| CHAPTER V.
CHARACTERISTIC LABOR SCENES AMONG THE
YELLOW, BLACK AND RED RACES. Labor Among Primitive Peoples | ||
THE INDIANS OF THE PACIFIC COAST.
Women belonging to the Indian tribes on the northwest coast are attended in labor by a number of older squaws, as many as may be necessary. These attendants are not especially skilled midwives, but the mothers, if living near enough, or some other older friend and a few of the neighbors. It is among these people as it is among the whites, there is always some old woman in every tribe, band or settlement, who is looked upon as an authority in these cases, who is considered an expert manipulator and whose every order or suggestion is implicitly obeyed.
During the first stage of labor, the patient will usually keep on her feet, moving about the lodge, or now and then lying on her bed for a short period at a time. At the recurrence of each pain the parturient will frequently utter a plaintive cry. In this she differs somewhat from her white sister, who will most generally announce the occurrence of pain by a sound which has, by the old women, been determined "grunt,'' "grunting;'' the former gives vent to along, plaintive cry, which the word "wail'' or "whine'' seems to express more nearly than any other. When the parturient lies down she usually reclines upon her back, with the legs semi-flexed upon the thighs, the thighs likewise flexed upon the body.
No assistance is rendered at the time of a pain during the first stage, but the attendants are all ready, and willing to help when the proper time comes.
The patient takes to her bed and lies on her back—her head slightly elevated. This bed or pallet is universally on the floor, and near the fire if the weather is cold. Her legs are well flexed upon her thighs, and her thighs upon her abdomen; knees and feet are each supported by an assistant; she herself usually uses her hand to press against her thighs, or when the pains become severe, to compress her own abdomen over the fundus uteri.
The officiating accoucheur—if the term is allowable— crouches upon the pallet at the feet of the parturient, with her hands pressed upon the nates, perineum vulva or abdomen
She does not rely upon vaginal examination, nor indeed does she at all practice that means either of diagnosis or assistance to her patient.
As the case progresses, and the expulsive pains increase in severity, the abdomen of the parturient is firmly compressed over the fundus uteri by the hands of an assistant. She now uses her own hands to press upon her thighs, and does not pull at the hands of an attendant as so many white women do.
The abdominal manipulations before referred to are practiced by an assistant, kneeling by the side of the patient, with her face towards the patient's feet. She spreads her fingers in such a manner as to grasp the entire fundus uteri as nearly as possible. When the uterus is being contracted by the force of nature the assistant follows the fundus with her hands, firmly grasping the organ, and gently but firmly pressing downward. When the pain subsides, she still keeps her firm hold of the uterus, and does not allow it to relax, at least she does all she can to prevent this.
If the case is a tedious one, and the head is slow to pass, another method is resorted to in addition to the one mentioned.
The woman is seized by two attendants, who grasp her around the thorax, immediately under the arms, raise her body off the bed, and support her in an erect position, so far as her body is concerned. She is permitted to rest upon her knees or feet, according to the peculiar notion of the accoucheuse, or according to attending circumstances.
By these means, and in the position above mentioned, she is as firmly supported as is possible for the attendants to do.
The abdominal pressure is firmly kept up until the end of the labor.
The accompanying illustration, although a labor scene among the Mexican Indians in the vicinity of San Luis
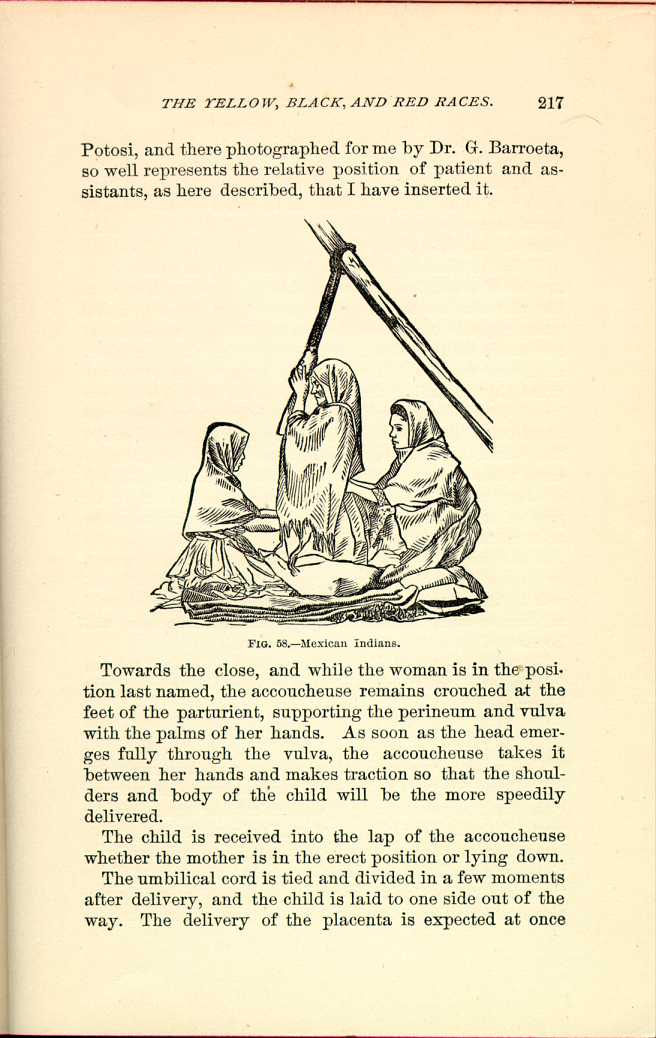
FIG. 58.—Mexican Indians.
[Description: Woman kneels, holding onto overhead rope, while two assistants attend her. Black and white illustration.]Towards the close, and while the woman is in the position last named, the accoucheuse remains crouched at the feet of the parturient, supporting the perineum and vulva with the palms of her hands. As soon as the head emerges fully through the vulva, the accoucheuse takes it between her hands and makes traction so that the shoulders and body of the child will be the more speedily delivered.
The child is received into the lap of the accoucheuse whether the mother is in the erect position or lying down.
The umbilical cord is tied and divided in a few moments after delivery, and the child is laid to one side out of the way. The delivery of the placenta is expected at once
This effort to assist the uterus in casting off the placenta is made immediately after the child is born, and stowed away in a safe place.
If the case has been an easy one, and the woman has not been raised from her couch, the first efforts to obtain the placenta are made as she lies there, the accoucheuse, making gentle but tolerable firm traction on the cord with one hand, manipulates the uterine globe with the other. At the same time, if thought necessary, an assistant will press (by spreading the fingers of both hands) and even kneed the abdomen, with the view of pressing the secundines out of the uterine cavity. If these efforts fail while the woman is in the recumbent posture, she is raised to the erect position, and thus supported, as in cases of difficult delivery of the child. The uterine globe is then firmly pressed and kneaded, whilst the accoucheuse makes more or less firm traction upon the cord.
But if the case should be one of abnormal attachment, or hour-glass contraction, they know no method of procedure that promises success. Frequently the patient will survive, escaping blood poisoning, and the secundines will be cast off in a state of disorganization.
By making persistent inquiries I learn that they seldom fail in sufficiently stimulating the uterus to cast off the placenta.
| CHAPTER V.
CHARACTERISTIC LABOR SCENES AMONG THE
YELLOW, BLACK AND RED RACES. Labor Among Primitive Peoples | ||