| CHAPTER III. THE THIRD STAGE OF
LABOR. Labor Among Primitive Peoples | ||
3. CHAPTER III.
THE THIRD STAGE OF
LABOR.
LABOR seems completed with the expulsion of the child, the one act upon which the efforts of the accoucheur and the expectations of the patient have centred, the culmination of hours of suffering and anxiety; both feel as if their work were completed, and but little thought is given by either to the remaining afterbirth which is usually expelled without much suffering to the mother, and if nature be not interfered with, rarely calls for any exertion on the part of the attendant.
Accidents occurring during the birth of the child are immediately followed by alarming results, while those happening during the delivery of the placenta can be ignored at the time, although the consequences are often disastrous. The third stage of labor accordingly excites but little interest, and is, I may almost say, unduly neglected; some radical changes have of late years been made in its treatment, but, although advocated by able obstetricians, they have by no means met with the hearty concurrence of the profession at large, of which they deserve and which their importance justifies.
My attention has been recently directed to what I may call the natural management of labor, or the customs observed during childbirth by such people as are not yet governed by modern obstetric law, and who follow the dictates of instinct in this purely mechanical function of our animal existence; my researches in regard to the position of women in labor have shown me the correctness of the course adopted by those
The management of the third stage of labor has received so little attention that I shall be obliged to confine myself, by reason of the scanty data at my command, to the leading points; I nevertheless hope to be able to develop the more important features sufficiently to show that these untutored people, following the guidance of instinct, have, as a rule, pursued a much more correct practice than can be attributed to the followers of scientific midwifery; above all they have fully appreciated, in resorting to abdominal expression, the dangers of the vis a fronte, and the importance of the vis a tergo as their main reliance for the speedy and successful removal of the placenta. Nor are the data as broad as I should like to see them; I can gather but little from the records of travellers or from the pages of history; the information I have been able to obtain is almost altogether in regard to the customs now observed among the North American Indians, and for this I am indebted to the kindly interest shown by the surgeons of the United States Army, and the physicians of the Indian Agencies who have freely responded to the questions I have put in the circular sent out through the Smithsonian Institution by the generous offices of Major J. W. Powell, the director, and others of the gentlemen connected with the Bureau of Ethnology, above all Dr. H. C. Yarrow.
I shall discuss, first, the management of the third stage of labor in simple cases, as it is customary among the various
MANAGEMENT OF SIMPLE CASES.
The placenta delivered in the same position which has been occupied during labor pains and the expulsion of the child.
Manual expression.—Among our Indians, as among all uncivilized nations, external manipulations are resorted to wherever good can be accomplished by them, and in obstetric practice massage and expression are freely and effectively used. The third stage of labor is a very short one, the placenta usually escaping very soon after the birth of the child; and by far the most common, the prevailing treatment in fact, is the one we will now consider. The patient and her assistants retain the positions relatively occupied during the birth of the child; the
The Kootenais kneel during labor, and after expulsion of the child continue to knead the abdomen, exercising the same pressure downward as when aiding the descent of the child, and in case this fails, they introduce the hand into the vagina and remove the placenta, giving the woman one joint of an unknown root to stop the hemorrhage, following it by another joint in fifteen minutes or half an hour until it does stop, with the idea
