| CHAPTER II.
POSTURE IN LABOR. Labor Among Primitive Peoples | ||
2. CHAPTER II.
POSTURE IN LABOR.
INTRODUCTION.
As it was this feature to which my attention was first attracted, I will ask the indulgence of the reader for a few brief introductory remarks, explanatory of the manner in which this entire subject, novel at the time, but now rapidly gaining in interest and popularity, was developed.
IT was my good fortune in 1877 to add a valuable collection of ancient Peruvian pottery to my archeological museum. At the same time, whilst interested in these matters, I was told of an urn or vessel brought from the ancient graves of Peru, which represented a midwife delivering a woman in labor, and was then stowed away in the home of its discoverer, Dr. Coates, of Chester, Penn. My interest was at once aroused and I wrote to the gentleman requesting a photograph or cast of this unique piece of pottery. I received no answer, but constantly bore the subject in mind, until, finally, upon my visit East in 1879, my esteemed friend, Dr. Albert H. Smith, of Philadelphia, enabled me, through the kind offices of Dr. Anna E. Broomall, to examine the specimen, which proved so intensely interesting to me that I determined to satisfy myself as to the correctness and the historic value of this group, and, moreover, to study the subject of posture in labor. This ancient Peruvian funeral urn, well characterized in the heliotype which accompanies this article, is one of the oldest distinct and well authenticated representations of a labor case which is extant. The method of delivery followed by those, at that time, highly civilized people, a thousand or more years ago, seemed to me so peculiar that I was anxious to know whether other people had similar curious customs and whether any traces of these could be found at the present day; moreover, it appeared to me as if a study of obstetric customs among the more primitive people might lead to valuable results which
The next and most complete work on the subject was by Dr. H. H. Ploss,[4] "Ueber die Lage und Stellung der Frau wæhrend der Geburt bei verschiedenen Völkern.'' He, without entering upon a theoretical discussion of the question, gives us the results of his very thorough study of the positions occupied by women in labor among the ancients and among the uncultured and savage races of the present day. He recognizes the positions assumed as: Firstly, recumbent in a more or less horizontal position. Secondly, sitting: (a.) in bed; (b.) on a stool; (c.) on a chair; (d.) on a cushion; (e.) on the thighs of another individual. Thirdly, standing. Fourthly, kneeling. Fifthly, squatting. Sixthly, swinging. Seventhly, suspended in an erect posture. I shall not infrequently refer to the authorities quoted by Dr.
I might add that in 1870, a paper appeared in Breslau, by H. v. Ludwig,[5] in which the author, upon theoretical grounds, advocates the kneeling or squatting positions to be assumed during the expulsion of the child, and insists that the women of savage races, of people who still exist under the most natural conditions, instinctively assume these positions. As soon as my attention had been once directed to this subject by that remarkable funeral urn, representing the custom of the ancient Peruvians, and I had entered upon the study of the posture occupied during labor by the women of other people, I found a great variety in their customs; but it soon became evident, and impressed itself forcibly upon my mind, that the recumbent position in labor is rarely assumed among those people who live naturally and are, as yet, governed by their instincts and have escaped the influence of civilization and of modern obstetrics. It certainly appeared as if the ordinary obstetric position of to-day must be an unnatural one, and in order to study the question as to what is the natural position of women in labor, the proper and only course to be followed seemed to me to investigate:—
1. The position occupied by women in labor among the
2. To observe the position assumed by women in labor among savage races of the present day whose movements are still governed by instinct.
I deem it a great mistake that we in this age of culture, should follow custom or fashion so completely, to the exclusion of reason and instinct, in a mechanical act which so nearly concerns our animal nature as the delivery of the pregnant female. If we wish to obtain an idea of the natural position we must look to the woman who is governed by instinct, not by prudery; and it is only among the savage races that we shall find her at the present day. In this purely animal function instinct will guide the woman more correctly than the varying customs of the times.
3. In our obstetric practice of to-day to observe the movements of women and the positions which they involuntarily assume in the agony of the expulsive pains when instinct comes forward, to the exclusion of every other feeling. I have accordingly—
1. Sought such information as history could give me— as could be afforded by our larger libraries, especially that of the Surgeon-general's office in Washington; and I have made free use of the references given by Ploss in his work already referred to, and by Goodell,[6] in his instructive paper on "Some Ancient Methods of Delivery.''
2. In order to obtain information as to the positions assumed by those people among whom no modern obstetric law or custom as yet prevails—among the savages of the present day—I have corresponded with leading obstetricians in foreign countries, as well as travelers who were likely to assist me in this inquiry. I have sought information from physicians in various portions of our own country, partly by correspondence, partly by questions kindly put to their readers, by a number of our medical journals. The most valuable information, however, I have obtained through circulars sent to the medical officers of the army and the
3. I have made it my duty to observe the positions assumed by women at the very moment of the expulsion, during the agony of the last pains.
The subject will be divided as follows:—
THE INTRODUCTION.
PART I., treating of the position of women among people whose labor is governed by instinct and not by prudery or the laws of obstetrics.
PART II. The position of women among civilized races of the present day, in the agony of the expulsive pains.
CONCLUSIONS; and these, I will briefly state, are: that the semi-recumbent and inclined positions are the correct ones for the parturient woman,—anatomically, theoretically, and practically,—and that we have unquestionable ethnological proof of this assertion. We must resume the semi-recumbent position, and it becomes a question whether we should return to the obstetric chair or not.
I have classified the positions, according to the inclination of the axis of the body, into: The perpendicular or upright, the inclined, and the horizontal or recumbent.
A. Perpendicular:—
1. Standing.
2. Partially suspended.
3. Suspended.
B. Inclined:—
1. Sitting erect on stool, cushion, or stone.
2. Squatting, as in defecation.
3. Kneeling.
(a.) With the body inclined forward, and resting on a chair or staff.
(b.) Knee-elbow position, knee-breast, or knees and hands.
(c.) With the body erect or inclined backwards.
(d.) Not definitely described.
4. Semi-recumbent.
(a.) Sitting semi-recumbent on the ground, a stone, or stool.
(b.) On the lap or between the thighs of an assistant who is seated on a chair or on the floor.
(c.) The obstetric chair.
(d.) Semi-recumbent positions, strictly speaking.
