| CHAPTER II.
POSTURE IN LABOR. Labor Among Primitive Peoples | ||
The Position of Women among Civilized Races of the Present Day in the Agony of the Expulsive Pains.
Abler obstetricians than myself have undoubtedly understood the movements of women, and the positions which they assumed in the agony of the expulsive pains. As regards myself, I must candidly confess this was not the case; and it was not until I had undertaken this work, and had begun to study the positions assumed by savage and civilized people during labor, that I began to understand that there was a method in the instinctive movements of women in the last stage of labor. I had seen them toss about, and sought to quiet them; I bade them have patience, and lie still upon their backs; but, since entering upon this study, I have learned to look upon their movements in a very different light. I have watched them with interest and profit, and believe that I have learned to understand them. It has often appeared to me, as I sat watching a tedious labor case, how unnatural was the ordinary obstetric position for one parturient woman; the child is forced, I may say, upwards through the pelvic canal in the face of gravity, which acts in the intervals between the pains, and permits the presenting part of the child to sink back again, down the inclined canal. If we look upon the structure of the pelvis,
The contractions of the previously inactive and rested abdominal muscles are a powerful adjunct to the tired uterine fibre, in the last prolonged and decisive expulsory effort, and in the dorsal decubitus they are somewhat hampered; they act to the best advantage in the inclined positions, semi-recumbent, kneeling, or squatting. We know that the squatting position is the one naturally assumed if an effort is required to expel the contents of the pelvic viscera; we, moreover, all know how difficult, even impossible, it is for many to perform those functions recumbent in bed, and mainly because they have not sufficient control of the abdominal muscles in that position. Much more is this the case in the expulsion of the child; but the recumbent position is sanctioned by custom; it is pointed out as apparently convenient; it is imperatively demanded by prudery, and by a false modesty which hides from view the patient's body beneath the bed-clothes; and above all it is dictated by modern laws of obstetrics, the justice of which I have never dared question; we have all been taught their correctness, and we all thoughtlessly follow their dictates. There is no reason for assuming this position, though we are taught it; it is not reason, or obstetric science, but obstetric fashion which guides us,—guides us through our patients; and blindly do we, like all fashion's votaries, follow in the wake.
We have seen in the first part of this paper that the recumbent position is one but rarely taken by women among savage tribes, or among people who still follow their instinct and not the dictates of the latest obstetric fashion. Now what does civilized woman in the hands of the modern obstetrician do when in the intense agony of the last expulsive pains? She loses control of herself, forgets the admonition of her physician, and gives way to her own instinct.
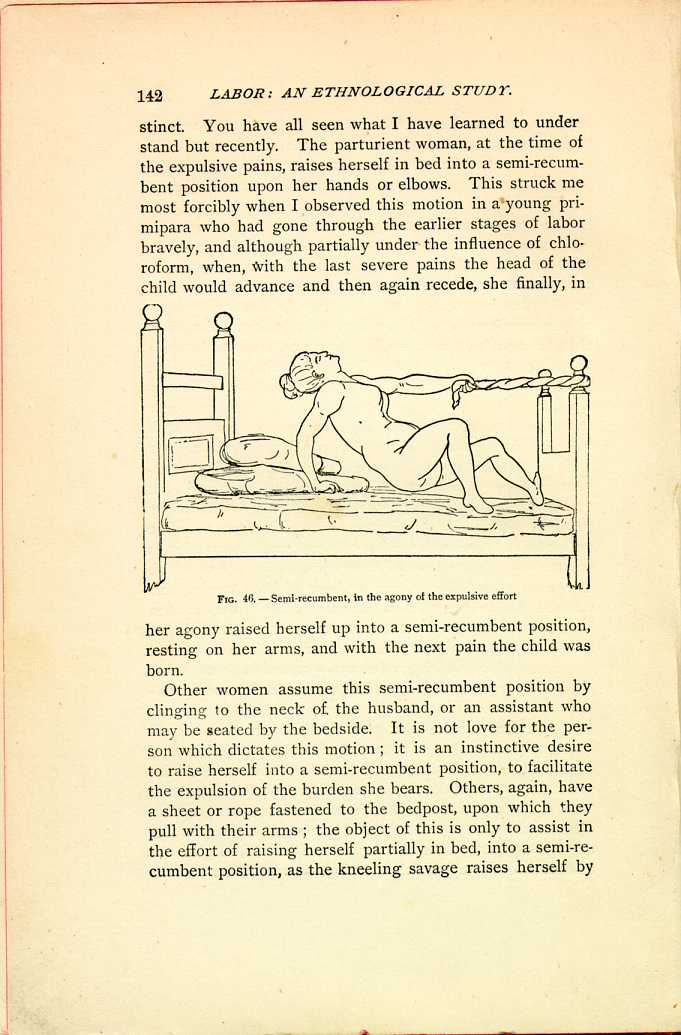
FIG. 46.—Semi-recumbent, in the agony of the expulsive effort
[Description: Woman on bed holds herself up with one arm while using the other to hold onto a rope tied to a bedpost at the foot of the bed. Black and white illustration.]Other women assume this semi-recumbent position by clinging to the neck of the husband, or an assistant who may be seated by the bedside. It is not love for the person which dictates this motion; it is an instinctive desire to raise herself into a semi-recumbent position, to facilitate the expulsion of the burden she bears. Others, again, have a sheet or rope fastened to the bedpost, upon which they pull with their arms; the object of this is only to assist in the effort of raising herself partially in bed, into a semi-recumbent position, as the kneeling savage raises herself by
I need hardly continue this evidence, as every one of the members is aware how frequently, in the last moments, a
| CHAPTER II.
POSTURE IN LABOR. Labor Among Primitive Peoples | ||