The women of the lower order of Mexicans, who are also usually delivered in the squatting posture, sometimes kneeling, follow the same custom as their Indian neighbors, but of them I am told that the third stage of labor is a much longer one. The midwife busies herself about the new-born child, while the patient is kept in her uncomfortable position, kneeling or squatting, with her rear and lateral assistants, until the placenta is expelled. This takes place seldom in less than half an hour, but generally within an hour; if not, the patient receives a more or less violent shaking, according to the exigencies of the case, the rear assistant, with her arms about the patient, actually shaking her up and down, and, if this does not answer, as a last resort, efforts are made to provoke vomiting. A decoction of some kind, either laxative or nauseating, is given the patient for the purpose of assisting the expulsion of the placenta; but among the Mexicans a cup of corn gruel, atole, is regularly given after the expulsion of the child. Among those who retain the semi-recumbent position in which they are usually delivered are the Wacos, Hoopas, lower
The Indians of the Pacific coast follow the same custom,
and they, as well as all other tribes, seem anxious to attempt
the speedy expulsion of the placenta, so that an effort is always
made to assist the uterus in casting off the remaining afterbirth
as soon as the child has been removed, and placed in a
safe place. The accoucheur makes gentle, but tolerably firm
traction on the cord with one hand, and with the other manipulates
the abdomen over the uterine globe. At the same time,
if thought necessary, the assistant will gently press the abdomen;
both hands, with the distended fingers, being laid above
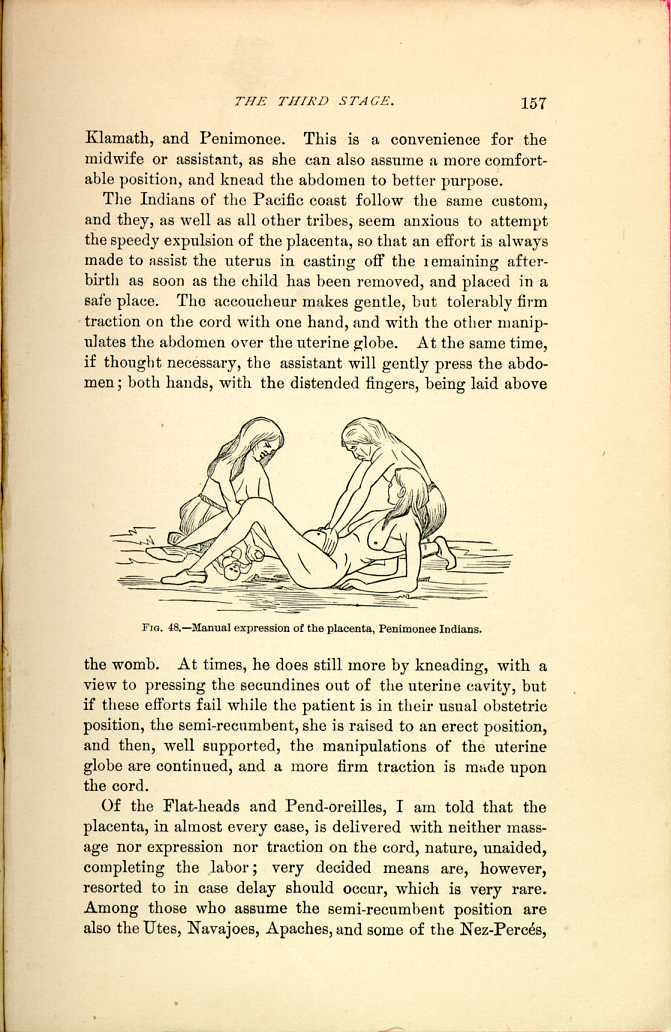
FIG. 48.—Manual expression of the placenta, Penimonee
Indians.
[Description: Woman reclines on floor, propped up on her elbows. One
assistant attends the newborn, while a second presses against the
patient's abdomen. Black and white illustration.]
Of the Flat-heads and Pend-oreilles, I am told that the placenta, in almost every case, is delivered with neither massage nor expression nor traction on the cord, nature, unaided, completing the labor; very decided means are, however resorted to in case delay should occur, which is very rare. Among those who assume the semi-recumbent position are also the Utes, Navajoes, Apaches, and some of the Nez-Percés,
The Burmese are among the very few people who adopt a dorsal decubitus as the obstetric position, and forcibly expel the placenta more by beating the abdomen than well-directed manipulations, and in extreme cases, by sitting or standing upon the abdomen and pressing with the feet upon the uterine globe.
The Makahs, of the Neah-Bay agency, retain the sitting posture in which the child is delivered, but whilst this, to them, apparently simple proceeding is always managed without professional assistance of any kind, skilled help is called as soon as the child is born. Until then nature is allowed to take its course, but as soon as the child is expelled, an old woman, who makes this a specialty, is called to deliver the afterbirth, which she does by pressing and working the abdomen constantly until the placenta and the clots are removed. This person has nothing whatsoever to do with the delivery of the child. The same position is occupied by the women of the Skokomish agency, and here, also, the very best practice is followed, the placenta being allowed to come away without any manual interference except expression over the region of the womb and a slight traction on the cord.
The Brulé Sioux and Warm Spring Indians retain the standing posture, in which the child is delivered; the midwife, standing behind the patient, aids the naturally rapid expulsion of the placenta by pressure on the fundus with her hands, varied by a kind of churning manipulation.
Intra-Abdominal Pressure.—The use of the diaphragm as a powerful aid to all efforts to expel the contents of the abdominal cavity is well-known to our midwives, and we know how frequently they direct their patients either to hold their breath or to scream, as the exigencies of the case may demand; but, fortunately, they do not resort to measures quite so violent as our Spanish neighbors in Mexico, who assist the expulsion of the placenta by vomiting the unlucky patient. Some of our Indian tribes also lay stress upon the intra-abdominal pressure, and the assistance of the diaphragm and abdominal muscles,
Traction on the Cord.—Traction upon the umbilical cord appears so natural, and is certainly so tempting a means of removing the placenta, that it is much esteemed by a class of meddlesome midwives which abounds in all civilized countries to the detriment of parturient women, but the untutored savage, guided in his practice by instinct and observation, is too shrewd to seek the removal of the retained placenta by such dangerous means.
