly visible on the posterior surface of the heart about an inch above the apex, through which the thorn had penetrated the right ventricle and lodged in the tricuspid valve. The supposition was that the thorn had been swallowed while eating radishes. Buck [12.101] mentions a case of hydatid cysts in the wall of the left ventricle, with rupture of the cysts and sudden death.
It is surprising the extent of injury to the pericardium Nature will tolerate. In his "Comment on the Aphorisms of Hippocrates,'' Cardanus says that he witnessed the excision of a portion of the pericardium with the subsequent cure of the patient. According to Galen, Marulus, the son of Mimographus, recovered after a similar operation. Galen also adds, that upon one occasion he removed a portion of carious sternum and found the pericardium in a putrid state, leaving a portion of the heart naked. It is said that in the presence of Leucatel and several theologians, François Botta opened the body of a man who died after an extended illness and found the pericardium putrefied and a great portion of the heart destroyed, but the remaining portion still slightly palpitating. In this connection Young [12.102] mentions a patient of sixty-five who in January, 1860, injured his right thumb and lost the last joint by swelling and necrosis. Chloroform was administered to excise a portion of the necrosed bone and death ensued. Postmortem examination revealed gangrene of the heart and a remarkable tendency to gangrene elsewhere (omentum, small intestines, skin, etc.). Recently, Dalton [12.103] records a remarkable case of stab-wound of the pericardium with division of the intercostal
Rupture of the heart from contusion of the chest is not always instantly fatal. According to Ashhurst, Gamgee has collected 28 cases of rupture of this viscus, including one observed by himself. In nine of these cases there was no fracture, and either no bruise of the parietes or a very slight one. The pericardium was intact in at least half of the cases, and in 22 in which the precise seat of lesion was noticed the right ventricle was ruptured in eight, the left in three, the left auricle in seven, the right in four. The longest period during which any patient survived the injury was fourteen hours.
Among the older writers who note this traumatic injury are Fine, who mentions concussion rupturing the right ventricle, and Ludwig, who reports a similar accident. Johnson [12.105] mentions rupture of the left ventricle in a paroxysm of epilepsy. There is another species of rupture of the heart which is not traumatic, in which the rupture occurs spontaneously, the predisposing cause being fatty degeneration, dilatation, or some other pathologic process in the cardiac substance. It is quite possible that the older instances of what was known as "broken-heart,'' which is still a by-word, were really cases in which violent emotion had produced rupture of a degenerated cardiac wall. Wright [12.106] gives a case of spontaneous rupture of the heart in which death did not occur for forty-eight hours. Barth has collected 24 cases of spontaneous rupture of the heart, and in every instance the seat of lesion was in the left ventricle. It was noticed that in some of these cases the rupture did not take place all at once, but by repeated minor lacerations, death not ensuing in some instances for from two to eleven days after the first manifestation of serious symptoms. A more recent analysis is given by Meyer of cases reported since 1870: [12.107] Meyer collects 25 cases of rupture of the left ventricle seven of the right ventricle, and four of the right auricle. Within the last year Collings [12.108] has reported a case of idiopathic rupture of the heart in a man of fifty-three, who had always lived a temperate life, and whose only trouble had been dyspepsia and a weak heart. There was no history of rheumatism or rheumatic fever. The man's father had died suddenly of heart disease. After feeling out of sorts for a time, the man experienced severe pain in the precordium and felt too ill to leave his bed. He gradually became worse and
Stokes [12.109] gives the case of a man who was severely crushed between the arms of a water-wheel of great size and the embankment on which the axle of the wheel was supported; a peculiar factor of the injury being that his heart was displaced from left to right. At the time of report, after recovery from the injury, the patient exhibited remarkable tolerance of great doses of digitalis. When not taking digitalis, his pulse was 100 to 120, regular, and never intermittent.
Hypertrophy of the Heart.—The heart of a man of ordinary size weighs nine ounces, and that of a woman eight; in cases of hypertrophy, these weights may be doubled, although weights above 25 ounces are rare. According to Osler, Beverly Robinson describes a heart weighing 53 ounces, and Dulles has reported one weighing 48 ounces. Among other modern records are the following: Fifty and one-half ounces, [12.110] 57 ounces, [12.111] and one weighing four pounds and six ounces. [12.112] The Ephemerides [12.113] contains an incredible account of a heart that weighed 14 pounds. Favell [12.114] describes a heart that only weighed 3 1/2 ounces.
Wounds of the aorta are almost invariably fatal, although cases are recorded by Pelletan, Heil, Legouest, and others, in which patients survived such wounds for from two months to several years. Green [12.115] mentions a case of stab-wound in the suprasternal fossa. The patient died one month after of another cause, and at the postmortem examination the aorta was shown to have been opened; the wound in its walls was covered with a spheric, indurated coagulum. No attempt at union had been made.
Zillner [12.116] observed a penetrating wound of the aorta after which the patient
Sundry Cases.—Sandifort *[709] mentions a curious case of coalescence of the esophagus and aorta, with ulceration and consequent rupture of the aorta, the hemorrhage proceeding from the stomach at the moment of rupture.
Heath [12.119] had a case of injury to the external iliac artery from external violence, with subsequent obliteration of the vessel. When the patient was discharged no pulse could be found in the leg.
Dismukes [12.120] reports a case in which the patient had received 13 wounds, completely severing the subclavian artery, and, without any medical or surgical aid, survived the injury two hours.
Illustrative of the degree of hemorrhage which may follow an injury so slight as that of falling on a needle we cite an instance, reported by a French authority, [12.121] of a child who picked up a needle, and, while running with it to its mother, stumbled and fell, the needle penetrating the 4th intercostal space, the broadened end of it remaining outside of the wound. The mother seized the needle between her teeth and withdrew it, but the child died, before
Rupture of the esophagus is attributable to many causes. Dryden [12.122] mentions vomiting as a cause, and Guersant [12.123] reports the case of a little girl of seven, who, during an attack of fever, ruptured her esophagus by vomiting. In 1837 Heyfelder reported the case of a drunkard, who, in a convulsion, ruptured his esophagus and died. Williams [12.124] mentions a case in which not only the gullet, but also the diaphragm, was ruptured in vomiting. In this country, Bailey [12.125] and Fitz [12.126] have recorded cases of rupture of the esophagus. Brewer *[587] relates a parallel instance of rupture from vomiting. All the foregoing cases were linear ruptures, but there is a unique case given by Boerhaave in 1724, in which the rent was transverse. Ziemssen and Mackenzie *[499] have both translated from the Latin the report of this case which is briefly as follows: The patient, Baron de Wassenaer, was fifty years of age, and, with the exception that he had a sense of fulness after taking moderate meals, he was in perfect health. To relieve this disagreeable feeling he was in the habit of taking a copious draught of an infusion of "blessed thistle'' and ipecacuanha. One day, about 10.30 in the evening, when he had taken no supper, but had eaten a rather hearty dinner, he was bothered by a peculiar sensation in his stomach, and to relieve this he swallowed about three tumbler-fuls of his usual infusion, but to no avail. He then tried to excite vomiting by tickling the fauces, when, in retching, he suddenly felt a violent pain; he diagnosed his own case by saying that it was "the bursting of something near the pit of the stomach.'' He became prostrated and died in eighteen and one-half hours; at the necropsy it was seen that without any previously existing signs of disease the esophagus had been completely rent across in a transverse direction.
Schmidtmuller [12.127] mentions separation of the esophagus from the stomach; and Flint [12.128] reports the history of a boy of seven who died after being treated for worms and cerebral symptoms. After death the contents of the stomach were found in the abdominal cavity, and the esophagus was completely separated from the stomach. Flint believed the separation was postmortem, and was possibly due to the softening of the stomach by the action of the gastric acids. In this connection may be mentioned the case reported by Hanford [12.129] of a man of twenty-three who had an attack of hematemesis and melanema two years before death. A postmortem was made five hours after death, and there was so much destruction of the stomach by a process resembling digestion that only the pyloric and cardiac orifices were visible. Hanford suggests that this was an instance of antemortem digestion of the stomach which physiologists claim is impossible.
Clarke [12.135] reports the case of a Hindoo of twenty-two, under treatment for ague, who, without pain or vomiting, suddenly fell into collapse and died twenty-three hours later. He also mentions a case of rupture of the stomach of a woman of uncertain history, who was supposed to have died of cholera. The examination of the bodies of both cases showed true rupture of the stomach and not mere perforation. In both cases, at the time of rupture, the stomach was empty, and the gastric juice had digested off the capsules of the spleens, thus allowing the escape of blood into the abdominal cavities. The seats of rupture were on the anterior walls. In the first case the coats of the stomach were atrophied and thin. In the second the coats were healthy and not even softened. There was absence of softening, erosion, or rupture on the posterior walls.
As illustrative of the amount of paralytic distention that is possible, Bamberger mentions a case in which 70 pounds of fluid filled the stomach.
Voluntary Vomiting.—It is an interesting fact that some persons exhibit the power of contracting the stomach at will and expeling its contents without nausea. Montégre [12.136] mentions a distinguished member of the Faculty of Paris, who, by his own volition and without nausea or any violent efforts, could vomit the contents of his stomach. In his translation of "Spallanzani's Experiments on Digestion'' Sennebier reports a similar instance in Geneva, in which the vomiting was brought about by swallowing air.