C. Horizontal or recumbent.
(a.) On the back.
(b.) On the side.
(c.) On the chest and stomach.
I have been aided in this work by so many kind friends and fellow practitioners that I feel it my duty to express my thanks to, at least, some of them, for the valuable assistance rendered. Dr. Isaac Coates, formerly of Chester, Penn., gave the impulse to this undertaking by kindly permitting me to photograph the historic urn which he unearthed from its resting place, that it might reveal to us the life of a people long since passed away; and it is owing to the efforts of Dr. Anna E. Broomall that I was actually enabled to do this. The kindness of Drs. Billings and Fletcher readily enabled me to obtain much important information from the vast and well catalogued materials of the Surgeon-general's library. To Dr. H. C. Yarrow my especial thanks are due for his unceasing efforts in the interest of this undertaking; his position and his researches in the library of the Surgeon-general's office enabled him to extend to me many favors; with the consent and at the direction of Major J. W. Powell, in charge of the Bureau of Ethnology of the Smithsonian Institution, aided by other friends, he has sent out a series of circulars to the surgeons of the army and Indian Agencies requesting information as to the obstetric practices among our North American Indians; I also gratefully acknowledge my indebtedness to the medical officers of the United States army, and the physicians to the Indian Agencies, for the valuable information given, and their cheerful and generous response to the circular sent. Dr. Raoul Fauquez, of Paris, had the kindness to offer information upon the subject in the various departments of France. Several of our medical journals placed before their readers
Quite a number of the instructive illustrations I owe to the genius of St. Louis' talented artist, Mr. Carl Gutherz whilst Dr. H. H. Ploss, of Leipzig, has permitted the use of several of the cuts from his own work.
GEOGRAPHICAL DISTRIBUTION.
Europe.
The dorsal decubitus, with the woman recumbent in bed, is now almost universal, having superseded the obstetric chair of the beginning of this century. Peculiar positions are still found here and there in remote districts.
France. A standing position is occasionally assumed.
Italy. Semi-recumbent on the lap; and in earlier days knee-elbow, semi-recumbent in bed, and erect, clinging to the neck of an assistant.
Spain. Kneeling.
Germany. Standing; on the lap of an assistant; partly suspended; semi-recumbent in bed, or in a sling.
Russia. Erect, wholly suspended; squatting; kneeling; sitting erect and in the lap of an assistant.
Sweden. Recumbent.
Greece. Kneeling and semi-recumbent in bed, or on a low stool reclining against an assistant, in ancient Greece. In later times, recumbent in bed, or semi-recumbent on a low stool, reclining against an assistant, which appears still very common.
Turkey. Chair; sitting on a stool.
Great Britain. Clinging to the neck of an assistant; kneeling, arms resting on a chair or in the lap of an assistant; knee-elbow position; sitting on a low stool; squatting; sitting semi-recumbent in the lap of an assistant (several of these positions have been frequently observed in Irish or Welsh emigrants in this country).
Kamtschatka. Kneeling.
Mongolia. Kneeling.
China. Chair or bed.
Japan. Chair, semi-recumbent, or kneeling erect on the floor.
Philippine Islands. Standing.
Sumatra. Recumbent.
Siam. Recumbent; lying on the side or back.
Burmah. Recumbent, on the back.
India. Standing; on the lap; sitting on a cushion or stool; recumbent in bed.
Andaman Islands. In the lap of the husband.
Persia. Squatting or kneeling.
Arabia. Squatting; semi-recumbent on the chair or the lap; or on two flat stones clinging to a rope.
Palestine. Chair.
Syria. Rocking-chair; semi-recumbent.
Hebrews. Semi-recumbent (on stones or a stool) and squatting.
Cyprus. Semi-recumbent on a stool (ancient and modern). Africa.
Egypt, ancient. Squatting.
Egypt, modern. Chair.
Abyssinia. Kneeling; sitting on a stone, reclining against an assistant or a tree.
Ethiopia. Kneeling; standing.
Dar-Fur. Standing.
East Africa. Standing; sitting or squatting.
Somali. Standing, holding on to a rope.
Wakamba. Standing, bent over backwards.
Kaffraria. Squatting.
Hottentots, Cape of Good Hope. Standing.
Old Calabar. Sitting on a chair or block.
Wazegua. Squatting.
Canary Islands. Sitting erect. North America.
Canada, French settlers. Semi-recumbent on the floor, back against an inclined chair.
Canada, Iroquois. Standing, clinging to the neck.
Mexico, Indians, half-breeds, and lower class of whites. Kneeling, clinging to a rope or the neck; squatting; standing, and semi-recumbent on the lap and in bed.
United States, Caucasians descended from various European races. Kneeling; squatting; sitting on the husband's lap; semi-recumbent
United States, Negroes. Kneeling, head in the lap; squatting; suspended from the limb of a tree.
United States, Indians. Mostly kneeling, clinging to a tent-pole, the body inclined forward, or to a rope or horizontal staff, the body inclined back; often squatting; occasionally sitting semi-recumbent in the lap or on the floor; semi-recumbent, or kneeling erect; more rarely recumbent; standing erect, clinging to the neck of an assistant; tied to a tree, or suspended; and the knee-chest position. Central and South America.
Nicaragua. Kneeling.
Guatemala. Squatting.
Venezuela. Semi-recumbent, seated in a hammock.
Peru, ancient and modern. Semi-recumbent in the husband's lap.
Chili. Semi-recumbent in the lap.
Brazil. Recumbent on the ground or in a hammock. Australia and Surrounding Islands.
Australia. Sitting erect; recumbent.
Ceram. Standing erect; suspended.
Polynesia. Squatting.
West Micronesia. Squatting.
New Zealand. Kneeling.
Sandwich Islands. Semi-recumbent on the lap, or lying on a mat.
1. PART I.
Position of Parturient women among People whose Parturition is governed by Instinct and not by Modern Obstetric Fashion.—Among the Ancients.—Among the Savage or Uncivilized Races of the present Day, and in Remote Districts of Civilized Countries.
I HAVE, as already stated, determined to classify the various positions, as nearly as possible, in accordance with the position assumed by the axis of the body, and shall hence consider first: A. The Perpendicular or Upright Positions; then B. The Inclined Positions; and finally C. The Horizontal or Recumbent Positions.
