| The Origin and Nature of the Emotions: Miscellaneous Papers | ||
PAIN
Pain, like other phenomena, was probably evolved for a particular purpose—surely for the good of the individual; like fear and worry, it frequently is injurious. What then may be its purpose?
We postulate that pain is one of the phenomena which result from a stimulation to motor action. When a barefoot boy steps on a sharp stone it is important that the injuring contact be released as quickly as possible; and therefore physical injury pain results and impels the required action. Anemia of the soft parts at the points of pressure results from prolonged sitting or lying in one position, and as a result pain compels a muscular action that shifts the damaging pressure—this is the pain of anemia; when the rays of the blazing sun shine directly upon the retina, pain immediately causes a protective muscular action—the lid is closed, the head turns away—this is light pain; when standing too close to a blazing fire the excessive heat causes a pain which results in the protective muscular action of moving away—this is heat pain; when the urinary bladder is acutely overdistended the resultant pain induces voluntary as well as involuntary muscular contraction—this is evacuation pain; associated with defecation is a characteristic warning pain, and an active pain which induces the required muscular action—this, like the pain accompanying
Let us pass on to the discussion of another and perhaps even more interesting type of pain, that associated with infection. Not all kinds of infection are painful; and in those infections that may be associated with pain there is pain only when certain regions of the body are involved. Among the infections that are not associated with pain are scarlet fever, typhoid fever, measles, malaria, whooping-cough, typhus fever, and syphilis in its early stages. The infections that are usually, though not always, associated with pain are the pyogenic infections. The pyogenic infections and the exanthemata constitute the great majority of infections and are the basis of the discussion which follows.
I will state one of my principal conclusions first, i. e., that the only types of infection that are associated with pain are those in which the infection may be spread by muscular action or those in which the fixation of parts by continued muscular rigidity is an advantage; and, further, as a striking corollary, that the type of infection that may cause muscular action when it attacks one region of the body may cause no such action when it attacks another region.
The primary, and perhaps the most striking, difference between the painless exanthemata and the painful pyogenic infections is that in the case of the exanthemata the protective response of the body is a chemical one,—the formation of antibodies in the blood, which usually produce permanent immunity,—while the response to the pyogenic infections is largely phagocytic. In the pyogenic infections, in order
There is a third type of pain which modifies muscular action in a curious way. We have already stated that local pain serves an adaptive purpose. In this light let us now consider headache. Headache is one of the commonest initiatory symptoms of the various infections, especially of those infections which are accompanied by no local pain and by no local muscular action. In peritonitis, cholecystitis, pleurisy, arthritis, appendicitis, salpingitis, child-birth, in obstructions of the intestinal and the genito-urinary tract, in short, in those acute processes in which the local symptoms are powerful enough to govern the individual as a whole,—
On the hypothesis that it is good for the individual who is acutely stricken by a disease or who is poisoned by auto-intoxication to rest and fast, and that the muscular system obeys the imperial command of pain, and in view of the fact that the brain is not only in constant touch with the conditions of every part of the body but that it is also the controlling organ of the body, one would expect that in these diseases the major pain whose purpose it is to govern general muscular action would be located in the head and there we find it. How curious and yet how intelligible is the fact that, though a headache may be induced by even a slight auto-intoxication, an abscess may exist within the brain without causing pain. When an obliterative endarteritis is threatening a leg with anemic gangrene, or when one lies too long in the same position on a hard bed, there is threatening injury from local anemia, and as a result there is acute pain, but when the obliterative endarteritis threatens anemia of the brain, or when an embolism or thrombosis has produced anemia of the brain, there may be no accompanying pain. The probable explanation of the pain which results
Of special significance is the pain which is due to cold, which increases muscular tone and produces shivering. The general increase in muscular tone produces an interesting postural phenomenon: the limbs are flexed and the body bent forward, a position which probably is due to the fact that the flexors are stronger than the extensors. As muscular action is always accompanied by heat production, the purpose of the muscular contraction and the shivering is quite certainly caused by cold to assist in the maintenance of the normal body temperature.
We have now discussed many of the causes of pain and in each instance we have found an associated muscular action which apparently serves some adaptive purpose (Figs. 24 and 25). If we assume that pain exists for the purpose of stimulating muscular reactions, we may well inquire what part of the nervous are is the site of the sensation of pain—the nerve-endings, the trunk, or the brain? Does pain result from physical contact with the nerve-endings, with the physical act of transmitting an impression along the nerve trunk, or with the process within the brain-cells by which energy is released to cause a motor act?