Although it is customary, among some of our Indian tribes, to make a certain traction upon the cord, I am uniformly told that this is always done with extreme caution, and but very few make use of it to drag down the afterbirth—a manipulation fraught with so much danger, and unfortunately so common among more intelligent people.
The Crows and Creeks are usually delivered prone upon the stomach, and the placenta is rapidly expelled, either in the same posture or while standing; in rare cases it is delayed, and then it is allowed to remain until it decomposes, and, remarkable to say, pyemia rarely follows, probably on account of the naturally strong constitution of the race. Among them, gentle traction upon the funis is the only assistance accorded to nature, and if there be much resistance, it is at once stopped, and the placenta allowed to remain, in preference to attempting its delivery by stronger traction.
The Rees, Gros-Ventres, and Mandans are confined in a kneeling posture, in which the placenta also is expelled, but if it does not come away rapidly, with some little rubbing of the belly with the hands greased with turtle fat, the accoucheur pulls gently and steadily on the cord, evidently relying somewhat upon this traction for the removal of the placenta.
The worst practice is that of the Cheyennes and Arrapahoes, who retain the dorsal decubitus in which the child is expelled, but never wait for the expulsion of the placenta by the proper contraction of the womb, removing it at once by
A change of position is not infrequently made immediately after the birth of the child, with a view to hastening the expulsion of the after-birth. As this period of labor is a short one, an uncomfortable position, if otherwise advantageous, may be readily assumed; and, moreover, the muscular effort, which the patient involuntarily undergoes in making this change, will assist the contraction of the womb. The change most frequently made is to a standing posture. Thus the squaws of the Cattaranguts rise to their feet from the kneeling posture, which they occupied during the birth of the child, with the idea of facilitating the expulsion of the afterbirth. If this does not take place within a short time, the attendant makes traction on the cord, at the same time making downward pressure over the abdomen, while the parturient maintains the standing posture.
Dr. D. D. Taylor, surgeon U. S. Army, in detailing the labor of a Sioux squaw whom he delivered, seated cross-legged on the floor, says: "The moment I cut the cord she jumped to her feet, and, standing erect, seized the squaw-belt, a leather belt about four inches wide, which she buckled over her hips and abdomen, drawing it as tightly as her strength would permit. During this time the hemorrhage was very abundant; within a minute, however, the placenta dropped on the floor, the bleeding ceased, the womb becoming firmly contracted, and she sat down on a stool looking as if nothing unusual had happened. The belt was removed the next morning, and she remained up and went about the house as usual. I saw no
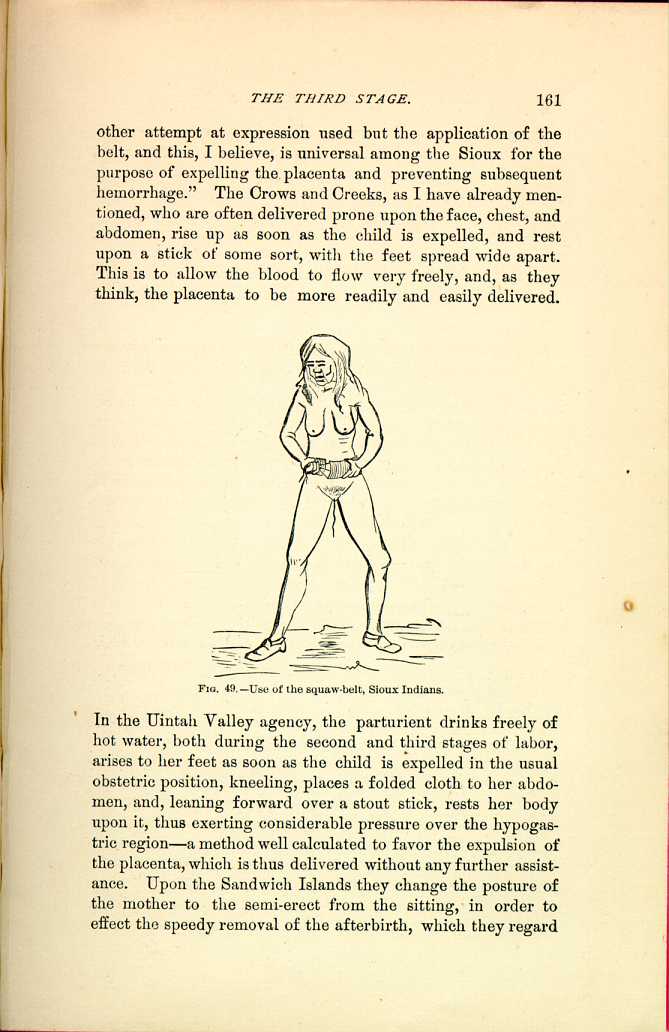
FIG. 49.—Use of the squaw-belt, Sioux Indians.
