| The Origin and Nature of the Emotions: Miscellaneous Papers | ||
The discovery of the anesthetic properties of ether and its practical application to surgery must always stand as one of the great achievements of medicine. It is eminently fitting that the anniversary of that notable day, when the possibilities of ether were first made known to the world, should be celebrated within these walls, and whatever the topic of your Ether Day orator, he must fittingly pause first to pay tribute to that great event and to the master surgeons of the Massachusetts General Hospital. On this occasion, on behalf of the dumb animals as well as on behalf of suffering humanity, I express a deep sense of gratitude for the blessings of anesthesia.
Two years ago, an historic appreciation of the discovery of ether was presented here by Professor Welch, and last year an address on medical research was given by President Eliot. I, therefore, will not attempt a general address, but will invite your attention to an experimental and clinical study. In presenting the summaries of the large amount of data in these researches, I acknowledge with gratitude the
The scope of this paper may be explained by a concrete example. When a barefoot boy steps on a sharp stone there is an immediate discharge of nervous energy in his effort to escape from the wounding stone. This is not a voluntary act. It is not due to his own personal experience—his ontogeny—but is due to the experience of his progenitors during the vast periods of time required for the evolution of the species to which he belongs, i. e., his phylogeny. The wounding stone made an impression upon the nerve receptors in the foot similar to the innumerable injuries which gave origin to this nerve mechanism itself during the boy's vast phylogenetic or ancestral experience. The stone supplied the phylogenetic association, and the appropriate discharge of nervous energy automatically followed. If the sole of the foot be repeatedly bruised or crushed by a stone, shock may be produced; if the stone be only lightly applied, then the consequent sensation of tickling causes a discharge of nervous energy. In like manner there have been implanted in the body other mechanisms of ancestral or phylogenetic origin whose purpose is the discharge of nervous energy for the good of the individual. In this paper I shall discuss the origin and mode of action of some of these mechanisms and their relation to certain phases of anesthesia.
The word anesthesia—meaning without feeling—describes accurately the effect of ether in anesthetic dosage. Although no pain is felt in operations under inhalation anesthesia, the
There is also strong negative evidence that traumatic impulses are not excluded by ether anesthesia from the part of the brain that is apparently asleep. This evidence is as follows: If the factor of fear be excluded, and if in addition the traumatic impulses be prevented from reaching the brain by cocain[3] blocking, then, despite the intensity or the duration of the trauma within the zone so blocked, there follows no exhaustion after the effect of the anesthetic disappears, and no morphologic changes are noted in the brain-cells.
Still further negative evidence that inhalation anesthesia offers little or no protection to the brain-cells against trauma is derived from the following experiment: A dog whose spinal cord had been divided at the level of the first dorsal segment, and which had then been kept in good condition for two months, showed a recovery of the spinal reflexes, such as the scratch reflex, etc. Such an animal is known as a "spinal dog." Now, in this animal, the abdomen and hind extremities had no direct nerve connection with the brain. In this dog, continuous severe trauma of the abdominal viscera and of the hind extremities lasting for four
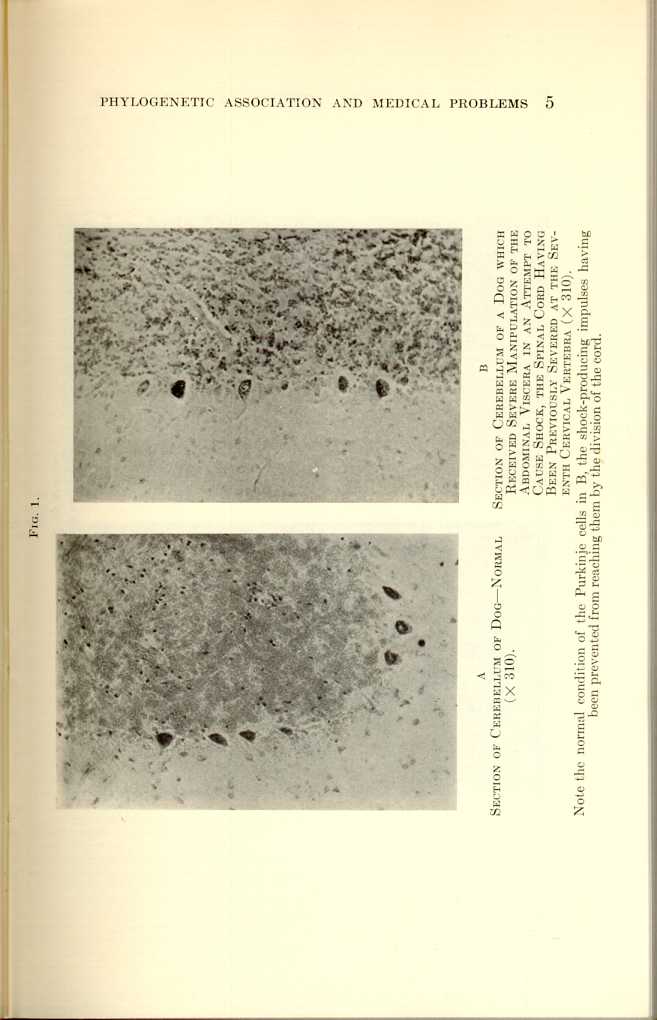
Fig. 1.
A
Section of Cerebellum of Dog—Normal (x310).