It seems most probable that the site of the pain is in the brain-cells. If this be so, then what is the physical process by which the phenomena of pain are produced? The one
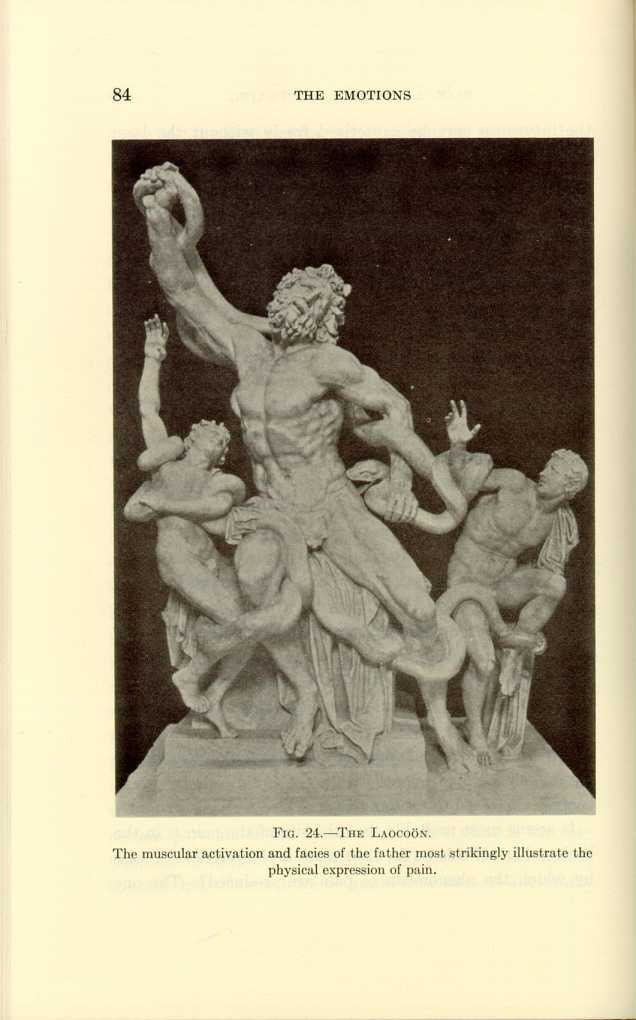
FIG. 24.—THE LAOCOÖN.
The muscular activation and facies of the father most strikingly illustrate the
physical expression of pain.
[Description: Black-and-white photograph of a sculpture depicting a man and
two youths wrestling with a snake.]
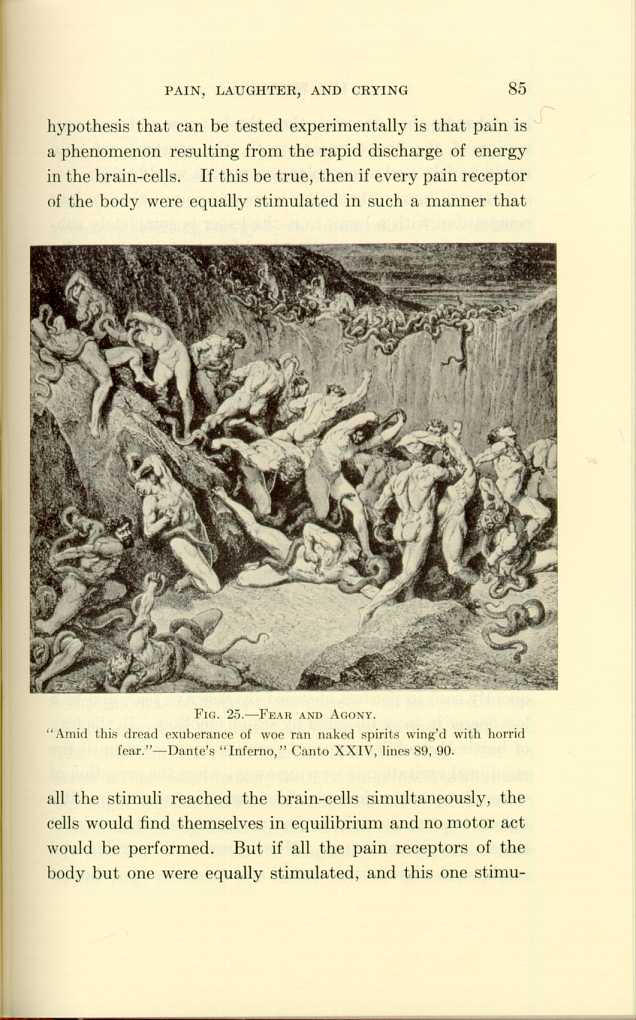
FIG. 25.—FEAR AND AGONY.