[Description: Woman stands with feet apart, holding belt around her abdomen. Black and white illustration.]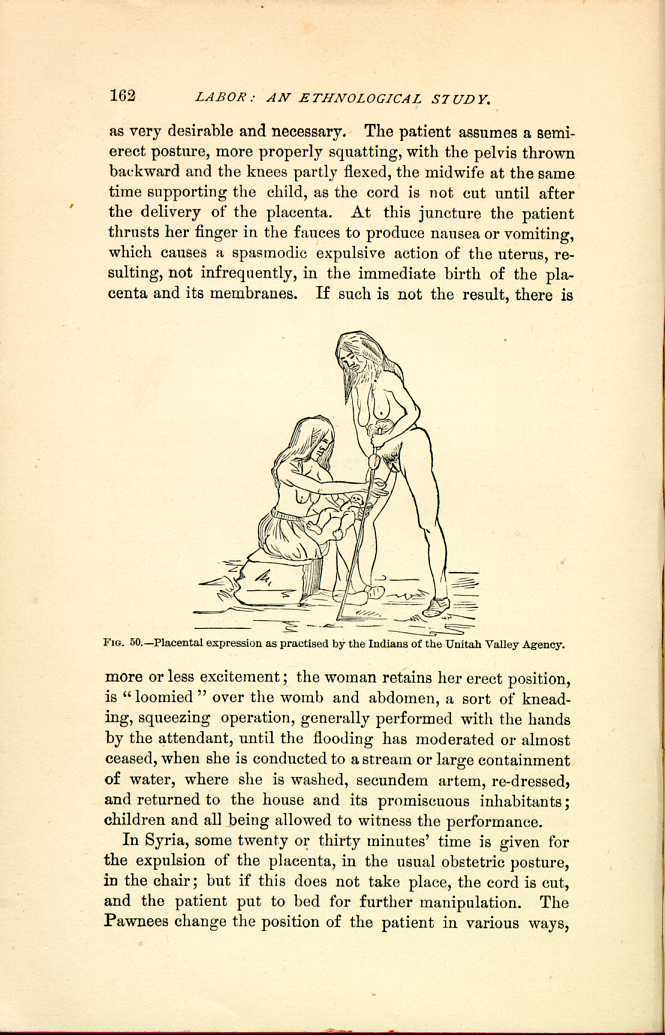
FIG. 50.—Placental expression as practiced by the Indians of the Unitah Valley Agency.
[Description: Post-partum woman stands leaning upon a pole, while an attendant, newborn in lap, works to express the placenta. Black and white illustration.]In Syria, some twenty or thirty minutes' time is given for the expulsion of the placenta, in the usual obstetric posture, in the chair; but if this does not take place, the cord is cut, and the patient put to bed for further manipulation. The Pawnees change the position of the patient in various ways,
MANAGEMENT OF THE PLACENTA IN CASE OF RETARDED EXPULSION.
We have already seen that, as a rule, the delivery of the placenta speedily follows the expulsion of the child, nature being merely assisted by the continuance of the external pressure, which serves to assist and facilitate the contraction of the uterine globe. If the placenta does not readily come, they are at a loss what to do, and the patient is often left to herself. Dr. C. M. Harrison writes from the Mexican frontier that the Indians, and lower order of Mexicans, seem to have no other method of extracting the placenta than by traction on the cord, and that he has seen women dead and dying merely from the want of having the placenta extracted. The Dakotas use most violent means, and if the delivery of the placenta is at all retarded, it is forcibly extracted, and often with fatal consequences. Other of the Indian tribes have more reasonable ways, and it is these which we will now consider. The description given me of the attempts at delivery of a retained placenta by a Mexican midwife, by Surgeon H. R. Tilton, U. S. Army, embodies many of the more violent methods resorted to. When called to the patient, he found that she had been given a quantity of raw beans, between a pint and a quart, as one remedy; these were probably intended to swell, and thus drive out the placenta. This failing, she had been vigorously choked, as another means of expelling the afterbirth. Finally, she was placed in the lap of her husband, in the obstetric position of that country, whilst he squeezed the abdomen powerfully with his encircling arms. This last expedient, by the way, is a favorite method among the Mexicans for facilitating labor, the contracting uterus being steadily followed down by the arms of the husband. After all these means had failed, the after-birth was readily removed by the surgeon, upon the introduction of the hand, but the recovery of the woman remained doubtful, after the violence to which she had been subjected.