A. PERPENDICULAR OR UPRIGHT POSTURE.
Under this heading I shall discuss, individually, those positions in which the body is erect or almost so, and, in accordance with some slight variations, will distinguish: 1. The Standing, 2. The Partially Suspended, 3. The Entirely Suspended Positions.
1. STANDING.
We shall find this apparently uncomfortable position assumed even at the present day, and in our own country: Thus, Dr. H. F. Campbell, of Georgia, writes me that he has delivered a patient standing, clinging to the bed-post, who would rather dispense with his services than assume any other position. Among our Indians it is rarely observed, although I have been informed by a correspondent that the Sioux women are delivered standing erect; I think
The Hindoos, especially upon the eastern coast of India and in the vicinity of Madras, are delivered in an erect, standing posture, supported by an assistant under each shoulder—the midwife attending to her duties, being seated in front of the patient,[9] and whether rare or not at the present day the position is certainly traditionary, as bas-reliefs still exist upon the ancient Indian monuments which represent the act of delivery in this very same way.
In Central Africa, and near the Cape, among the Boers, the standing posture is not uncommon. Among the Negritos, upon the Philippine Islands, the parturient woman assumes the standing position, but apparently bent forward a little, as she supports the abdomen against a bamboo cane planted in the ground, thus apparently exercising some pressure upon the uterus.[10] Among the Wakambas, in Africa,
A similar position is shown in an old painting in the
Academy of Medicine in New York. (See Fig. 5.) The
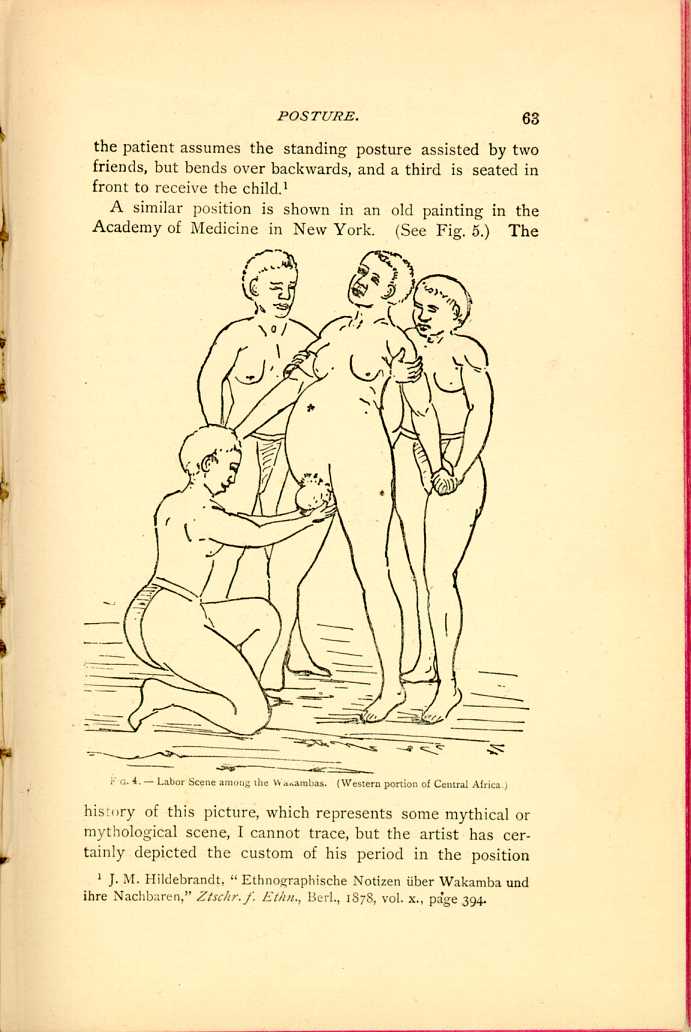
FIG. 4.—Labor Scene among the Wakambas.
(Western portion of Central Africa.)
[Description: Woman giving birth while standing upright, supported by two
friends. Another woman kneels before her to receive the child. Black
and white illustration.]
The Loangos, in Equatorial Africa, are delivered standing,
leaning against the wall of the hut, or kneeling, the
head resting upon the arms. The reason assigned for this
procedure is that they expect to obtain the desired head
presentation by assuming these positions. In difficult labor

FIG. 5.—Mythical Labor Scene.
[Description: Two women assist in delivering baby from a robed woman. Black
and white illustration.]
2. PARTIALLY SUSPENDED.
Parturient women endeavor to assume this position of partial suspension in various ways. Some hang to the neck
The women of the Iroquois
in Canada, are all
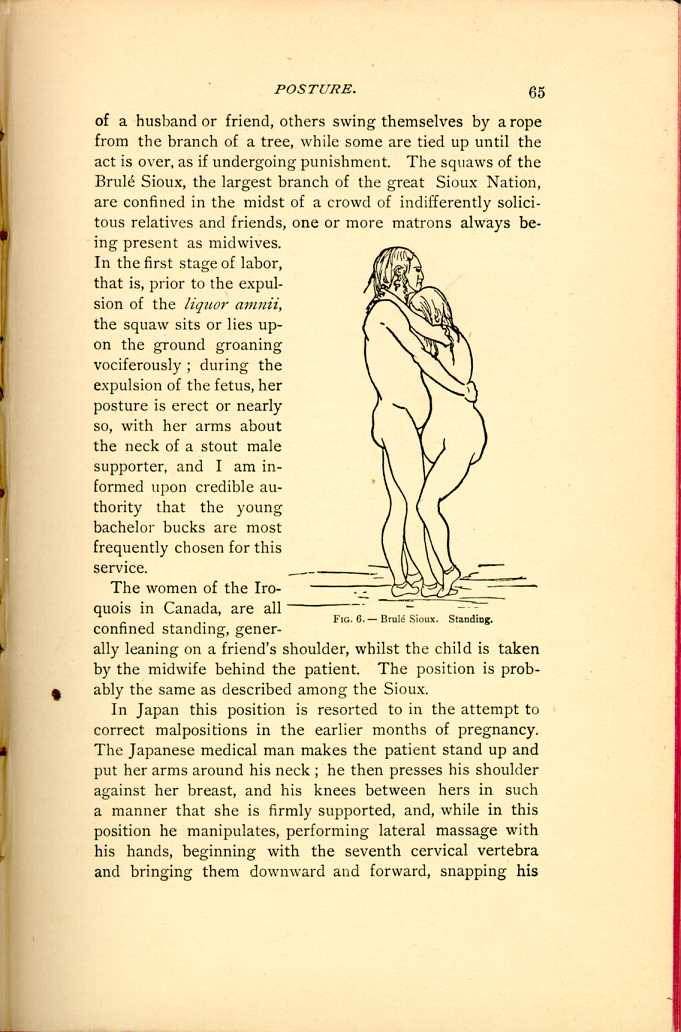
FIG. 6.—Brulé Sioux. Standing.