In discussing wounds and other injuries of the stomach no chapter would be complete without a description of the celebrated case of Alexis St. Martin, whose accident has been the means of contributing so much to the knowledge of the physiology of digestion. This man was a French Canadian of good constitution, robust and healthy, and was employed as a voyageur by the American Fur Company. On June 16, 1822, when about eighteen years of age, he was accidentally wounded by a discharge from a musket. The contents of the weapon, consisting of powder and duck-shot, entered his left side from a distance of not more than a yard off. The charge was directed obliquely forward and inward, literally blowing off the integument and muscles for a space about the size of a man's hand, carrying away the anterior half of the 6th rib, fracturing the 5th rib, lacerating the lower portion of the lowest lobe of the left lung, and perforating the diaphragm and the stomach. The whole mass of the discharge together with fragments of clothing were driven into the muscles and cavity of the chest. When first seen
Spizharny [12.137] relates a remarkable case of gastric fistula in the loin, and collects 61 cases of gastric fistula, none of which opened in the loin. The patient was a girl of eighteen, who had previously had perityphlitis, followed by abscesses about the navel and lumbar region. Two fistulæ were found in the right loin, and were laid open into one canal, which, after partial resection of the 12th rib, was dilated and traced inward and upward, and found to be in connection with the stomach. Food was frequently found on the dressings, but with the careful use of tampons a cure was effected.
In the olden times wounds of the stomach were not always fatal. The celebrated anatomist, Fallopius, successfully treated two cases in which the stomach was penetrated so that food passed through the wound. Jacobus Orthaeus tells us that in the city of Fuldana there was a soldier who received a wound of the stomach, through which food passed immediately after being
Archer [12.138] tells of a man who was stabbed by a negro, the knife entering the cartilages of the 4th rib on the right side, and penetrating the stomach to the extent of two inches at a point about two inches below the xiphoid cartilage. The stomachal contents, consisting of bacon, cabbage, and cider, were evacuated. Shortly after the reception of the injury, an old soldier sewed up the wound with an awl, needle, and wax-thread; Archer did not see the patient until forty-eight hours afterward, at which time he cleansed and dressed the wound. After a somewhat protracted illness the patient recovered, notwithstanding the extent of injury and the primitive mode of treatment.
Travers [12.139] mentions the case of a woman of fifty-three who, with suicidal intent, divided her abdominal parietes below the navel with a razor, wounding the stomach in two places. Through the wound protruded the greater part of the larger curvature of the stomach; the arch of the colon and the entire greater omentum were both strangulated. A small portion of the coats of the stomach, including the wound, was nipped up, a silk ligature tied about it, and the entrails replaced. Two months afterward the patient had quite recovered, though the ligature of the stomach had not been seen in the stool. Clements [12.140] mentions a robust German of twenty-two who was stabbed in the abdomen with a dirk, producing an incised wound of the stomach. The patient recovered and was returned to duty the following month.
There are many cases on record in which injury of the stomach has been due to some mistake or accident in the juggling process of knife-swallowing or sword-swallowing. The records of injuries of this nature extend back many hundred years, and even in the earlier days the delicate operation of gastrotomy, sometimes with a successful issue, was performed upon persons who had swallowed knives. Gross mentions that in 1502 Florian Mathias of Bradenberg removed a knife nine inches long from the stomach of a man of thirty-six, followed by a successful recovery. Glandorp, *[380] from whom, possibly, Gross derived his information, relates this memorable case as being under the direction of Florianus Matthaesius of Bradenburg. The patient, a native of Prague, had swallowed a knife eight or nine inches long, which lay pointing at the superior portion of the stomach. After it had been lodged in this position for seven weeks and two days gastrotomy was performed, and the knife extracted; the patient recovered. In 1613 Crollius reports the case of a Bohemian peasant who had concealed a knife in his mouth, thinking no one would suspect he possessed the weapon; while he was excited it slipped into the stomach, from whence it subsequently penetrated through to the skin; the man recovered. There is another old case of a man at Prague who swallowed
It is said that in 1691, while playing tricks with a knife 6 1/2 inches long, a country lad of Saxony swallowed it, point first. He came under the care of Weserern, physician to the Elector of Brandenburgh, who successfully extracted it, two years and seven months afterward, from the pit of the lad's stomach. The horn haft of the knife was considerably digested. In 1720 Hubner [12.141] of Rastembourg operated on a woman who had swallowed an open knife. After the incision it was found that the knife had almost pierced the stomach and had excited a slight suppuration. After the operation recovery was very prompt.
Bell [12.142] of Davenport, Iowa, performed gastrotomy on a man, who, while attempting a feat of legerdemain, allowed a bar of lead, 10 1/8 inches long, 1 1/2 inches wide, and 9 1/2 ounces in weight, to slip into his stomach. The bar was removed and the patient recovered. Gussenbauer [12.143] gives an account of a juggler who turned his head to bow an acknowledgment of applause while swallowing a sword; he thus brought his upper incisors against the sword, which broke off and slipped into his stomach. To relieve suffocation the sword was pushed further down. Gastrotomy was performed, and the piece of sword 11 inches long was extracted; as there was perforation of the stomach before the operation, the patient died of peritonitis.
An hour after ingestion, Bernays of St. Louis successfully removed a knife 9 1/2 inches long. By means of an army-bullet forceps the knife was extracted easily through an incision 5/8 inch long in the walls of the stomach. Gross [12.144] speaks of a man of thirty who was in the habit of giving exhibitions of sword-swallowing in public houses, and who injured his esophagus to such an extent as to cause abscess and death. In the Journal of the American Medical Association, March 1, 1896, there is an extensive list of gastrotomies performed for the removal of knives and other foreign bodies, from the seventeenth century to the present time.
The physiologic explanation of sword-swallowing is quite interesting. We know that when we introduce the finger, a spoon, brush, etc., into the throat of a patient, we cause extremely disagreeable symptoms. There is nausea, gagging, and considerable hindrance with the function of respiration.
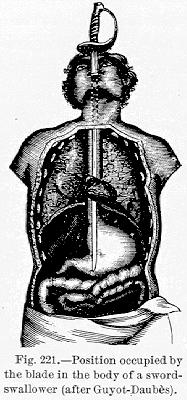
permitting the blade to traverse the greater diameter of the stomach. According to Guyot-Daubès, *[394] these organs, in a straight line, extend a distance of from 55 to 62 cm., and consequently the performer is enabled to swallow an instrument of this length. The length is divided as follows:—
| Mouth and pharynx, | 10 to 12 cm. |
| Esophagus, | 25 to 28 cm. |
| Distended stomach, | 20 to 22 cm. |
| — | |
| 55 to 62 cm. |
These acrobats with the sword have rendered important service to medicine. It was through the good offices of a sword-swallower that the Scotch physician, Stevens, was enabled to make his experiments on digestion. He caused this assistant to swallow small metallic tubes pierced with holes. They were filled, according to Reaumur's method, with pieces of meat. After a certain length of time he would have the acrobat disgorge the tubes, and in this way he observed to what degree the process of digestion had taken place. It was also probably the sword-swallower who showed the physicians to what extent the pharynx could be habituated to contact, and from this resulted the invention of the tube of Faucher, the esophageal sound, ravage of the stomach, and illumination of this organ by electric light. Some of these individuals also have the faculty of swallowing several pebbles, as large even as hen's eggs, and of disgorging them one by one by simple contractions of the stomach.
According to Bonet, there was a man by the name of Pichard who swallowed a razor and two knives in the presence of King Charles II. of England, the King himself placing the articles into the man's mouth. In 1810 Babbington and Curry *[302] are accredited with citing the history of an American sailor in Guy's Hospital, London, who frequently swallowed penknives for the amusement of his audiences. At first he swallowed four, and three days later passed them by the anus; on another occasion he swallowed 14 of different sizes with the same result. Finally he attempted to gorge himself with 17 penknives, but this performance was followed by horrible pains and alarming abdominal symptoms. His excrement was black from iron. After death the cadaver was opened and 14 corroded knives were found in the stomach, some of the handles being partly digested; two were found in the pelvis and one in the abdominal cavity. Paré *[618] recalls the instance of a shepherd who suffered distressing symptoms after gulping a knife six inches long. Afterward the knife was abstracted from his groin. Fabricius Hildanus *[334] cites a somewhat similar case.
Early in the century there was a man known as the "Yankee knife-swallower,'' whose name was John Cummings, an American sailor, who had performed his feats in nearly all the ports of the world. One of his chief performances was swallowing a billiard ball. Poland [12.146] mentions a man (possibly Cummings) who, in 1807, was admitted to Guy's Hospital with dyspeptic symptoms which he attributed to knife-swallowing. His story was discredited at first; but after his death, in March, 1809, there were 30 or 40 fragments of knives found in his stomach. One of the back-springs on a knife had transfixed the colon and rectum. In the Edinburgh Philosophical
Drake [12.148] reports a curious instance of polyphagia. The person described was a man of twenty-seven who pursued the vocation of a "sword-swallower.'' He had swallowed a gold watch and chain with a seal and key attached; at another time he swallowed 34 bullets and voided them by the anus. At Poughkeepsie, N. Y., in August, 1819, in one day and night he swallowed 19 pocket-knives and 41 copper cents. This man had commenced when a lad of fifteen by swallowing marbles, and soon afterward a small penknife. After his death his esophagus was found normal, but his stomach was so distended as to reach almost to the spine of the ilium, and knives were found in the stomach weighing one pound or more. In his exhibitions he allowed his spectators to hear the click of the knives and feel them as low down as the anterior superior spine of the ilium.
The present chief of the dangerous "profession'' of sword-swallowing is Chevalier Cliquot, a French Canadian by birth, whose major trick is to swallow a real bayonet sword, weighted with a cross-bar and two 18-pound dumbbells. He can swallow without difficulty a 22-inch cavalry sword; formerly, in New York, he gave exhibitions of swallowing fourteen 19-inch bayonet swords at once. A negro, by the name of Jones, exhibiting not long since in Philadelphia, gave hourly exhibitions of his ability to swallow with impunity pieces of broken glass and china.