In the Laguna Pueblo, a tea made of the corn blossoms, or
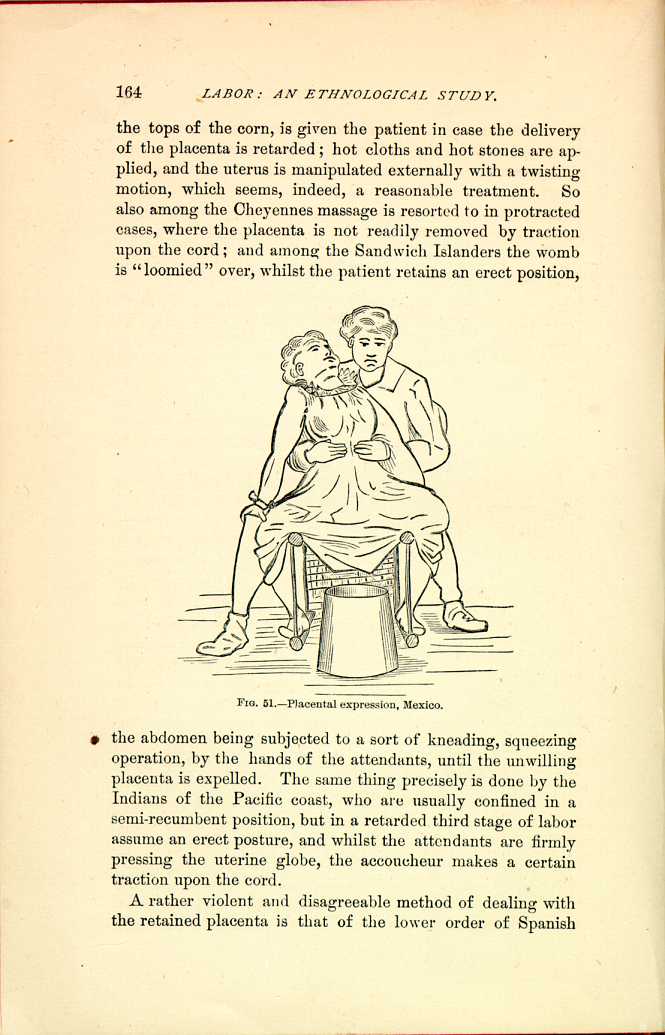
FIG. 51.—Placental expression, Mexico.
[Description: Woman sits on lap of a man, her legs apart over a cylindrical container. Black and white illustration.]A rather violent and disagreeable method of dealing with the retained placenta is that of the lower order of Spanish
The method of the Comanches is to grasp the womb, knead and compress it, make slight traction upon the cord, and efforts to reach the placenta with the hand, in which the patient as well as the assistant takes part. The Papagos pursue a course which is certainly peculiar to them, of producing a more steady and, perhaps, not too violent traction upon the cord, by so attaching it that the amount of force to be used is left to the judgment and the sensations of the patient; it seems as if her sense of pain were to serve as a safety valve for the amount of force to be expended, and thus the proper limit determined and dangerous consequences avoided. In the interesting description given me by Surgeon Charles Smart, U. S. Army, who was called in a case in which the placenta had been retained for three or four days, he found the attendants in great alarm for the safety of the mother. The patient lay on her side, with her knees drawn up, and every now and again, while he was learning the particulars of the case, she was directed to stretch herself out. The reason of this he found by introducing his hand for the purpose of making an examination; a buckskin thong, about the size of a whipcord, was made fast to the cut end of the funis, whilst the other extremity was discovered hitched around the great toe, and when she stretched the limb in bed traction was made
Since writing the above I learn that the Japanese, also, either carefully hold the projecting end of the cord or tie it to the patient's leg, in case the placenta should resist the simpler efforts directed toward its expulsion.
Among the Flat-heads, Pend-oreilles, and Kootewais, in case the usually speedy and natural expulsion of the placenta does not take place, the patient leaves the obstetric position, upon a low stool, and is made to stand and walk about, a proceeding which, though probably injurious to the delicate women of our civilization, is harmless and almost always successful among these Indians.