[Description: Pregnant woman stands, supported by a man. She faces him with
her arms around his neck. Black and white illustration.]
In Japan this position is resorted to in the attempt to correct malpositions in the earlier months of pregnancy. The Japanese medical man makes the patient stand up and put her arms around his neck; he then presses his shoulder against her breast, and his knees between hers in such a manner that she is firmly supported, and, while in this position he manipulates, performing lateral massage with his hands, beginning with the seventh cervical vertebra and bringing them downward and forward, snapping his
The "New York Medical Record'' adds, that the accoucheurs are, in Japan, as a rule, advanced in age. If this custom is found in our own country it certainly comes to us from some of the inland countries of Europe. Thus, Spence, in his "System of Midwifery,''[14] says that the position which is very frequently practiced in the northern portion of Scotland, is that of hanging about the neck of a person as tall, or, if possible, taller than herself, who gently supports the patient's back, and with her knees fixes the knees of the woman in labor. In Italy it was Savonarola, who died in Padua in 1460, who taught that in difficult labors the parturient woman should either hang to the neck of a stout person or assume the knee-elbow position.[15]
The practice in some Mexican families[16] is to keep the woman in an upright position, with the knees and thighs slightly flexed, the feet wide apart, while she supports herself by two ropes suspended from above. He adds that massage is very freely resorted to, but no binder is at any time used.
We find precisely the same position in Africa among several native tribes. Thus, the Somali women assume an erect posture, partially suspended by a rope during the expulsion of the child, which is received by a family attendant or midwife.[17] So, also, we find that the women of Dar Fur, on the Nile, are delivered standing, with the legs separated,[18] holding on to a rope.
A somewhat more barbarous custom is that followed by
some of our North American Indians, and by the inhabitants
of Ceram, an island north of Australia, namely: they
tie the patient to a post or tree, with the hands above the
head. The Coyoteros are in the habit of tying their
women, in labor, to a tree, with the hands above the head,
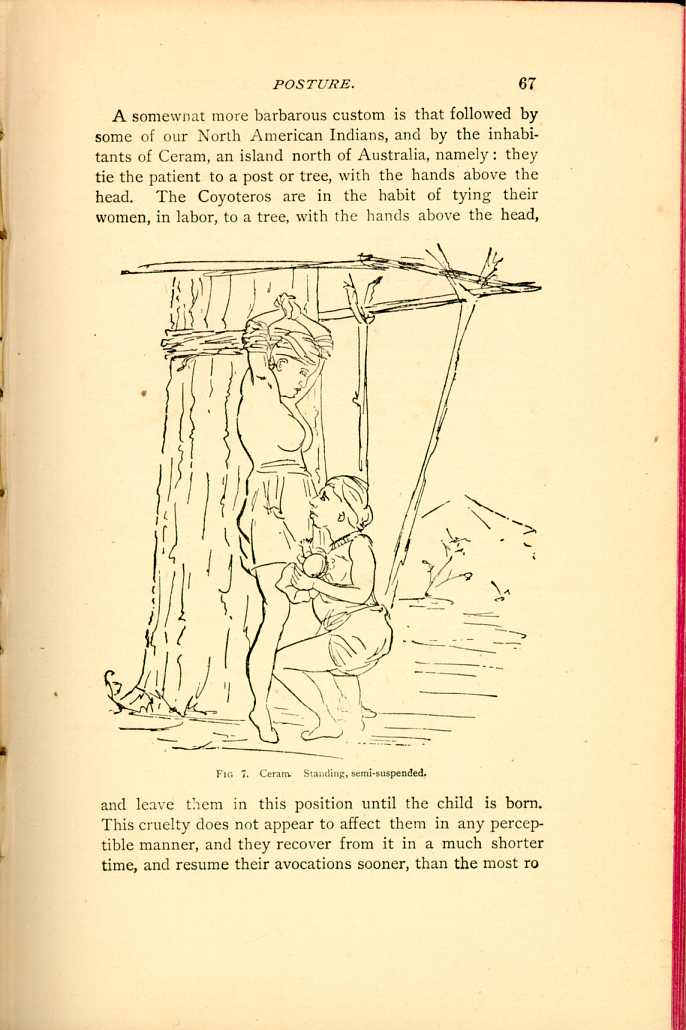
FIG 7. Ceram. Standing, semi-suspended.
[Description: Woman gives birth leaning against a tree, her arms bound above
her. Another woman squats before her to assist delivery. Black and
white illustration.]