Foreign Bodies in the Alimentary Canal.—In the discussion of the foreign bodies that have been taken into the stomach and intestinal tract possibly the most interesting cases, although the least authentic, are those relating to living animals, such as fish, insects, or reptiles. It is particularly among the older writers that we find accounts of this nature. In the Ephemerides we read of a man who vomited a serpent that had crept into his mouth, and of another person who ejected a beetle that had gained entrance in a similar manner. From the same authority we find instances of the vomiting of live fish, mice, toads, and also of the passage by the anus of live snails and snakes. Frogs vomited are mentioned by Bartholinus, Dolaeus, Hellwigius, Lentilus, Salmuth, and others. *[708] à Vege mentions a man who swallowed a young chicken whole. Paullini speaks of a person who, after great pain, vomited a mouse which he had swallowed. Borellus, Bartholinus, Thoner, and Viridet, are among the older authorities mentioning persons who swallowed toads. Hippocrates speaks of asphyxia from a serpent which had crawled into the mouth.
Borellus states that he knew a case of a person who vomited a salamander. Plater *[535] reports the swallowing of eels and snails. Rhodius mentions persons who have eaten scorpions and spiders with impunity. Planchon [12.149]
There is an abundance of cases in which leeches have been accidentally swallowed. Pliny, Aetius, Dioscorides, Scribonius-Largus, Celsus, Oribasius, Paulus Aegineta, and others, describe such cases. Bartholinus speaks of a Neapolitan prince who, while hunting, quenched his thirst in a brook, putting his mouth in the running water. In this way he swallowed a leech, which subsequently caused annoying hemorrhage from the mouth. Timaeus mentions a child of five who swallowed several leeches, and who died of abdominal pains, hemorrhage, and convulsions. Rhodius, Riverius, and Zwinger make similar observations. According to Baron Larrey the French soldiers in Napoleon's Egyptian campaign occasionally swallowed leeches. Grandchamp and Duval [12.153] have commented on curious observations of leeches in the digestive tract. Dumas and Marques also speak of the swallowing of leeches. Colter [12.154] reports a case in which beetles were vomited. Wright [12.155] remarks on Banon's case of fresh-water shrimps passed from the human intestine. Dalton, Dickman, [12.156] and others, have discussed the possibility of a slug living in the stomach of man. Pichells [12.157] speaks of a case in which beetles were expelled from the stomach; and Pigault [12.158] gives an account of a living lizard expelled by vomiting. Fontaine, Gaspard, Vetillart, Ribert, MacAlister, [12.159] and Waters [12.160] record cases in which living caterpillars have been swallowed.
Sundry Cases.—The variety of foreign bodies that have been swallowed either accidentally or for exhibitional or suicidal purposes is enormous. Nearly every imaginable article from the minutest to the most incredible size has been reported. To begin to epitomize the literature on this subject would in itself consume a volume, and only a few instances can be given here, chosen in such a way as to show the variety, the effects, and the possibilities of their passage through the intestinal canal.
Chopart [12.161] says that in 1774 the belly of a ravenous galley-slave was opened, and in the stomach were found 52 foreign bodies, including a barrel-hoop 19 inches long, nails, pieces of pipe, spoons, buckles, seeds, glass, and a knife. In the intestines of a person Agnew [12.162] found a pair of suspenders, a mass of straw, and three roller-bandages, an inch in width and diameter. Velpeau [12.163] mentions
Among the insane a favorite trait seems to be swallowing nails. In the Philosophical Transactions [12.167] is an account of the contents of the stomach of an idiot who died at thirty-three. In this organ were found nine cart-wheel nails, six screws, two pairs of compasses, a key, an iron pin, a ring, a brass pommel weighing nine ounces, and many other articles. The celebrated Dr. Lettsom, in 1802, spoke of an idiot who swallowed four pounds of old nails and a pair of compasses. A lunatic in England [12.168] swallowed ten ounces of screws and bits of crockery, all of which were passed by the anus. Boardman [12.169] gives an account of a child affected with hernia who swallowed a nail 2 1/2 inches long. In a few days the nail was felt in the hernia, but in due time it was passed by the rectum. Blower [12.170] reports an account of a nail passing safely through the alimentary canal of a baby. Armstrong [12.171] mentions an insane hair-dresser of twenty-three, in whose stomach after death were found 30 or more spoon handles, 30 nails, and other minor articles.
Closmadenc *[363] reported a remarkable case which was extensively quoted. [12.172] The patient was an hysteric young girl, an inmate of a convent, to whom he was called to relieve a supposed fit of epilepsy. He found her half-asphyxiated, and believed that she had swallowed a foreign body. He was told that under the influence of exaggerated religious scruples this girl inflicted penance upon herself by swallowing earth and holy medals. At the first dose of the emetic, the patient made a strong effort to vomit, whereupon a cross seven cm. long appeared between her teeth. This was taken out of her mouth, and with it an enormous rosary 220 cm. long, and having seven medals attached to it. Hunt [12.173] recites a case occurring in a pointer dog, which swallowed its collar and chain, only imperfectly masticating the collar. The chain and collar were immediately missed and search made for them. For several days the dog was ill and refused food. Finally the gamekeeper saw the end of the chain hanging from the dog's anus, and taking hold of it, he drew out a yard of chain with links one inch long, with a
Fear of robbery has often led to the swallowing of money or jewelry. Vaillant, the celebrated doctor and antiquarian, after a captivity of four months in Algiers, was pursued by Tunis pirates, and swallowed 15 medals of gold; shortly after arriving at Lyons he passed them all at stool. Fournier and Duret [12.174] published the history of a galley slave at Brest in whose stomach were found 52 pieces of money, their combined weight being one pound, 10 1/4 ounces. On receiving a sentence of three years' imprisonment, an Englishman, [12.175] to prevent them being taken from him, swallowed seven half-crowns. He suffered no bad effects, and the coins not appearing the affair was forgotten. While at stool some twenty months afterward, having taken a purgative for intense abdominal pain, the seven coins fell clattering into the chamber. Hévin mentions the case of a man who, on being captured by Barbary pirates, swallowed all the money he had on his person. It is said that a certain Italian swallowed 100 louis d'ors at a time.
It occasionally happens that false teeth are accidentally swallowed, and even passed through the intestinal tract. Easton [12.176] mentions a young man who accidentally swallowed some artificial teeth the previous night, and, to further their passage through the bowel, he took a dose of castor oil. When seen he was suffering with pain in the stomach, and was advised to eat much heavy food and avoid aperients. The following day after several free movements he felt a sharp pain in the lower part of his back. A large enema was given and the teeth and plate came away. The teeth were cleansed and put back in his mouth, and the patient walked out. Nine years later the same accident again happened to the man but in spite of treatment nothing was seen of the teeth for a month afterward, when a body appeared in the rectum which proved to be a gold plate with the teeth in it. In The Lancet of December 10, 1881, there is an account of a vulcanite tooth-plate which was swallowed and passed forty-two hours later. Billroth [12.177] mentions an instance of gastrotomy for the removal of swallowed artificial teeth, with recovery; and another case in which a successful esophagotomy was performed. Gardiner [12.178] mentions a woman of thirty-three who swallowed two false teeth while supping soup. A sharp angle of the broken plate had caught in a fold of the cardiac end of the stomach and had caused violent hematemesis. Death occurred seventeen hours after the first urgent symptoms.
In the Museum of the Royal College of Surgeons in London there is an intestinal concretion weighing 470 grains, which was passed by a woman of seventy who had suffered from constipation for many years. Sixteen years
Berwick [12.179] mentions a child of eight months who was playing with a detached organ-handle, and put it in its mouth. Seeing this the mother attempted to secure the handle, but it was pushed into the esophagus. A physician was called, but nothing was done, and the patient seemed to suffer little inconvenience. Three days later the handle was expelled from the anus. Teakle [12.180] reports the successful passage through the alimentary canal of the handle of a music-box. Hashimoto, Surgeon-General of the Imperial Japanese Army, tells of a woman of forty-nine who was in the habit of inducing vomiting by irritating her fauces and pharynx with a Japanese toothbrush— a wooden instrument six or seven inches long with bristles at one end. In May, 1872, she accidentally swallowed this brush. Many minor symptoms developed, and in eleven months there appeared in the epigastric region a fluctuating swelling, which finally burst, and from it extended the end of the brush. After vainly attempting to extract the brush the attending physician contented himself with cutting off the projecting portion. The opening subsequently healed; and not until thirteen years later did the pain and swelling return. On admission to the hospital in October, 1888, two fistulous openings were seen in the epigastric region, and the foreign body was located by probing. Finally, on November 19, 1888, the patient was anesthetized, one of the openings enlarged, and the brush extracted. Five weeks later the openings had all healed and the patient was restored to health.
Garcia [12.181] reports an interesting instance of foreign body in a man between forty-five and fifty. This man was afflicted with a syphilitic affection of the mouth, and he constructed a swab ten inches long with which to cleanse his fauces. While making the application alone one day, a spasmodic movement caused him to relinquish his grasp on the handle, and the swab disappeared. He was almost suffocated, and a physician was summoned; but before his arrival the swab had descended into the esophagus. Two weeks later, gastroperitoneal symptoms presented, and as the stick was located, gastrotomy was proposed; the patient, however, would not consent to an operation. On the twenty-sixth day an abscess formed on the left side below the nipple, and from it was discharged a large quantity of pus and blood. Four days after this, believing himself to be better, the man began to redress the wound, and from it he saw the end of a stick protruding. A physician was called, and by traction the stick was withdrawn from between the 3d and 4th ribs;
Occasionally an enormous mass of hair has been removed from the stomach. A girl of twenty [12.182] with a large abdominal swelling was admitted to a hospital. Her illness began five years previously, with frequent attacks of vomiting, and on three occasions it was noticed that she became quite bald. Abdominal section was performed, the stomach opened, and from it was removed a mass of hair which weighed five pounds and three ounces. A good recovery ensued. In the Museum of St. George's Hospital, London, *[619] are masses of hair and string taken from the stomach and duodenum of a girl of ten. It is said that from the age of three the patient had been in the habit of eating these articles. There is a record in the last century of a boy of sixteen who ate all the hair he could find; after death his stomach and intestines were almost completely lined with hairy masses. In the Journal of the American Medical Association, March 1, 1896, there is a report of a case of hair-swallowing.