"Amid this dread exuberance of woe ran naked spirits wing'd with horrid
fear."—Dante's "Inferno," Canto XXIV, lines 89, 90.
[Description: Black-and-white illustration depicting inhabitants of Hell
being attacked by snakes.]
It is well known that when a greater pain is thrown into competition with a lesser one, the lesser is completely submerged. In this manner the school-boy initiates the novice into the mystery of the painless plucking of hair. The simultaneous, but severe application of the boot to the blindfolded victim takes complete and exclusive possession of the final common path and the hair is painlessly plucked through the triumph of the boot stimulus over the hair stimulus in the struggle for the possession of the final common path.
Another argument in favor of this hypothesis that pain is an accompaniment of the release of energy in the brain-cells is found in the fact that painless stimuli received through the special senses may completely submerge the painful stimuli of physical injury; for although the stimuli to motor action, which are received through the senses of sight, hearing, and smell, cause even more powerful motor action than those caused by physical contact stimuli, yet they are not accompanied by pain. Examples of this triumph of stimulation of the special senses over contact stimulation are frequently seen in persons obsessed by anger or fear, and to a less degree in those obsessed by sexual emotion. In the fury of battle the soldier may not perceive his wound until the emotional excitation is wearing away, when the sensation of warm blood on the skin may first attract his attention. Religious fanatics are said to feel no pain when they subject themselves to self-injury. Now, since both psychic and mechanical stimuli cause motor action by the excitation of
We will now turn to a new viewpoint, a practical as well as a fascinating one, which can best be illustrated by two case histories: A man, seventy-eight years old, whose chief complaint was obstinate constipation, was admitted to the medical ward of the Lakeside Hospital several years ago. The abdomen was but slightly distended; there was no fever, no increased leukocytosis, no muscular rigidity, and but slight general tenderness. He claimed to have lost in weight and strength during the several months previous to his admission. A tentative diagnosis of malignant tumor of the large intestine was made, but free movements were
A child, several years old, was taken ill with some indefinite disease. A number of the ablest medical and surgical consultants of a leading medical center thoroughly and repeatedly investigated the case. Although they could make no definite diagnosis they all agreed that the trouble surely could not be appendicitis because there was neither muscular rigidity nor tenderness. The autopsy showed a gangrenous appendix and general peritonitis.
How can these apparently anomalous cases be explained? These two cases are illustrations of the same principle that underlies the freedom from pain which results from the use of narcotics and anesthetics, the same principle that explains the fact that cholecystitis may occur in the aged without any other local symptoms than the presence of a mass and perhaps very slight tenderness; and that accounts in general for the lack of well-expressed disease phenomena in senility and in infancy. The reason why the aged, the very young, and the subjects of general paresis show but few symptoms of disease is that in senility the brain is deteriorated, while in infancy the brain is so undeveloped that the mechanism of association is inactive, hence pain and tenderness, which are among the oldest of the associations, are wanting. Senility and infancy are by nature normally narcotized. The senile are passing through the twilight into the night; while infants are traversing through the dawn into the day. Hence it is that the diagnosis of injury and disease in the extremes of
For the same reason, when a patient who is seriously ill with a painful disease turns upon the physician a glowing eye and an eager face, and remarks how comfortable he feels, then the end is near. This is a brilliant and fateful clinical mirage.
When one reflects on the vast amount of evidence as to the origin and the purpose of pain, he is forced to conclude that pain is a phenomenon of motor stimulation, and that its principal rôle is the protection of the individual against the gross and the microscopic enemies in his environment. The benefits of pain are especially manifested in the urgent muscular actions by means of which the body moves away from physical injury; obstructions of the hollow viscera are overcome; rest is compelled in the acute infections—the infected points are held rigidly quiet, the muscles of the abdomen are fixed, and harmful peristalsis is arrested in peritonitis; while there is absolutely no pain in the diseases or injuries which affect those regions of the body in which in the course of evolution no pain receptors were placed, or in those diseases in which muscular inhibition or contraction is of no help. In a biologic sense pain is closely associated with the emotional stimuli, for both pain and the emotions incite motor activity for the good of the individual.
The frequent occurrence of post-operative and post-traumatic pain is accounted for by the fact that the operation or the injury has lowered the threshold of the brain-cells to trauma; the brain and not the local sensitive field is the site of the pain. I have found that, by blocking
| The Origin and Nature of the Emotions: Miscellaneous Papers | ||