3. SUSPENDED.
Not unfrequently the negroes in our southern States still follow the customs brought from their African homes, or merely handed down by tradition; in their method of delivery they do not vary from that of the tribe from which they sprang. Occasionally the erect posture is taken, and a graphic description of such a labor has been given me, as witnessed in Louisiana. A negress gave birth to a child while hanging on to the limb of a tree. She would raise herself from the ground during the pains, whilst the assistant who was with her took charge of the child after it was born.[21]
In some portions of Finland, among the Esthen, as well as in some portions of Russia, the women are delivered in a similar manner while hanging to a cross-bar; they attempt, as it were, to shake out the child.[22]
We have the authority of Father Och that, in Brazil, the parturient woman occasionally has her arms tied to a tree while she is waited on by some old hags until the delivery is completed.[23]
In some portions of Germany, though the instances are
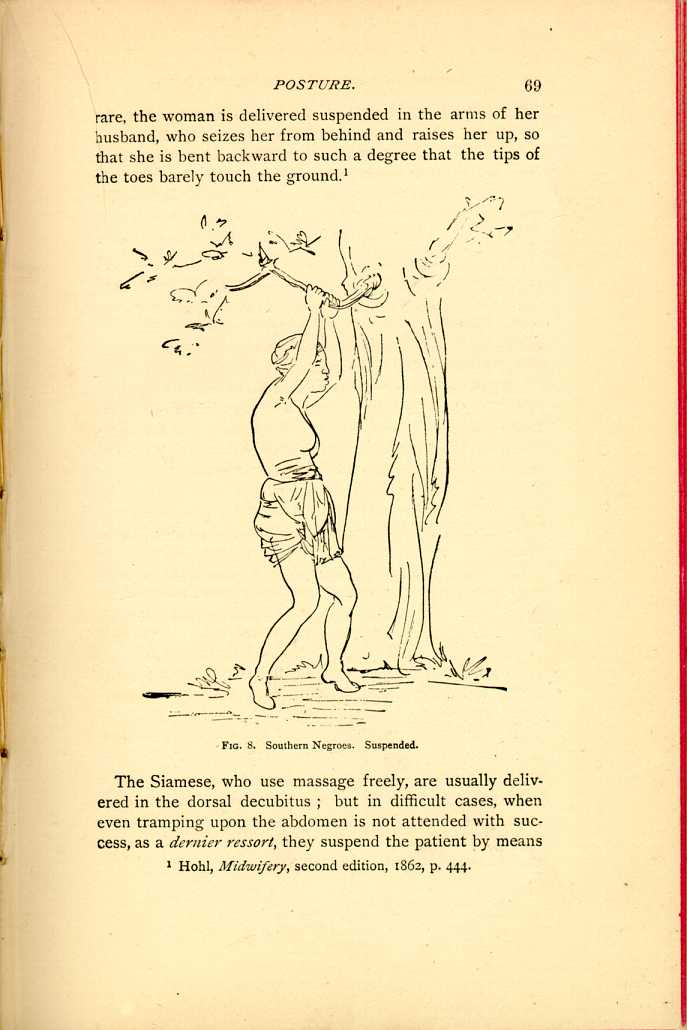
FIG. 8. Southern Negroes. Suspended.
[Description: Pregnant woman hangs by her hands from a tree branch. Black and white illustration.]The Siamese, who use massage freely, are usually delivered in the dorsal decubitus; but in difficult cases, when even tramping upon the abdomen is not attended with success, as a dernier ressort, they suspend the patient by means
B. INCLINED POSITIONS.
This class, which we shall find, by far, the most common among civilized and savage people, ancient and modern, I have divided into four kinds, though the first one may not, perhaps, with the greatest propriety, be called an inclined position.
1. The erect, sitting posture.
2. The squatting position, as in defecation
3. The kneeling posture and its modifications; and finally,—
4. The semi-recumbent position, whether on the lap of an assistant, in a chair, on the floor, or in bed.
1. SITTING ERECT.
I hardly know whether to consider the erect sitting posture as an inclined or an upright position, but, as the pelvic axis is certainly more inclined than in the standing posture, and, as it will be very hard to draw a line between the distinctly erect sitting posture and the somewhat inclined, I have determined to place it among the inclined, and to consider it first under this head, because it is most nearly related to the perpendicular or upright. Women confined in this position make use of cushions, stones, stools, or mother earth herself; but the temptation to assume a somewhat reclining position, leaning against the assistant or some other support, is so great, that it is difficult to say with precision that the erect sitting posture is assumed, as the notes upon the subject, by most writers, are not sufficiently clear. I can find but one distinct description of a labor in which it is stated that the patient was confined sitting upright, and that this is the usual position among native
The Nayer women, of Malabar, are confined while seated upon a cushion, or a low three-legged stool without a back, and are supported by the midwife, or some female relative. As is so common among savage races, they then bathe in the nearest stream, or other convenient water, immediately after delivery, and resume their work, as far as is permissible, in the state of uncleanliness in which they are considered to be after labor.[26]
In a similar way the native woman of Guatemala, South America, is confined. She is seated on the ground, supported by a midwife, who presses one knee into the small of her back.[27]
In Calabar, Africa, the same position is assumed, the woman sitting on a low chair, or block, while the midwife squats in front of her, pressing the sides of the abdomen.[28]
On the Canary Islands, the parturient woman sits upon the floor, with a chair or other support beside her, upon which her arms rest. In Astrakhan, in Russia, she sits in a similar way between two boxes or trunks, upon which her arms rest.[29]
A sitting position, with the body decidedly bent forward, was observed in a Sioux squaw, who, like her sisters among most of the Indian tribes, sought a solitary confinement upon the banks of a stream.[30] The position of this woman, until the expulsion of the child,—about forty minutes,— was cross-legged on the floor, her arms crossed over her breast, head bowed, and the body bent forward, especially
2. SQUATTING.
This position naturally
follows the erect sitting
posture, although the
body is always inclined
forward to a certain degree;
it is hardly to be
defined with exactness,
yet we may, in a general
way, consider all postures
as squatting which
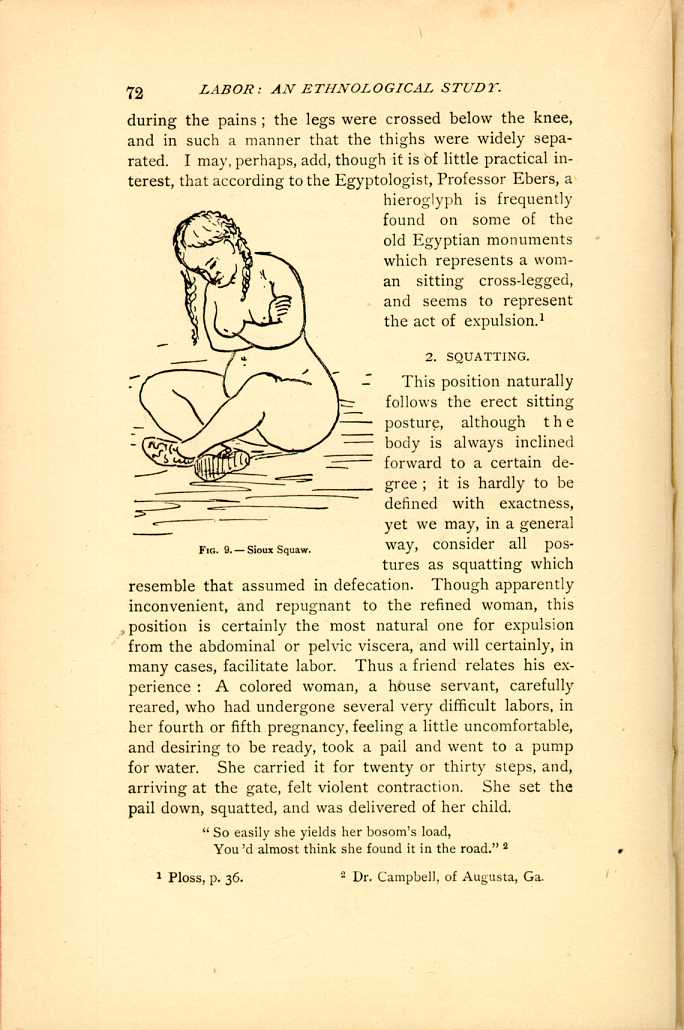
FIG. 9.—Sioux Squaw.