Foreign Bodies in the Intestines.—White [12.183] relates the history of a case in which a silver spoon was swallowed and successfully excised from the intestinal canal. Houston [12.184] mentions a maniac who swallowed a rusty iron spoon 11 inches long. Fatal peritonitis ensued and the spoon was found impacted in the last acute turn of the duodenum. In 1895, in London, *[619] there was exhibited a specimen, including the end of the ileum with the adjacent end of the colon, showing a dessertspoon which was impacted in the latter. The spoon was seven inches long, and its bowl measured 1 1/2 inches across. There was much ulceration of the mucous membrane. This spoon had been swallowed by a lunatic of twenty-two, who had made two previous ineffectual attempts at suicide. Mason [12.185] describes the case of a man of sixty-five who, after death by strangulated hernia, was opened, and two inches from the ileocecal valve was found an earthen egg-cup which he had swallowed. Mason also relates the instance of a man who swallowed metal balls 2 1/2 inches in diameter; and the case of a Frenchman who, to prevent the enemy from finding them, swallowed a box containing despatches from Napoleon. He was kept prisoner until the despatches were passed from his bowels. Denby [12.186] discovered a large egg-cup in the ileum of a man. Fillion [12.187] mentions an instance of recovery following the perforation of the jejunum by a piece of horn which had been swallowed. Madden [12.188] tells of a person, dying of intestinal obstruction, in whose intestines were found several ounces of crude mercury and a plum-stone. The mercury had evidently been taken for purgative effect. Rodenbaugh [12.189] mentions a most interesting case of beans sprouting while in the bowel. Harrison [12.190] relates a curious case in which the swallowed
In cases of appendicitis foreign bodies have been found lodged in or about the vermiform appendix so often that it is quite a common lay idea that appendicitis is invariably the result of the lodgment of some foreign body accidentally swallowed. In recent years the literature of this subject proves that a great variety of foreign bodies may be present. A few of the interesting cases will be cited in the following lines:—
In the New England Medical Journal, 1843, is an account of a vermiform appendix which was taken from the body of a man of eighty-eight who had died of pneumothorax. During life there were no symptoms of disease of the appendix, and after death no adhesions were found, but this organ was remarkably long, and in it were found 122 robin-shot. The old gentleman had been excessively fond of birds all his life, and was accustomed to bolt the meat of small birds without properly chewing it; to this fact was attributed the presence of these shot in the appendix. A somewhat similar case [12.191] was that of a man who died in the Hôtel-Dieu in 1833. The ileum of this man contained 92 shot and 120 plum stones. Buckler [12.192] reports a case of appendicitis in a child of twelve, in which a common-sized bird-shot was found in the appendix. Packard [12.193] presented a case of appendicitis in which two pieces of rusty and crooked wire, one 2 1/2 and the other 1 1/2 inches long, were found in the omentum, having escaped from the appendix. Howe [12.194] describes a case in which a double oat, with a hard envelope, was found in the vermiform appendix of a boy of four years and one month of age. Prescott [12.195] reports a case of what he calls fatal colic from the lodgment of a chocolate-nut in the appendix; and Noyes [12.196] relates an instance of death in a man of thirty-one attributed to the presence of a raisin-seed in the vermiform appendix. Needles, pins, peanuts, fruit-stones, peas, grape-seeds, and many similar objects have been found in both normal and suppurative vermiform appendices.
Intestinal Injuries.—The degree of injury that the intestinal tract may sustain, and after recovery perform its functions as usual, is most extraordinary; and even when the injury is of such an extent as to be mortal, the persistence of life is remarkable. It is a well known fact that in bull-fights, after mortal injuries of the abdomen and bowels, horses are seen to struggle on almost until the sport is finished. Fontaine [12.197] reports a case of a Welsh quarryman who was run over by a heavy four-horse vehicle. The stump of a glass bottle was crushed into the intestinal cavity, and the bowels protruded and were bruised by the wheels of the wagon. The grit was so firmly ground into the bowel that it was impossible to remove it; yet the man made a complete recovery.
Tardieu [12.199] relates the case of a chemist who removed a large part of the mesentery with a knife, and yet recovered. Delmas of Montpellier reports the history of a wagoner with complete rupture of the intestines and rupture of the diaphragm, and who yet finished his journey, not dying until eighteen hours after.
Successful Intestinal Resection.—In 1755 Nedham [12.200] of Norfolk reported the case of a boy of thirteen who was run over and eviscerated. It was found necessary to remove 57 inches of the protruding bowel, but the boy made a subsequent recovery. Koebererle [12.201] of Strasburg performed an operation on a woman of twenty-two for the relief of intestinal obstruction. On account of numerous strictures it was found necessary to remove over two yards of the small intestine; the patient recovered without pain or trouble of any kind. In his dissertation on "Ruptures'' Arnaud remarks that he cut away more than seven feet of gangrenous bowel, his patient surviving. Beehe [12.202] reports recovery after the removal of 48 inches of intestine. The case was one of strangulation of an umbilical hernia.
Sloughing of the Intestine Following Intussusception.—Lobstein *[488] mentions a peasant woman of about thirty who was suddenly seized with an attack of intussusception of the bowel, and was apparently in a moribund condition when she had a copious stool, in which she evacuated three feet of bowel with the mesentery attached. The woman recovered, but died five months later from a second attack of intussusception, the ileum rupturing and peritonitis ensuing. There is a record in this country [12.203] of a woman of forty-five who discharged 44 inches of intestine, and who survived for forty-two days. The autopsy showed the sigmoid flexure gone, and from the caput ceci to the termination the colon only measured 14 inches. Vater [12.204] gives a history of a penetrating abdominal wound in which a portion of the colon hung from the wound during fourteen years, forming an artificial anus.
Among others mentioning considerable sloughing of intestine following intussusception, and usually with complete subsequent recovery, are Bare, [12.205] 13 inches of the ileum; Blackton, [12.206] nine inches; Bower, [12.207] 14 inches; Dawson, [12.208] 29 inches; Sheldon, [12.209] 4 1/2 feet; Stanley, [12.210] three feet; Tremaine, [12.211] 17 inches; and Grossoli, [12.212] 40 cm.
Operations upon the gastrointestinal tract have been so improved in the modern era of antisepsis that at the present day they are quite common. There are so many successful cases on record that the whole subject deserves mention here.
Gastrostomy is an operation for establishing a fistulous opening in the stomach through the anterior wall. Many operations have been devised, but the results of this maneuver in malignant disease have not thus far been very satisfactory. It is quite possible that, being an operation of a serious nature, it is never performed early enough, the patient being fatally weakened by inanition. Gross and Zesas [12.221] have collected, respectively, 207 and 162 cases with surprisingly different rates of mortality: that of Gross being only 29.47 per cent., while that of Zesas was for cicatricial stenoses 60 per cent., and for malignant cases 84 per cent. It is possible that in Zesas's statistics the subjects were so far advanced that death would have resulted in a short time without operation. Gastrotomy we have already spoken of.
Pyloroplasty is an operation devised by Heineke and Mikulicz, and is designed to remove the mechanic obstruction in cicatricial stenoses of the pylorus, at the same time creating a new pylorus.
Gastroenterostomy and pylorectomy are operations devised for the relief of malignant disease of the pylorus, the diseased portions being removed and the parts resected.
Gastrectomy or extirpation of the stomach is considered by most surgeons entirely unjustifiable, as there is seldom hope of cure or prospect of amelioration. La Tribune Médicale for January 16, 1895, [12.222] gives an abstract of Langenbuch's contribution upon total extirpation of the stomach. Three patients were treated, of whom two died. In the first case, on opening the abdominal cavity the stomach was found very much contracted, presenting extensive carcinomatous infiltration on its posterior surface. After division of the epiploön section was made at the pylorus and at the cardiac extremities; the portions removed represented seven-eighths of the stomach. The pylorus was stitched to the remains of the cardiac orifice, making a cavity about the size of a hen's egg. In this case a cure was accomplished in three weeks. The second case was that of a man in whom almost the entire stomach
Enterostomy, or the formation of a fecal fistula above the ileocecal valve, was performed for the first time by Nélaton in 1840, but the mortality since 1840 has been so great that in most cases it is deemed inadmissible.
Colostomy, an operation designed to make a fistulous opening in any portion of the rectum, was first practiced by Littre. In early times the mortality of inguinal colostomy was about five per cent., but has been gradually reduced until König reports 20 cases with only one death from peritonitis, and Cripps 26 cases with only one death. [12.223] This will always retain its place in operative surgery as a palliative and life-saving operation for carcinomatous stenosis of the lower part of the colon, and in cases of carcinoma of the rectum in which operation is not feasible.
Intestinal anastomosis, whereby two portions of a severed or resected bowel can be intimately joined, excluding from fecal circulation the portion of bowel which has become obstructed, was originally suggested by Maisonneuve, and was studied experimentally by von Hacken. Billroth resorted to it, and Senn modified it by substituting decalcified bone-plates for sutures. [12.224] Since that time, Abbe, Matas, Davis, Brokaw, Robinson, Stamm, Baracz, and Dawburn, have modified the material of the plates used, substituting catgut rings, untanned leather, cartilage, raw turnips, potatoes, etc. Recently Murphy of Chicago has invented a button, which has been extensively used all over the world, in place of sutures and rings, as a means of anastomosis. Hardly any subject has had more discussion in recent literature than the merits of this ingenious contrivance.