The Indians of the Misqually agency commonly use a steam bath in the very rare cases of retention. A hole is made in the ground and filled with hot rocks which are covered with leaves of the fir-tree; water is then poured upon them, and the woman made to sit over this vapor bath for a few minutes. This simple means seldom fails, and if it should, other help is called —maybe a woman, maybe a physician, if one is convenient.
MANAGEMENT OF THE UMBILICAL CORD.
The Indian midwives, as well as learned obstetricians, differ in their views with regard to the proper time for cutting the funis, but, as a rule, we find that the cord is not severed until labor is completed and the secundines are expelled; this practice we find among the Sandwich Islanders and among most of our Indians; the child remaining on the ground in front of the mother until the placenta is delivered; among the Kiowas, Comanches, and Wichitas, it is customary, after the placenta is delivered, that the assistant should take the cord between her fingers and squeeze such blood as may remain in it back toward the placenta, and not until then the cord is cut and tied. So also the Blackfeet, Uncapapas, Lower and Upper Yankton-ans of the Sioux nation do not sever the funis until the placenta has been expelled, while the Flatheads and Kootewais, Crows and Creeks, cut the cord at once, and I may here add that, as soon as the cord is tied and cut and the child is
Some difference also seems to exist, and probably with reason, for the methods of each, as to the distance from the child at which the funis should be tied. The Wakamba, in Africa, use threads of the best of the adansonia or monkey-bread tree, and tie the funis tightly two or three inches from the navel, the Mexicans some three inches. The Japanese tie the funis in two places, about one inch apart, close to the child's body; the Comanches, on the contrary, using only one ligature, tie the cord about a foot from the body of the child, and in Africa we find one of the tribes, the Waswahili, where the cord is also left very long and slowly dries; the navel in later years being often found the size of a fist. The Loango, of Middle Africa, on the contrary cut the cord short and dry it rapidly; it is severed at double the length of the first joint of the thumb, or is measured off to the knee, then the child is taken to the fire and the remnant of the funis is steadily pressed by the warmed fingers of the numerous attendants so as to hasten its drying, which is completed in twenty-four hours; then the withered mass is forced off with the thumb nail and burnt (Indiscretes aus Loango; Dr. Peschuel-Loesche, Ztschrft. f. Ethnolog., 1878, X., p. 29).
The Syrians tie both sides; the Catarangut Indians ligate only one end, the child's end; so also the Blackfeet, who, however, take the precaution to pinch the protruding placental end of the funis with the fingers, so as to prevent oozing.
Certain superstitions also exist in regard to the method of cutting the funis, a dull instrument being frequently used, probably on the principle of the modern saw-knife, as bruising and crushing rather than cutting, and thus preventing hemorrhage. Some of the African tribes, the Wakambi for instance, make use of their ordinary knives; the Loango, however, would deem it a misfortune to the new-born babe to use anything but the edge of the stem of a palm leaf; the Papagos of Brazil cut the cord with a sharp fragment of a vessel or a shell. The
So far my observations have been confined almost exclusively to the management of the third stage of labor among the American Indians, on account of the amount of valuable original material at my disposal; for the sake of comparison I will now add such data as I have been able to gather with regard to the treatment customary among other peoples. Some of these facts are referred to in other parts of this volume, but the greater part I owe to an instructive paper by Dr. H. H. Ploss, of Leipzig (Historisch-ethnographische Notizen zur Behandlung der Nachgeburts-Periode).
The same customs, often somewhat modified, will be found to predominate.
In Old Calabar,[1] the child, as soon as it is born, is placed between the thighs of the mother and remains there until the placenta is expelled, however long this may be. In Surinam,[2] the placenta follows the child very quickly, and little help seems to be needed. The Australian woman squats down in a small excavation in the ground prepared for that purpose, and as soon as the child has been expelled she awaits the coming of the afterbirth; the position is that as in defecation. It seems that this is a favorite position, and it seems reasonable, as many of the same muscles come in play which serve in defecation. In New Caledonia, as well as upon other Oceanic Islands, a number of old women assist the parturient, cut the cord with a shell or splint of bamboo, and tie the placental end of the navel string to the mother's toe, leaving, the expulsion to nature.