[Description: Pregnant woman sits cross-legged. Black and white
illustration.]
"So easily she yields her bosom's load
You'd almost think she found it in the road.''[32]
Then, again, he tells me of attending a lady of good position in society in two labors. "In her first labor, delivery was retarded without apparent cause. There was nothing like impaction, or inertia, yet the head did not advance. At every pain she made violent efforts, and would bring her chest forward. I had determined to use the forceps, but just then, in one of the violent pains, she raised herself up in bed and assumed a squatting position, when the most magic effect was produced. It seemed to aid in completing delivery in the most remarkable manner, as the head advanced rapidly, and she soon expelled the child by what appeared to be one prolonged attack of pain. In subsequent parturition, labor appeared extremely painful and retarded in the same manner; I allowed her to take the same position, as I had remembered her former labor, and she was delivered at once, squatting.''
The Irish, also, are familiar with this most natural of all positions, although the knee-elbow position is more common among them. A striking instance is related to me of a poor Irish woman who was found upon a vacant lot in New York city, squatting upon the ground, endeavoring to express the placenta, the child having already been delivered in the same position.[33]
Dr. John Williams, physician to the Green Bay Indian Agency, seems to consider with great favor this position as assumed by the Pawnee Indians. He has had extensive experience as Agency physician, having been associated with different tribes of Indians in different localities, and he does not think that climate has anything to do with the labor of the parturient woman. He says: "I am satisfied that the Pawnee Indian women are far more exempt from the maladies resulting from parturition than the Menemonee, Stockbridge, or Oneidas of Wisconsin. Possibly this may be attributed to the position assumed during labor. The position of the Pawnee woman in parturition is generally
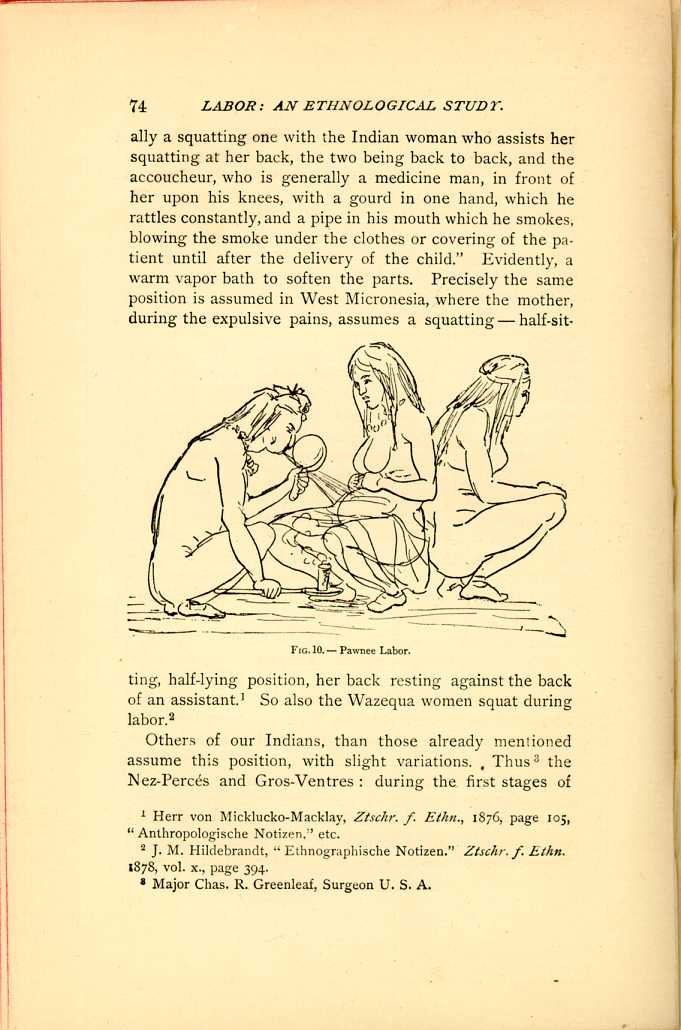
FIG. 10.—Pawnee Labor.