Foreign Bodies in the Rectum.—Probably the most celebrated case of foreign body introduced into the rectum is the classic one mentioned by Hévin. [12.225] Some students introduced the frozen tail of a pig in the anus of a French prostitute. The bristles were cut short, and having prepared the passage with oil, they introduced the tail with great force into the rectum, allowing a portion to protrude. Great pain and violent symptoms followed; there was distressing vomiting, obstinate constipation, and fever. Despite the efforts to withdraw the tail, the arrangement of the bristles which allowed entrance, prevented removal. On the sixth day, in great agony, the woman applied to Marchettis, who ingeniously adopted the simple procedure of taking a long hollow reed, and preparing one of its extremities so that it could be introduced into the rectum, he was enabled to pass the reed entirely around the tail and to withdraw both. Relief was prompt, and the removal of the
Tuffet *[302] is quoted as mentioning a farmer of forty-six who, in masturbation, introduced a barley-head into his urethra. It was found necessary to cut the foreign body out of the side of the glans. A year later he put in his anus a cylindric snuff-box of large size, and this had to be removed by surgical methods. Finally, a drinking goblet was used, but this resulted in death, after much suffering and lay treatment. In his memoirs of the old Academy of Surgery in Paris, Morand speaks of a monk who, to cure a violent colic, introduced into his fundament a bottle of l'eau de la reine de Hongrie, with a small opening in its mouth, by which the contents, drop by drop, could enter the intestine. He found he could not remove the bottle, and violent inflammation ensued. It was at last necessary to secure a boy with a small hand to extract the bottle. There is a record of a case [12.226] in which a tin cup or tumbler was pushed up the rectum and then passed into the colon where it caused gangrene and death. It was found to measure 3 1/2 by 3 1/2 by two inches. There is a French case [12.227] in which a preserve-pot three inches in diameter was introduced into the rectum, and had to be broken and extracted piece by piece.
Cloquet [12.228] had a patient who put into his rectum a beer glass and a preserving pot. Montanari removed from the rectum of a man a mortar pestle 30 cm. long, and Poulet *[641] mentions a pederast who accidentally killed himself by introducing a similar instrument, 55 cm. long, which perforated his intestine. Studsgaard mentions that in the pathologic collection at Copenhagen there is a long, smooth stone, 17 cm. long, weighing 900 gm., which a peasant had introduced into his rectum to relieve prolapsus. The stone was extracted in 1756 by a surgeon named Frantz Dyhr. Jeffreys [12.229] speaks of a person who, to stop diarrhea, introduced into his rectum a piece of wood measuring seven inches.
There is a remarkable case recorded [12.230] of a stick in the anus of a man of sixty, the superior extremity in the right hypochondrium, the inferior in the concavity of the sacrum. The stick measured 32 cm. in length; the man recovered. It is impossible to comprehend this extent of straightening of the intestine without great twisting of the mesocolon. Tompsett [12.231] mentions that he was called to see a workman of sixty-five, suffering from extreme rectal hemorrhage. He found the man very feeble, without pulse, pale, and livid. By digital examination he found a hard body in the rectum, which he was sure was not feces. This body he removed with a polyp-forceps, and found it to be a cylindric candle-box, which measured six inches in circumference, 2 1/2 in length, and 1 1/2 in diameter. The removal was followed by a veritable flood of fecal material, and the man recovered. Lane [12.232] reports
Hunter [12.233] mentions a native Indian, a resident of Coorla, who had introduced a bullock's horn high up into his abdomen, which neither he nor his friends could extract. He was chloroformed and placed in the lithotomy position, his buttocks brought to the edge of the bed, and after dilatation of the sphincter, by traction with the fingers and tooth-forceps, the horn was extracted. It measured 11 inches long. The young imbecile had picked it up on the road, where it had been rendered extremely rough by exposure, and this caused the difficulty in extraction.
In Nelson's Northern Lancet, 1852, *[582] there is the record of a case of a man at stool, who slipped on a cow's horn, which entered the rectum and lodged beyond the sphincter. It was only removed with great difficulty.
A convict at Brest [12.234] put up his rectum a box of tools. Symptoms of vomiting, meteorism, etc., began, and became more violent until the seventh day, when he died. After death, there was found in the transverse colon, a cylindric or conic box, made of sheet iron, covered with skin to protect the rectum and, doubtless, to aid expulsion. It was six inches long and five inches broad and weighed 22 ounces. It contained a piece of gunbarrel four inches long, a mother-screw steel, a screw-driver, a saw of steel for cutting wood four inches long, another saw for cutting metal, a boring syringe, a prismatic file, a half-franc piece and four one-franc pieces tied together with thread, a piece of thread, and a piece of tallow, the latter presumably for greasing the instruments. On investigation it was found that these conic cases were of common use, and were always thrust up the rectum base first. In excitement this prisoner had pushed the conic end up first, thus rendering expulsion almost impossible. Ogle [12.235] gives an interesting case of foreign body in the rectum of a boy of seventeen. The boy was supposed to be suffering with an abdominal tumor about the size of a pigeon's egg under the right cartilages; it had been noticed four months before. On admission to the hospital the lad was suffering with pain and jaundice; sixteen days later he passed a stick ten inches long, which he reluctantly confessed that he had introduced into the anus. During all his treatment he was conscious of the nature of his trouble, but he suffered rather than confess. Studsgaard [12.236] mentions a man of thirty-five who, for the purpose of stopping diarrhea, introduced into his rectum a preserve-bottle nearly seven inches long with the open end uppermost. The next morning he had violent pain in the abdomen, and the bottle could be felt through the abdominal wall. It was necessary to perform abdominal section through the linea alba, divide the sigmoid flexure, and thus remove the bottle. The intestine was sutured and the patient recovered. The bottle measured 17 cm. long, five cm. in diameter at its lower end, and three cm. at its upper end.
Complete transfixion of the abdomen does not always have a fatal issue. In fact, two older writers, Wisemann and Muys, testify that it is quite possible for a person to be transfixed without having any portion of the intestines or viscera wounded. In some nations in olden times, the extremest degree of punishment was transfixion by a stake. In his voyages and travels, [12.240] in describing the death of the King of Demaa at the hands of his page, Mendez Pinto says that instead of being reserved for torture, as were his successors Ravaillac, and Gerard, the slayer of William the Silent, the assassin was impaled alive with a long stake which was thrust in at his fundament and came out at the nape of his neck. There is a record [12.241] of a man of twenty-five, a soldier in the Chinese war of 1860, who, in falling from his horse, was accidentally transfixed by a bayonet. The steel entered his back two inches to the left of the last dorsal vertebra, and reappeared two inches to the left and below the umbilicus; as there was no symptom of visceral wound there were apparently no injuries except perforation of the parietes and the peritoneum. The man recovered promptly.
Ross [12.242] reports a case of transfixion in a young male aborigine, a native of New South Wales, who had received a spear-wound in the epigastrium during a quarrel; extraction was impossible because of the sharp-pointed barbs; the spear was, therefore, sawed off, and was removed posteriorly by means of a small incision. The edges of the wound were cleansed, stitched, and a compress and bandage applied. During the night the patient escaped and joined his comrades in the camp, and on the second day was suffering with radiating pains and distention. The following day it was found that the stitches and plaster had been removed, and the anterior wound was gaping and contained an ichorous discharge. The patient was bathing the wound with a decoction of the leaves of the red-gum tree. Notwithstanding that the spear measured seven inches, and the interference of treatment, the abdominal wound closed on the sixth day, and recovery was uninterrupted. Gilkrist [12.243] mentions an instance in which a ramrod was fired into a soldier's abdomen, its extremity lodging in the spinal column, without causing the slightest evidence of wounds of the intestines or viscera. A minute postmortem
Humphreys [12.244] says that a boy of eleven, while "playing soldier'' with another boy, accidentally fell on a rick-stake. The stake was slightly curved at its upper part, being 43 inches long and three inches in circumference, and sharp-pointed at its extremity. As much as 17 1/2 inches entered the body of the lad. The stake entered just in front of the right spermatic cord, passed beneath Poupart's ligament into the cavity of the abdomen, traversed the whole cavity across to the left side; it then entered the thorax by perforating the diaphragm, displaced the heart by pushing it to the right of the sternum, and pierced the left lung. It then passed anteriorly under the muscles and integument in the axillary space, along the upper third of the humerus, which was extended beyond the head, the external skin not being ruptured. The stick remained in situ for four hours before attempts at extraction were made. On account of the displacement of the heart it was decided not to give chloroform. The boy was held down by four men, and Humphreys and his assistant made all the traction in their power. After removal not more than a teaspoonful of blood followed. The heart still remained displaced, and a lump of intestine about the size of an orange protruded from the wound and was replaced. The boy made a slow and uninterrupted recovery, and in six weeks was able to sit up. The testicle sloughed, but five months later, when the boy was examined, he was free from pain and able to walk. There was a slight enlargement of the abdomen and a cicatrix of the wound in the right groin. The right testicle was absent, and the apex of the heart was displaced about an inch.
Woodbury [12.245] reports the case of a girl of fourteen, who fell seven or eight feet directly upon an erect stake in a cart; the tuberosity was first struck, and then the stake passed into the anus, up the rectum for two inches, thence through the rectal wall, and through the body in an obliquely upward direction. Striking the ribs near the left nipple it fractured three, and made its exit. The stake was three inches in circumference, and 27 inches of its length passed into the body, six or seven inches emerging from the chest. This girl recovered so rapidly that she was able to attend school six weeks afterward. In a case reported by Bailey [12.246] a middle-aged woman, while sliding down a hay-stack, struck directly upon a pitchfork handle which entered the vagina; the whole weight of the woman was successfully maintained by the cellular tissue of the uterovaginal culdesac.
Minot [12.247] speaks of the passage of one prong of a pitchfork through the body of a man of twenty-one, from the perineum to the umbilicus; the man recovered.
Hamilton [12.248] reports a case of laceration of the perineum with penetration
There are several cases on record in which extensive wounds of the abdominal parietes with protrusion and injury to the intestine have not been followed by death. Injuries to the intestines themselves have already been spoken of, but there are several cases of evisceration worthy of record.