A German physician had an opportunity to observe a native of Sumatra, who, following her instincts, had the abdomen anointed with oil after the expulsion of the child, and, after some pressing, expelled the placenta with a few clots of
This leaving of the expulsion to nature has found many advocates in the last century, and a few still persist. It seems that in some of the eastern provinces, as in Galicia, the midwives do not bother about the afterbirth, and cases of retention and putrefaction are common. In Persia traction upon the navel string is said to be common. The same is said to be the case in Palestine, where, as Dr. Rosen writes, it the placenta does not rapidly follow the birth of the child, the midwife passes her well oiled fingers into the vagina to seize the placenta. If it does not approach the orifice, she ties the cord with the aid of a string to the patient's toe, and the child is wrapped up and kept warm until the placenta appears. The Chinese follow a similar method; as they attach the cord with a string to the patient's hip in order to prevent the return of the placenta. Some rest is then given the patient, after which the placenta is slowly pulled out; if it does not follow, the hand or a blunt hook is introduced. In New Caledonia the same method of tying the navel string to the patient's toe is followed, as they think the stretching of the foot will end the business. Among all people where the management of this third stage depends upon a vis a fronte, a pulling out of the placenta, the manipulation and methods of hastening its expulsion are more severe and more dangerous.
Chinese physicians advise an expectant method, and seem to consider the remaining of the placenta as less harmful than the active interference.
Chinese midwives tickle the fauces with a feather to produce vomiting, and then forcibly drag out the placenta, which is the death of many women.[3]
Inversion and prolapsus are frequent in Russia, according to Dr. Kreble, on account of the methods of dragging out the
The customs in Germany are less harmful, but often foolish enough. In the Palatinate, midwives urge the patient to cough or breathe into the hand; others rub the abdomen after pouring a few drops of spirits upon it. In Suavia it is believed that the broth of three crawfish well mashed up will expel the afterbirth.[4]
In the Bavarian Palatinate, the patient is urged to stand up in case of tardy expulsion of the placenta, take in hand her husband's walking stick, put his hat upon her head, and then she is again put to bed, almost like the trotting about of the Indian women to expel the placenta, but not quite as effective.
Dr. Damianius Georgin says that expert midwives in Greece express the afterbirth by pressure upon the abdomen, at the same time nausea is induced by placing a finger, or the braided hair of the patient, into her mouth. She is also induced to blow into an empty bottle. Others have seen[5] the Greek mother raised by her assistant several times in succession over a tripod, which serves as an obstetric chair, and suddenly dropped down upon it, continuing these shocks until the placenta is expelled. The informant states that this proceeding is quite harmless. In Jaffa, upon the coast of the Mediterranean, Dr. Tobler says that after the parturient has received a swallow of brandy the midwife forces out the placenta by a firm pressure upon the navel.
Whatever individual differences may exist, the various tribes of North American Indians demonstrate most of these methods, but as a rule are more practical.
A rather surprising conclusion is forced upon us by the study of these various methods of treatment resorted to in the third stage of labor: the untutored, simple-minded savage, although crude in the methods he pursues, obeys a correct, even if we should term it an animal, instinct, and approximates more closely to the teachings of the science of to-day—
Instinct has taught these peoples the necessity of expelling the placenta, and they attain this object by the correct means, by a vis a tergo, by expression—the Makah Indians even leaving this important duty to a specially skilled person.
Among peoples of a certain civilization a more harmful method is resorted to: it is among the Chinese, Persians, the common people of Russia, and such, that we find it customary to drag out the after-birth by the funis—whilst the more ignorant of the midwives of our great cities either follow the same pernicious habit or do worse (like those of Galicia and such border provinces), leave it in altogether, if nature, or their own dangerous traction, does not readily produce it.
The same class of people, even when pursuing correct methods, appear less reasonable, more brutal, than their more primitive brethren. Thus the Arabs, at times when impatient at the tardy progress of labor, suspend the parturient by the arms from one of the tent poles, to constrict the abdomen so as to force the fœtus down upon the perineum, whatever be the position. Others place a plank, or other large flat piece of wood, upon the belly of the mother, and place upon it a sufficient number of women to achieve the pressure necessary to expel the child: a small portable mill used for grinding barley may serve the same purpose. Should the presentation seem at fault, the patient is held up by the feet and shaken, or rolled over and over on the ground.
It is unquestionably to these rough means, more particularly traction upon the funis, that the women of these peoples are indebted for the existence and even the frequence of prolapse, the one uterine disease to which they are most subject. Although other uterine diseases undoubtedly exist, they are not so apparent to the observer, perhaps not even known to the sufferer herself, whilst prolapse above all other disturbances makes itself known; still it does not affect the nervous and physical organization of these stronger and less delicately constituted women as it does that of the ladies reared amid luxuries and excitements in the whirl of our civilization.
These accidents are probably more common upon the borders of civilization than among savages.
A partial civilization seems destructive to the natural and usually correct instinct of man, and in the relative methods of different peoples in managing this important stage of labor we find a striking expression of this fact.