[Description: Medicine man rattles gourd and blows pipe smoke towards abdomen of squatting pregnant woman. Another woman squats nearby. Black and white illustration.]Others of our Indians, than those already mentioned assume this position, with slight variations. Thus[36] the Nez-Percés and Gros-Ventres: during the first stages of
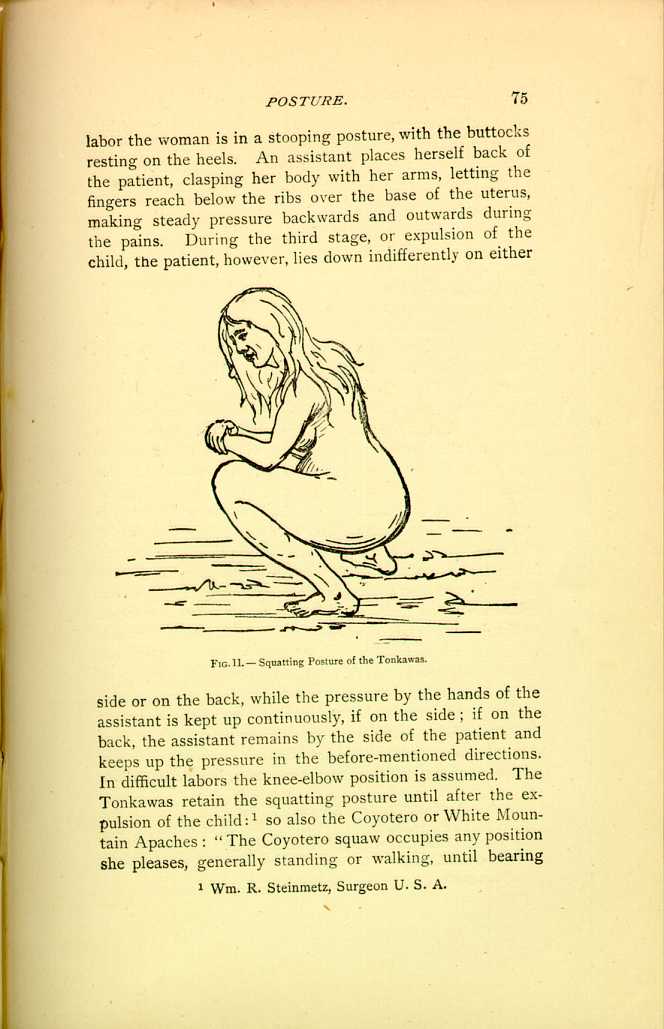
FIG. 11.—Squatting Posture of the Tonkawas.
[Description: Pregnant woman in squatting position. Black and white illustration.]A slight variation of this position is found among some of the larger branches of the Sioux Nation, the Brulé, Loafer, Ogallala, Wazahzah, and Northern, who stoop, and with their hands grasp deer-thongs attached to stakes driven into the ground, against which they pull.[39]
The Mexican half-breeds, in New Mexico and vicinity, sometimes suspend a cord from the ceiling, with a stick attached, so that the women can seize it in a half-upright, squatting position.[40] The same we find among the Kalmucks upon the borders of China and Russia, and not unfrequently during the third stage of labor they squat lower in bed on their heels, whilst holding with their hands on to a pole, the abdomen being pressed from behind by an assistant.[41]
The squatting position, with the body bent forward, is assumed by the women of Southern Arabia in the vicinity of Aden, who, however, rest their hands upon the ground instead of crossing them upon the breast, as the squaw does. But, among these people, as among so many of our Indians, and the tribes of Africa, massage is freely resorted to if any obstruction seems to prevent the labor, sometimes with the hands, sometimes with the feet; in the latter case, the assistant, standing with her heels upon the lower ribs, works the fundus of the uterus with her toes.[42]
Every people varies its customs a little. The Polynesian and Australian negresses squat, as in defecation, over a small hole which they have scratched in the ground for the reception of the child.[43] Ploss also states, upon the authority
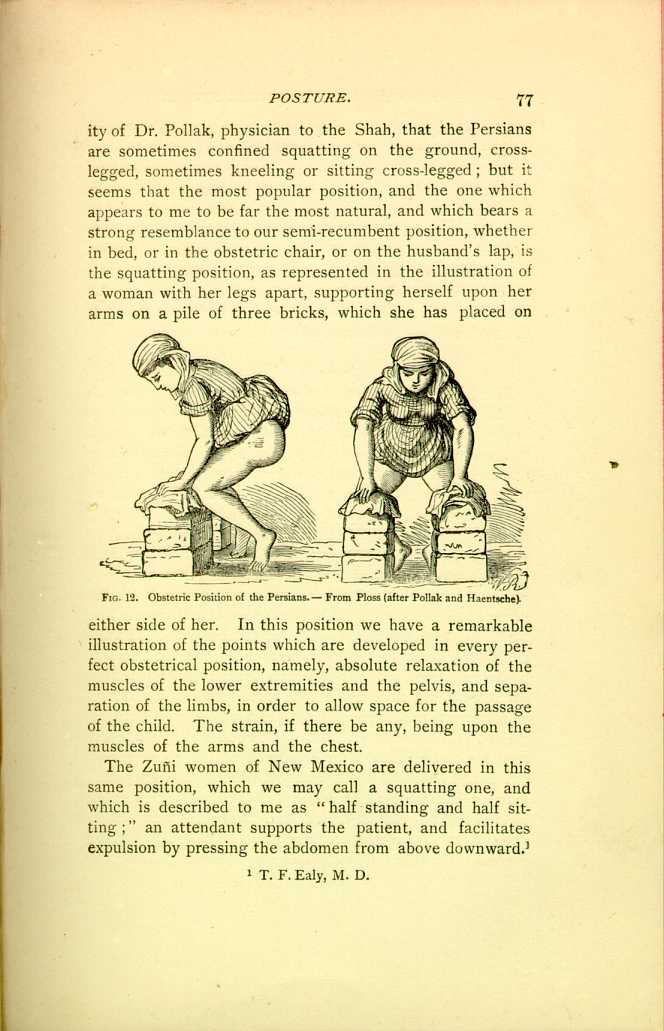
FIG. 12. Obstetric Position of the Persians.—From Ploss (after Pollak and Haentsche).
[Description: Front and side view of a pregnant woman supporting herself in a squatting position by placing her hands of stacks of bricks on either side of her. Black and white illustration.]The Zuñi women of New Mexico are delivered in this same position, which we may call a squatting one, and which is described to me as "half standing and half sitting;'' an attendant supports the patient, and facilitates expulsion by pressing the abdomen from above downward.[44]
In the neighboring Laguna Pueblo pretty much the same custom is followed. In the early stages of labor the patient stands, as she urinates, with her hands on her knees; later, she stands up, supported by a woman on each side, or a rope is cast over a joist of the roof and allowed to hang down in a wide loop; she puts her breast in the loop and holds on to the ascending ropes, her feet on the floor, in a half-sitting (squatting) posture, thus obtaining great expulsive force; if tired and worn, she lies down. All these positions are assumed at the choice of the patient or the advice of her assistants, two to six in number.[45]