Doughty [12.250] says that at midnight on June 7, 1868, he was called to see a man who had been stabbed in a street altercation with a negro. When first seen in the street, the patient was lying on his back with his abdomen exposed, from which protruded an enormous mass of intestines, which were covered with sand and grit; the small intestine (ileum) was incised at one point and scratched at another by the passing knife. The incision, about an inch in length, was closed with a single stitch of silk thread, and after thorough cleansing the whole mass was returned to the abdominal cavity. In this hernial protrusion were recognized four or five feet of the ileum, the cecum with its appendix, part of the ascending colon with corresponding portions of the mesentery; the distribution of the superior mesentery, made more apparent by its living pulsation, was more beautifully displayed in its succession of arches than in any dissection that Doughty had ever witnessed. Notwithstanding the extent of his injuries the patient recovered, and at last reports was doing finely.
Barnes [12.251] reports the history of a negro of twenty-five who was admitted to the Freedmen's Hospital, New Orleans, May 15, 1867, suffering from an incised wound of the abdomen, from which protruded eight inches of colon, all of the stomach, and nearly the whole of the small intestines. About 2 1/2 feet of the small intestine, having a whitish color, appeared to be filled with food and had much of the characteristic feeling of a sausage. The rest of the small intestine had a dark-brown color, and the stomach and colon, distended with gas, were leaden-colored. The viscera had been exposed to the atmosphere for over an hour. Having nothing but cold Mississippi water to wash them with, Barnes preferred returning the intestines without any attempt at removing blood and dirt further than wiping with a cambric handkerchief and the stripping they would naturally be subjected to in being returned through the opening. In ten minutes they were returned; they were carefully examined inch by inch for any wound, but none was found. Three silver sutures were passed through the skin, and a firm compress applied. The patient went to sleep shortly after his wound was dressed, and never had a single subsequent bad symptom; he was discharged on May 24th, the wound being entirely healed, with the exception of a cartilage of a rib which had not reunited.
Baillie, [12.253] Bhadoory, [12.254] Barker, Edmundson, [12.255] Johnson, [12.256] and others, record instances of abdominal wounds accompanied by extensive protrusion of the intestines, and recovery. Shah [12.257] mentions an abdominal wound with protrusion of three feet of small intestine. By treatment with ice, phenol, and opium, recovery was effected without peritonitis.
Among nonfatal perforating gunshot wounds of the abdomen, Loring: [12.258] reports the case of a private in the First Artillery who recovered after a double gunshot perforation of the abdomen. One of the balls entered 5 1/2 inches to the left of the umbilicus, and two inches above the crest of the ilium, making its exit two inches above the crest of the ilium, on a line with and two inches from the 4th lumbar vertebra. The other ball entered four inches below and to the rear of the left nipple, making its exit four inches directly below the point of entrance. In their passages these balls did not wound any of the viscera, and with the exception of traumatic fever there was no disturbance of the health of the patient. Schell [12.259] records the case of a soldier who was wounded July 3, 1867, by a conoid ball from a Remington revolver of the Army pattern. The ball entered on the left side of the abdomen, its lower edge grazing the center of Poupart's ligament, and passing backward, inward, and slightly upward, emerged one inch to the left of the spinous process of the sacrum. On July 6th all the symptoms of peritonitis made their appearance. On July 11th there was free discharge of fecal matter from both anterior and posterior wounds. This discharge continued for three days and then ceased. By August 12th both wounds were entirely healed. Mineer [12.260] reports a case of a wound from a revolver-ball entering the abdomen, passing through the colon, and extracted just above the right ilium. Under simple treatment the patient recovered and was returned to duty about ten weeks afterward.
There are a number of cases on record in which a bullet entering the abdominal cavity is subsequently voided either by the bladder or by the bowel. Ducachet [12.261] mentions two cases at the Georgetown Seminary Hospital during the late war in which Minié balls entering the abdominal wall were voided by the anus in a much battered condition. Bartlett [12.262] reports the case of a young man who was accidentally shot in the abdomen with a Colt's revolver. Immediately after the accident he complained of constant and pressing
Wounds of the liver often end very happily, and there are many cases on record in which such injuries have been followed by recovery, even when associated with considerable loss of liver-substance. In the older records, Glandorp *[380] and Scultetus mention cures after large wounds of the liver. Fabricius Hildanus reports a case that ended happily, in which a piece of liver was found in the wound, having been separated by a sword-thrust. There is a remarkable example [12.265] of recovery after multiple visceral wounds, self-inflicted by a lunatic. This man had 18 wounds, 14 having penetrated the abdomen, the liver, colon, and the jejunum being injured; by frequent bleeding, strict regimen, dressing, etc., he recovered his health and senses, but relapsing a year and a half later, he again attempted suicide, which gave the opportunity for a postmortem to learn the extent of the original injuries. Plater, *[635] Schenck, Cabrolius, *[245] the Ephemerides, and Nolleson [12.266] mention recovery after wounds of the liver. Salmuth *[706] and the Ephemerides report questionable instances in which portions of the liver were ejected in violent vomiting. Macpherson [12.267] describes a wound of the liver occurring in a Hindoo of sixty who had been struck by a spear. A portion of the liver was protruding, and a piece weighing 1 1/4 ounces was removed, complete recovery following.
Postempski [12.268] mentions a case of suture of the liver after a stab-wound. Six sutures of chromicized cat-gut were carefully tightened and fastened with a single loop. The patient left his bed on the sixth day and completely recovered. Gann [12.269] reports a case of harpoon-wound of the liver. While in a dory spearing fish in the Rio Nuevo, after a sudden lurch of the boat, a young man of twenty-eight fell on the sharp point of a harpoon, which penetrated his abdomen. About one inch of the harpoon was seen protruding from below the tip of the ensiform cartilage; the harpoon was seven inches long. It was found that the instrument had penetrated the right lobe of the liver; on passing the hand backward along the inferior surface of the liver, the point
Romme [12.270] discusses the subject of punctured wounds of the liver, as a special text using the case of the late President Carnot. He says that in 543 cases of traumatism of the liver collected by Elder, 65 were caused by cutting or sharp-pointed instruments. Of this group, 23 recovered and 42 died. The chief causes of death were hemorrhage and peritonitis. The principal symptoms of wounds of the liver, such as traumatic shock, collapse, local and radiating pains, nausea, vomiting, and respiratory disturbances were all present in the case of President Carnot. From an experience gained in the case of the President, Romme strongly recommends exploratory celiotomy in all penetrating wounds of the liver. Zeidler [12.271] reports three cases of wound of the liver in which recovery ensued. The hemorrhage in one case was arrested by the tampon, and in the other by the Pacquelin cautery.
McMillan [12.272] describes a man of twenty who was kicked by a horse over the liver and rupturing that organ. A large quantity of offensive fluid was drawn off from the liver, and the man recovered. Frazer [12.273] reports a case of rupture of liver and kidney in a boy of thirteen who was squeezed between the tire and driving chain of a mill, but who recovered despite his serious symptoms. Allen [12.274] mentions recovery after an extensive incised wound of the abdomen, liver, and lung. Massie [12.275] cites an instance of gunshot wound of the right hypochondrium, with penetration and protrusion of the liver. The patient, a boy of seven, recovered after excision of a small part of the protruding liver. Lawson Tait has incised the liver to the extent of three inches, evacuated two gallons of hydatids, and obtained successful recovery in ten weeks.
There are several cases of wound of the liver followed by recovery reported by surgeons of the United States Army. [12.276] Whitehead mentions a man of twenty-two who on June 3, 1867, was shot in the liver by a slug from a pistol. At the time of the injury he bled freely from the wound of entrance continuing to lose blood and bile until daylight the next morning, when the hemorrhage ceased, but the flow of bile kept on. By June 10th there was considerable improvement, but the wound discharged blood-clots, bile, and serum. When the patient left the hospital on July 15th the wound was healthy, discharging less than 1 1/2 ounces during the twenty-four hours, of a mixture of free bile, and bile mixed with thick material. When last heard from—July 27, 1867—the patient was improving finely in flesh and strength. McKee mentions a commissary-sergeant stationed at Santa Fe,
Resection of the Liver.—It is remarkable to what extent portions of the liver may be resected by the knife, cautery, or ligature, and the patient recover. Langenbuch records a case in which he successfully removed the greater portion of the left lobe of a woman of thirty. The lobe had been extensively deformed by tight lacing, and caused serious inconvenience. There was considerable hemorrhage, but the vessels were secured, and the woman made a good recovery. *[845] McWhinnie, in The Lancet, records a case of dislodgment of an enlarged liver from tight lacing. Terrilon [12.277] mentions an instance in which a portion of the liver was removed by ligature after celiotomy. The ligature was removed in seven days, and the sphacelated portion of the liver came off with it. A cicatrix was completed at the end of six weeks, and the patient, a woman of fifty-three,
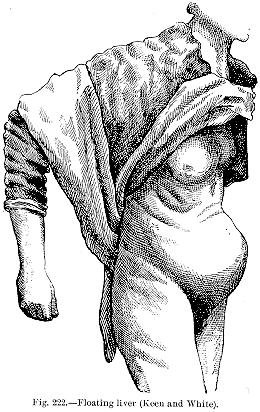
made an excellent recovery. Bastianelli [12.278] discusses those cases in which portions of the liver, having been constricted from the general body of the organ and remaining attached by a pedicle, give rise to movable tumors of the abdomen. He records such a case in a woman of thirty-seven who had five children. A piece of liver weighing 500 grams was removed, and with it the gall-bladder, and the patient made an uninterrupted recovery. Tricomi reports a case in which it was found necessary to remove the left lobe of the liver. An attempt had been made to remove a liver-tumor the size of a fist by constricting the base with an elastic ligature. This attempt was a failure, and cure was also unsuccessfully
Floating liver is a rare malady in which the liver forms an abdominal prominence that may be moved about, and which changes its situation as the patient shifts the attitude. The condition usually arises from a lax abdominal wall following repeated pregnancies. The accompanying illustration (Fig. 222) exhibits a typical case verified by postmortem examination. *[845]
Hypertrophy of the Liver.—The average weight of the normal liver is from 50 to 55 ounces, but as noted by Powell, *[642] it may become so hypertrophic as to weigh as much as 40 pounds. Bonet describes a liver weighing 18 pounds; and in his "Medical and Surgical Observations,'' Gooch speaks of a liver weighing 28 pounds. Vieussens, the celebrated anatomist, [12.280] reports an instance in which the liver weighed 20 pounds, and in his "Aphorisms,'' Vetter cites a similar instance. In 1811 Kraus of Germany describes a liver weighing 25 pounds; modern instances of enlarged liver are too numerous to be quoted here.