PECULIAR SUPERSTITIONS AND CUSTOMS.
The Sandwich Islanders, like many of our Indians, accustomed to the speedy expulsion of the afterbirth, are in great alarm if this does not occur, and think that a rapid delivery is all important; in case their simple means do not succeed, they do not seem to worry much about the patient; the Menemonee and others leaving her often in the same position for days, whilst the Crows and Creeks and allied tribes, and the Mexicans also, cease to bother about her, leaving the placenta until it sloughs away, or the patient succumbs to the consequent pyemia. The African negroes, either on account of ignorance or superstition, rarely make any attempt at artificial removal of the retained afterbirth. Among all these savage people, a certain belief seems to exist that, if nature, aided by their simple and rational means of external expression, does not speedily expel the placenta, it must not be interfered with and they turn away from the unfortunate sufferer; should the cord tear in their efforts at traction, which fortunately are, as a rule, gentle, they give up the patient; hence we see with what care the Kootewai squaw seizes the placental end of the cord as soon as it is cut in order that it may not escape back into the womb; it is possible that some such superstition, rather than obstetric knowledge, should cause the Indian midwife to make but gentle traction on the cord, and induce her to rely mainly upon external pressure, either by belt or hand, or even such as may be caused by the efforts at vomiting; possibly it may have been the teaching of some shrewd law-giver, but there is certainly some fear which prevents the women of savage tribes from making that dangerous traction upon the navel string which is so common among their white sisters; it is truly unfortunate that no such superstitious fear governs the civilized midwife.
A peculiar trait is also developed among many of these people which we are familiar with in the superstitions of some of
FIG. 53—Vessels in which the placenta is buried, Japan.
[Description: Two box-like containers, one shaped like a clamshell, the other cylindrical, with a round lid. Both appear to be bound with twine. Black and white illustration.]A peculiar superstition is that of the Loango, who hasten the drying of the navel, force it off within twenty-four hours, and burn it, believing that the child would fall into evil ways if the remnant of the funis should become food for the rats, and as long as the navel is still on the child, no male being, not even the father, is admitted to the presence of the new-born.
CONCLUSIONS.
The same doubts as to the proper management of the third stage of labor which have annoyed our obstetricians seem to have arisen in the savage mind. We find various customs existing among the different tribes and people, and, right or wrong, they cling to them with the pertinacity of the modern writer, well satisfied with the correctness of his own view. We find the same methods and the same errors, an occasional yielding to the same temptations which beset the midwife of our advanced civilization, but in the main a correct practice predominates, and the untutored savage, guided by instinct and observation, pursues the very course which is now considered the most advantageous and scientific among our leading obstetricians.
I cannot refrain from quoting some points from the excellent remarks of Playfair upon the management of the third stage of labor in order to show how well his teachings are borne out by the instinctive practice of the savage. He says: "There is unquestionably no period of labor where skilled management is more important, and none in which mistakes are more frequently made.... The general practice as to the management of this stage is opposed to the natural mechanism of placental expulsion, and is far from being well adapted to secure the important advantages which we ought to have in view.'' The objections he makes to the ordinary practice are: "That it inculcates the common error of relying on the binder as a means of promoting uterine contraction, advising its application before the expulsion of the placenta; that it teaches that traction on the cord should be used as a means of withdrawing the placenta, whereas the uterus itself should be made to expel the afterbirth. This may seem an exaggerated statement to those who have accustomed themselves to resort to the method of pulling on the placenta, but I feel confident that all who have learned the method of expression of the placenta would certify to its accuracy. The cardinal point to bear in mind is that the placenta should be expelled from the uterus by a vis a tergo, not drawn out by a vis a fronte.... The distinct enunciation of the doctrine that the placenta should be pressed and not drawn out of the uterus we owe to Credé and other German writers, but it is only of late years that this practice has become at all common. Those who have not seen placental expression produced, find it difficult to understand that, in the great majority of cases, the uterus may be made to expel the placenta out of the vagina, but such is unquestionably the fact.'' Is this not the practice most commonly followed among our Indian tribes? And is not, in consequence of this method of treatment, the placenta, as a rule, rapidly expelled, and its retention a matter of very rare occurrence?
As a rule the patient retains the position in which the child is expelled, usually one most favorable for the use of the abdominal muscles, kneeling or squatting. Steady pressure is kept up upon the contracting uterine globe, and if its contractions cease, they are stimulated by massage, by a kneading, churning of the tumor, and aided by slight traction on the cord, the placenta is
| CHAPTER III. THE THIRD STAGE OF
LABOR. Labor Among Primitive Peoples | ||