B
Section of Cerebellum of a Dog which Received Severe Manipulation of
the Abdominal Viscera in an Attempt to Cause Shock, the Spinal Cord
Having Been Previously Severed at the Seventh Cervical Vertebra
(x310).[a]
[Description: Black and white photos showing microscopic view of cerebellum of a dog
under various conditions.]
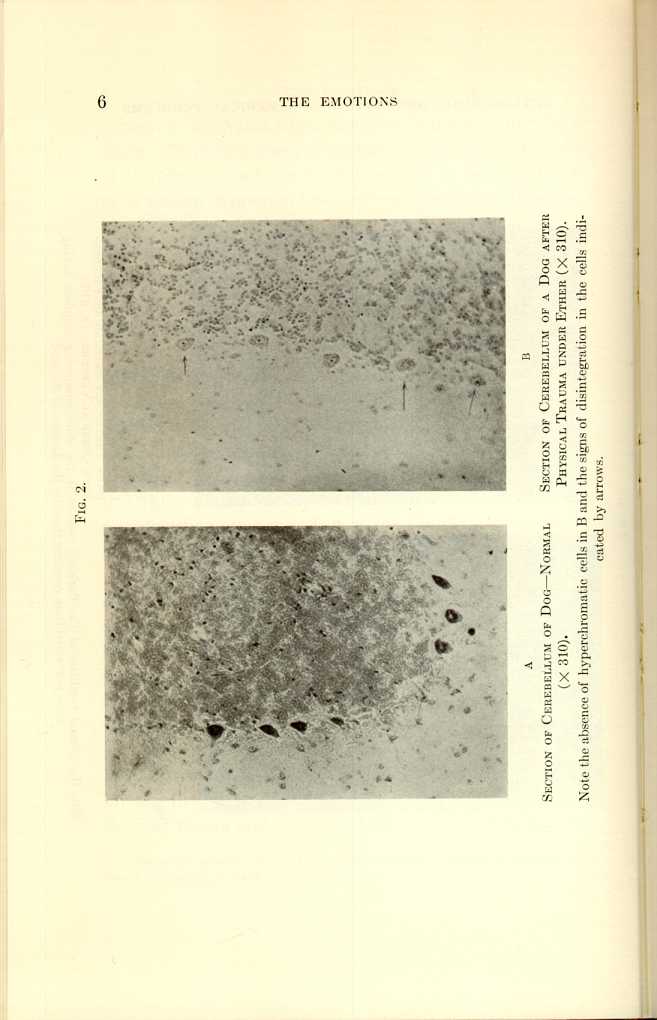
Fig. 2.
A
Section of Cerebellum of Dog—Normal (x310).
B
Section of Cerebellum of Dog after Physical Trauma under Ether
(x310).[b]
[Description: Black and white photos showing microscopic view of cerebellum of a dog
under various conditions.]
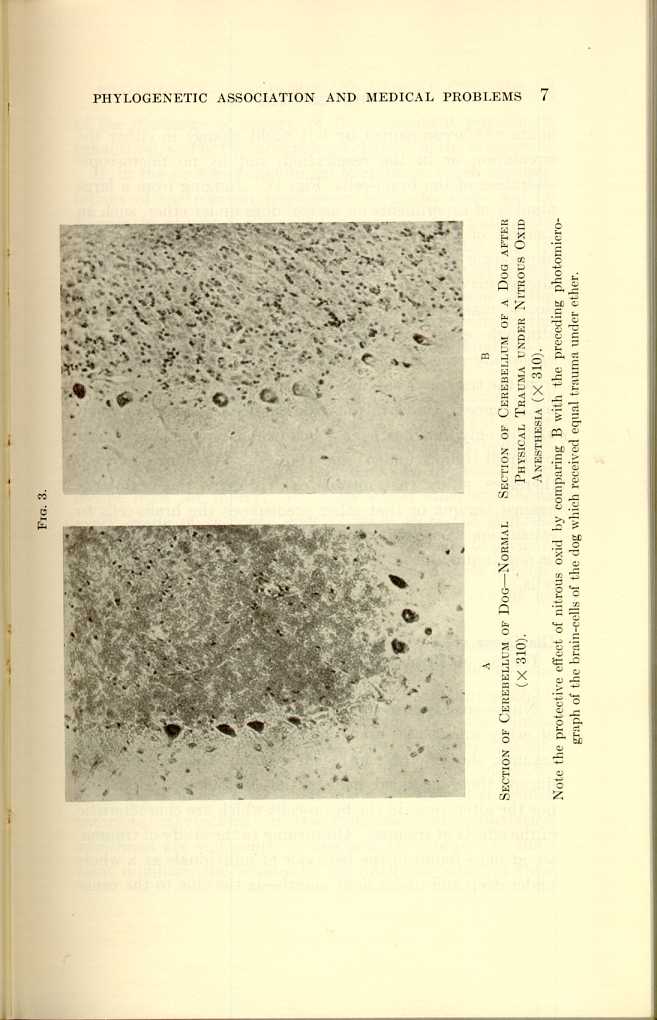
Fig. 3.
A
Section of Cerebellum of Dog—Normal (x310).
B
Section of Cerebellum of Dog after Physical Trauma under Nitrous Oxid
Anesthesia (x310).[c]
[Description: Black and white photos showing microscopic view of cerebellum
of a dog under various conditions.]
| The Origin and Nature of the Emotions: Miscellaneous Papers | ||