Rupture of the gall-bladder, although generally followed by death, is not always fatal. In such cases bile is usually found in the abdominal cavity. Fergus [12.281] mentions a case in which, after this accident, the patient was considered convalescent and was walking about, when, on the seventh day, peritonitis suddenly developed and proved fatal in two days. Several cases of this accident have been reported as treated successfully by incision and drainage (Lane) or by inspiration (Bell). In these cases large quantities of bile escaped into the abdominal cavity. Peritonitis does not necessarily follow. *[845] Cholecystotomy for the relief of the distention of the gall-bladder from obstruction of the common or cystic duct and for the removal of gall-stones was first performed in 1867 by Bobbs of Indianapolis, but it is to Marion Sims, in 1878, that perfection of the operation is due. It has been gradually improved and developed, until today it is a most successful operation. Tait reports 54 cases with 52 perfect recoveries. Cholyecystectomy, or excision of the gall-bladder, was first practiced in 1880 by Langenbuch of Berlin, and is used in cases in which gall-stones are repeatedly forming. Ashhurst's statistics show only four deaths in 28 cases.
At St. Bartholomew's Hospital, in London, is a preserved specimen of a gall-bladder which had formed the contents of a hernial sac, and which, near the fundus, shows a constriction caused by the femoral ring. It was
The fatality of rupture of the spleen is quite high. Out of 83 cases of injury to this organ collected by Elder, and quoted by MacCormac, only 11 recovered; but the mortality is less in punctured or incised wounds of this organ, the same authorities mentioning 29 recoveries out of 35 cases. In his "Surgery'' Gooch says that at the battle of Dettingen one of Sir Robert Rich's Dragoons was left all night on the field, weltering in his blood, his spleen hanging out of his body in a gangrenous state. The next morning he was carried to the surgeons who ligated the large vessels, and extirpated the spleen; the man recovered and was soon able to do duty. In the Philosophical Transactions [12.282] there is a report of a man who was wounded in the spleen by a large hunting-knife. Fergusson found the spleen hanging from the wound and ligated it. It separated in ten days and the patient recovered.
Williams [12.283] reports a stab-wound of the spleen in a negro of twenty-one. The spleen protruded, and the protruding part was ligated by a silver wire, one-half of the organ sloughing off; the patient recovered. Sir Astley Cooper mentions a curious case, in which, after vomiting, during which the spleen was torn from its attachments, this organ produced a swelling in the groin which was supposed to be a hernia. The vomiting continued, and at the end of a week the woman died; it was then found that the spleen had been turned half round on its axis, and detached from the diaphragm; it had become enlarged; the twist interrupted the return of the blood. Portal [12.284] speaks of a rupture of the spleen simply from engorgement. There was no history of a fall, contusion, or other injury. Tait [12.285] describes a case of rupture of the spleen in a woman who, in attempting to avoid her husband's kick, fell on the edge of the table. There were no signs of external violence, but she died the third day afterward. The abdomen was found full of blood, and the spleen and peritoneal covering was ruptured for three inches.
Splenectomy, excision of the spleen, has been performed a number of times, with varying results, but is more successful when performed for injury than when for disease. Ashhurst *[174] has tabulated a total of 109 operations, 27 having been for traumatic causes, and all but five having terminated successfully; of 82 operations for disease, only 32 recovered. Vulpius has collected 117 cases of splenectomy, with a death-rate of 50 per gent. If, however,
Abnormalities of Size of the Spleen.—The spleen may be extremely small. Storck [12.290] mentions a spleen that barely weighed an ounce; Schenck speaks of one in the last century that weighed as much as 20 pounds. Frank *[351] describes a spleen that weighed 16 pounds; there is another record of one weighing 15 pounds. [12.291] Elliot [12.292] mentions a spleen weighing 11 pounds; Burrows [12.293] one, 11 pounds; Blasius, four pounds; Osiander, nine pounds; Blanchard, *[213] 31 pounds; Richardson, [12.294] 3 1/2 pounds; and Hare, [12.295] 93 ounces.
The thoracic duct, although so much protected by its anatomical position, under exceptional circumstances has been ruptured or wounded. Kirchner [12.296] has collected 17 cases of this nature, two of which were due to contusions of the chest, one each to a puncture, a cut, and a shot-wound, and three to erosion from suppuration. In the remaining cases the account fails to assign a definite cause. Chylothorax, or chylous ascites, is generally a result of this injury. Krabbel mentions a patient who was run over by an empty coal car, and who died on the fifth day from suffocation due to an effusion into the right pleural cavity. On postmortem examination it was found
Manley [12.297] reports a case of rupture of the thoracic duct in a man of thirty-five, who was struck by the pole of a brewery wagon; he was knocked down on his back, the wheel passing squarely over his abdomen. There was subsequent bulging low down in the right iliac fossa, caused by the presence of a fluid, which chemic and microscopic examination proved was chyle. From five to eight ounces a day of this fluid were discharged, until the tenth day, when the bulging was opened and drained. On the fifteenth day the wound was healed and the man left the hospital quite restored to health.
Keen has reported four instances of accidental injury to the thoracic duct, near its termination at the base of the left side of the neck; the wounding was in the course of removals for deep-seated growths in this region. Three of the cases recovered, having sustained no detriment from the injury to the thoracic duct. One died; but the fatal influence was not specially connected with the wound of the duct.
Possibly the boldest operation in the history of surgery is that for ligation of the abdominal aorta for inguinal aneurysm. It was first practiced by Sir Astley Cooper in 1817, and has since been performed several times with a uniformly fatal result, although Monteiro's patient survived until the tenth day, and there is a record in which ligature of the abdominal aorta did not cause death until the eleventh day. [12.298] Loreta of Bologna is accredited with operating on December 18, 1885, for the relief of a sailor who was suffering from an abdominal aneurysm caused by a blow. An incision was made from the ensiform cartilage to the umbilicus, the aneurysm exposed, and its cavity filled up with two meters of silver-plated wire. Twenty days after no evidence of pulsation remained in the sac, and three months later the sailor was well and able to resume his duties.
Ligation of the common iliac artery, which, in a case of gunshot injury, was first practiced by Gibson of Philadelphia in 1812, is, happily, not always fatal. Of 82 cases collected by Ashhurst, 23 terminated successfully.
Foreign bodies loose in the abdominal cavity are sometimes voided at stool, or may suppurate externally. Fabricius Hildanus *[334] gives us a history of a person wounded with a sword-thrust into the abdomen, the point breaking
There are several instances on record of tolerance of foreign bodies in the skin and muscles of the back for an extended period. Gay [12.303] speaks of a curious case in which the point of a sheath-knife remained in the back of an individual for nine years. Bush reported to Sir Astley Cooper [12.304] the history of a man who, as he supposed, received a wound in the back by canister shot while serving on a Tartar privateer in 1779. There was no ship-surgeon on board, and in about a month the wound healed without surgical assistance. The man suffered little inconvenience and performed his duties as a seaman, and was impressed into the Royal Navy. In August, 1810, he complained of pain in the lumbar region. He was submitted to an examination, and a cicatrix of this region was noticed, and an extraneous body about 1/2 inch under the integument was felt. An incision was made down it, and a rusty blade of a seaman's clasp-knife extracted from near the 3d lumbar vertebra. The man had carried this knife for thirty years. The wound healed in a few days and there was no more inconvenience.
Fracture of the lower part of the spine is not always fatal, and notwithstanding the lay-idea that a broken back means certain death, patients with well-authenticated cases of vertebral fracture have recovered. Warren [12.305] records the case of a woman of sixty who, while carrying a clothes-basket, made a misstep and fell 14 feet, the basket of wet clothes striking the right shoulder, chest, and neck. There was fracture of the 4th dorsal vertebra at the transverse processes. By seizing the spinous process it could be bent backward and forward, with the peculiar crepitus of fractured bone. The clavicle was fractured two inches from the acromial end, and the sternal end was driven high up into the muscles of the neck. The arm and hand were paralyzed, and the woman suffered great dyspnea. There was at first a grave emphysematous condition due to the laceration of several broken ribs. There was also suffusion and ecchymosis about the neck and shoulder. Although complicated with tertiary syphilis, the woman made a fair recovery,
The results sometimes following the operation of laminectomy for fracture of the vertebræ are often marvelous. One of the most successful on record is that reported by Dundore. [12.306] The patient was a single man who lived in Mahanoy, Pa., and was admitted to the State Hospital for Injured Persons, Ashland, Pa., June 17, 1889, suffering from a partial dislocation of the 9th dorsal vertebra. The report is as follows—"He had been a laborer in the mines, and while working was injured March 18, 1889, by a fall of top rock, and from this date to that of his admission had been under the care of a local physician without any sign of improvement. At the time of his admission he weighed but 98 pounds, his weight previous to the injury being 145. He exhibited entire loss of motion in the lower extremities, with the exception of very slight movement in the toes of the left foot; sensation was almost nil up to the hips, above which it was normal; he had complete retention of urine, with a severe cystitis. His tongue was heavily coated, the bowels constipated, and there was marked anorexia, with considerable anemia. His temperature varied from 99° to 100° in the morning, and from 101° to 103° in the evening. The time which had elapsed since the accident precluded any attempt at reduction, and his anemic condition would not warrant a more radical method.
"He was put on light, nourishing diet, iron and strychnin were given internally, and electricity was applied to the lower extremities every other day; the cystitis was treated by irrigating the bladder each day with Thiersch's solution. By August his appetite and general condition were much improved, and his weight had increased to 125 pounds, his temperature being 99° or less each morning, and seldom as high as 100° at night. The cystitis had entirely disappeared, and he was able, with some effort, to pass his urine without the aid of a catheter. Sensation in both extremities had slightly improved, and he was able to slightly move the toes of the right foot. This being his condition, an operation was proposed as the only means of further and permanent improvement, and to this he eagerly consented, and, accordingly, on the 25th of August, the 9th dorsal vertebra was trephined.
"The cord was found to be compressed and greatly congested, but there was no evidence of laceration. The laminæ and spinous processes of the 8th and 9th dorsal vertebræ were cut away, thus relieving all pressure on the cord; the wound was drained and sutured, and a plaster-of-Paris jacket applied, a hole being cut out over the wound for the purpose of changing the dressing when necessary. By September 1st union was perfect, and for the next month the patient remained in excellent condition, but without any sign of improvement as to sensation and motion. Early in October he was able
Although few cases show such wonderful improvement as this one, statistics prove that the results of this operation are sometimes most advantageous. Thorburn [12.307] collects statistics of 50 operations from 1814 to 1885, undertaken for relief of injuries of the spinal cord. Lloyd [12.308] has compiled what is possibly the most extensive collection of cases of spinal surgery, his cases including operations for both disease and injury. White has collected 37 cases of recent date; and Chipault [12.309] reports two cases, and collected 33 cases. Quite a tribute to the modern treatment by antisepsis is shown in the results of laminectomy. Of his non-antiseptic cases Lloyd reports a mortality of 65 per cent.; those surviving the operation are distributed as follows: Cured, one; partially cured, seven; unknown, two; no improvement, five. Of those cases operated upon under modern antiseptic principles, the mortality was 50 per cent.; those surviving were distributed as follows: Cured, four; partially cured, 15; no improvement, 11. The mortality in White's cases, which were all done under antiseptic precautions, was 38 per cent. Of those surviving, there were six complete recoveries, six with benefit, and 11 without marked benefit. Pyle [12.310] collects 52 cases of spinal disease and injury, in which laminectomy was performed. All the cases were operated upon since 1890. Of the 52 cases there were 15 deaths (a mortality of 29.4 per cent.), 26 recoveries with benefit, and five recoveries in which the ultimate result has not been observed. It must be mentioned that several of the fatal cases reported were those of cervical fracture, which is by far the most fatal variety.
Injury to the spinal cord does not necessarily cause immediate death. Mills and O'Hara, both of Philadelphia, have recorded instances of recovery after penetrating wound of the spinal marrow. [12.311] Eve [12.312] reports three cases of gunshot wound in which the balls lodged in the vertebral canal, two of the patients recovering. He adds some remarks on the division of the spinal cord without immediate death.
Ford [12.313] mentions a gunshot wound of the spinal cord, the patient living ten days; after death the ball was found in the ascending aorta. Henley [12.314] speaks of a mulatto of twenty-four who was stabbed in the back with a knife. The
Although the word hernia can be construed to mean the protrusion of any viscus from its natural cavity through normal or artificial openings in the surrounding structures, the usual meaning of the word is protrusion of the abdominal contents through the parietes—what is commonly spoken of as rupture. Hernia may be congenital or acquired, or may be single or multiple —as many as five having been seen in one individual. [12.315] More than two-thirds of cases of rupture suffer from inguinal hernia In the oblique form of inguinal hernia the abdominal contents descend along the inguinal canal to the outer side of the epigastric artery, and enter the scrotum in the male, and the labium majus in the female. In this form of hernia the size of the sac is sometimes enormous, the accompanying illustration showing extreme cases of both scrotal and labial hernia *[845] (Plate 7). Umbilical hernia may be classed under three heads: congenital, infantile, and adult. Congenital umbilical hernia occurs most frequently in children, and is brought about by the failure of the abdominal walls to close. When of large size it may contain
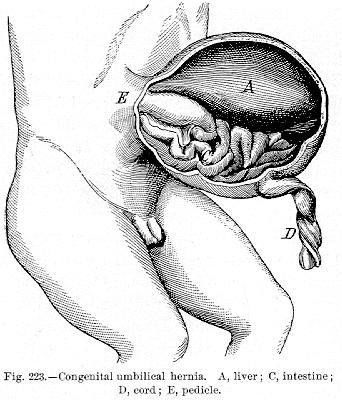
not only the intestines, but various other organs, such as the spleen, liver, etc. (Fig. 223). In some monsters all the abdominal contents are contained in the hernia. Infantile umbilical hernia is common, and appears after the separation of the umbilical cord; it is caused by the yielding of the cicatrix in this situation. It never reaches a large size, and shows a tendency to spontaneous cure. Adult umbilical hernia rarely commences in infancy. It is most commonly seen in persons with pendulous bellies, and is sometimes of enormous size, in addition to the ordinary abdominal contents, containing even the stomach and uterus. A few years since there was a man in Philadelphia past middle age, the victim of adult umbilical hernia so pendulous that while walking he had to support it with his arms and hands. It was said that this hernia did not enlarge until after his service as a soldier in the late war.
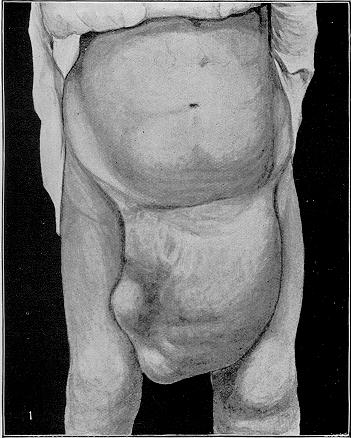
PLATE 7.
[Description: Drawing of a large scrotal hernia]
Fig. 1.—Large scrotal hernia.
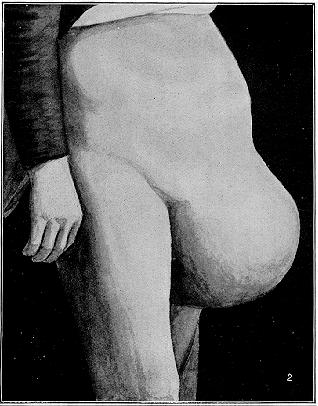
Fig. 2.—Large labial hernia (Keen and White).
[Description: Drawing of large labial hernia]
Pim [12.317] saw a colored woman of twenty-four who, on December 29, 1858, was delivered normally of her first child, and who died in bed at 3 A. M. on February 12, 1859. The postmortem showed a tumor from the ensiform cartilage to the symphysis pubis, which contained the omentum, liver (left lobe), small intestines, and colon. It rested upon the abdominal muscles of the right side. The pelvic viscera were normally placed and there was no inguinal nor femoral hernia.
Hulke [12.318] reports a case remarkable for the immense size of the rupture which protruded from a spot weakened by a former abscess. There was a partial absence of the peritoneal sac, and the obstruction readily yielded to a clyster and laxative. The rupture had a transverse diameter of 14 1/2 inches, with a vertical diameter of 11 1/2 inches. The opening was in the abdominal walls outside of the internal inguinal ring. The writhings of the intestines were very conspicuous through the walls of the pouch.
Dade [12.319] reports a case of prodigious umbilical hernia (Fig. 224). The patient was a widow of fifty-eight, a native of Ireland. Her family history was
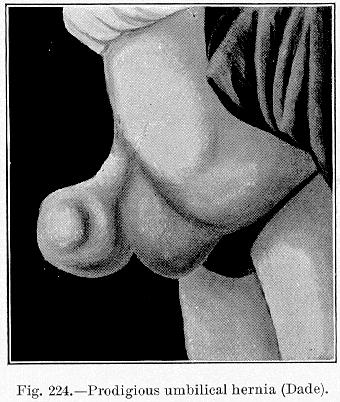
good, and she had never borne any children. The present dimensions of the tumor, which for fifteen years had been accompanied with pain, and had progressively increased in size, are as follows: Circumference at the base, 19 1/2 inches; circumference at the extremity, 11 1/4 inches; distance of extremity from abdominal wall, 12 3/4 inches. Inspection showed a large lobulated tumor protruding from the abdominal wall at the umbilicus. The veins covering it were prominent and distended. The circulation of the skin was defective, giving it a blue appearance. Vermicular contractions of the small intestines could be seen at the distance of ten feet. The tumor was soft and velvety to the touch, and could only partially be reduced. Borborygmus could be easily heard. On percussion the note over the bulk was tympanitic, and dull at the base. The distal extremity contained a portion of the small intestine instead of the
A peculiar form of hernia is spontaneous rupture of the abdominal walls, which, however, is very rare. There is an account of such a case [12.320] in a woman of seventy-two living in Pittsburg, who, after a spasmodic cough, had a spontaneous rupture of the parietes. The rent was four inches in length and extended along the linea alba, and through it protruded a mass of omentum about the size of a child's head. It was successfully treated and the woman recovered. Wallace [12.321] reports a case of spontaneous rupture of the abdominal wall, following a fit of coughing. The skin was torn and a large coil of ileum protruded, uncovered by peritoneum. After protracted exposure of the bowel it was replaced, the rent was closed, and the patient recovered.
| CHAPTER XII.
SURGICAL ANOMALIES OF THE THORAX AND
ABDOMEN. Anomalies and Curiosities of Medicine | ||