3. KNEELING.
The kneeling posture, like some other positions which appear to us peculiar, is a historical one. It is referred to in the Bible, as well as by the Roman poets. It was taught in ancient Rome, among the Arabs, and in Germany during the Middle Ages, and definite rules were laid down for the circumstances under which it should be resorted to. At this present day it is still, at times, adopted in the rural districts of our own States, and more frequently than we should suppose in our cities. It is that position which is, perhaps, most universal among our Indians, that is, among what we may call the blanket Indians, those who have not yet partially succumbed to the advances of eastern civilization. Some of our ablest obstetricians, Fellows of this Society, who have given me their opinions upon the kneeling posture in labor, differ in their views in regard to its advantages and disadvantages; to one it seems physiologically correct, and appears most practically to favor the expulsion of the child, whilst it is frowned upon by another as liable to be followed by hemorrhage. We, however, do not hear of this as a frequent occurrence among the Indians, where the position is so common; in fact, we neither hear of this nor any other accident consequent upon labor, not even of prolapse, which might be supposed to follow; probably, because the position is only assumed during the
If I may make a broad assertion, the kneeling posture seems most common among the red and yellow races; our Indians mainly being delivered kneeling, with the body inclined forward; whilst the Mongolians seem, as a rule, to retain the body more erect. I have classified the kneeling positions as follows:—
(a.) The body inclined forward.
(b.) This position overdone; that is, with the body thrown
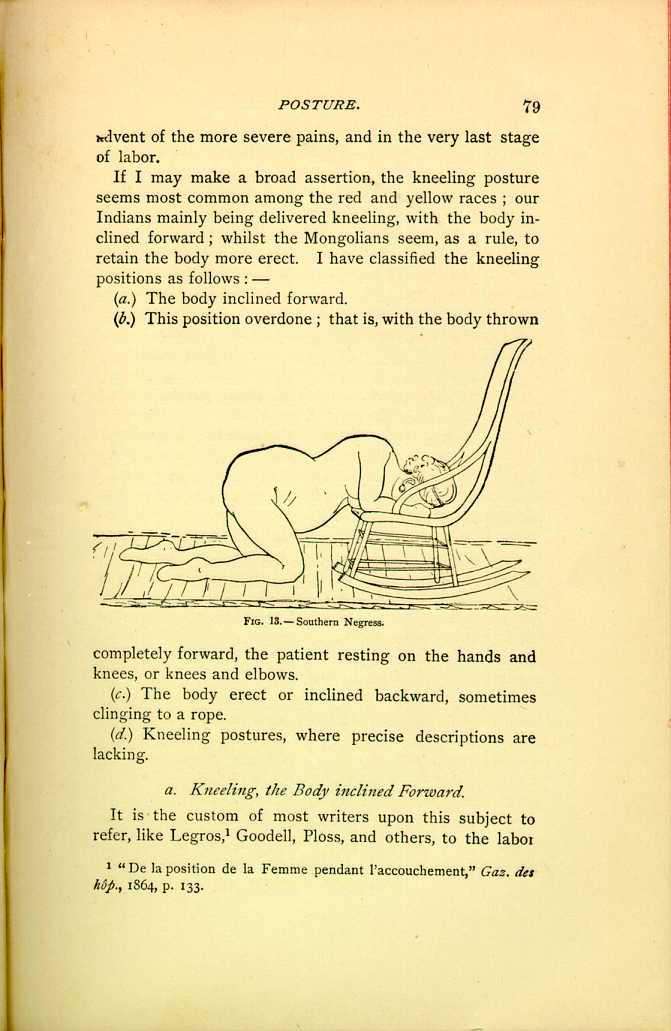
FIG. 13.—Southern Negress.
[Description: Pregnant woman kneels on the floor,
her face and arms resting in the seat of
a rocking chair. Black and white illustration.]
(c.) The body erect or inclined backward, sometimes clinging to a rope.
(d.) Kneeling postures, where precise descriptions are lacking.
a. Kneeling, the Body inclined Forward.
It is the custom of most writers upon this subject to refer, like Legros,[46] Goodell, Ploss, and others, to the labor
In a previous labor she had been confined in a similar position, resting head and arms in the lap of her mistress; precisely the same position which the squaws of the Umpgua tribe, in Oregon, are in the habit of assuming. Let us look in upon a scene of this kind.
The patient was found in a lodge, roughly constructed of lumber and drift-wood; the place was packed to suffocation with men and women, the stifling odor from sweat and smoke and stench of whale oil, rendered the lodge unendurable for more than a few moments together. The parturient, situated in the centre of the place, was entirely naked excepting a covering by a dirty blanket, which was thrown across her loins. Her head and shoulders were supported in the lap of an old squaw, while her thighs were stoutly pressed against the pelvis by a squaw on each side, who were engaged in crowding the uterus downward in a brutal manner with their clenched fists, occasionally giving it a lateral motion; another squaw sat between her knees, with her hands under the blanket, ready to receive the child when it came. The crowd in the lodge all the while kept up a deafening din by crying, shouting, pounding on tin vessels, and thumping up against the roof with poles,
Many of the Indian tribes follow this custom, the parturient woman assuming a kneeling position, head and arms resting in the lap of an attendant, or upon any convenient support: a stump, box, bed, or chair; so the tribes of the Quapaw Agency, the Peorias, Shawnees, Wyandots, Ottawas, and Senecas.[49]
The Indians of the Cattarangus Reservation are delivered in the same way, assuming this position just before the expulsion of the child, whilst in the earlier stages they sit or walk about as they please.[50] So, also, the Klatsops of northwestern Oregon, who, however, retain the body more erect, as a young woman assistant stands behind the parturient and clasps her under the arms and around the breast, supporting the patient and forcibly holding her up.[51]
The whites equally resort to this position; thus I hear of its observance in the western and southwestern portions of Missouri. Dr. Willis P. King, of Sedalia, writes me that he has found quite a number of cases where the women desired, during the last part of the second stage, to get up and kneel by a chair; and he says that all the women who have been in the habit of being delivered in this way were Pennsylvanians, of the Pennsylvania German stock, or, at least, that the suggestion had come from a Pennsylvania woman. Since he has seen a woman flood almost to syncope after delivery in this position, he condemns it severely.
I am a little astonished to see this position mentioned as originating in this country among the Pennsylvania Germans, because the only reference that I can find to the kneeling posture among the Germans (and we cannot in reality call the Fins Germans) is by Holst,[52] who says that the Esthen, in difficult cases, seek to hasten delivery by assuming
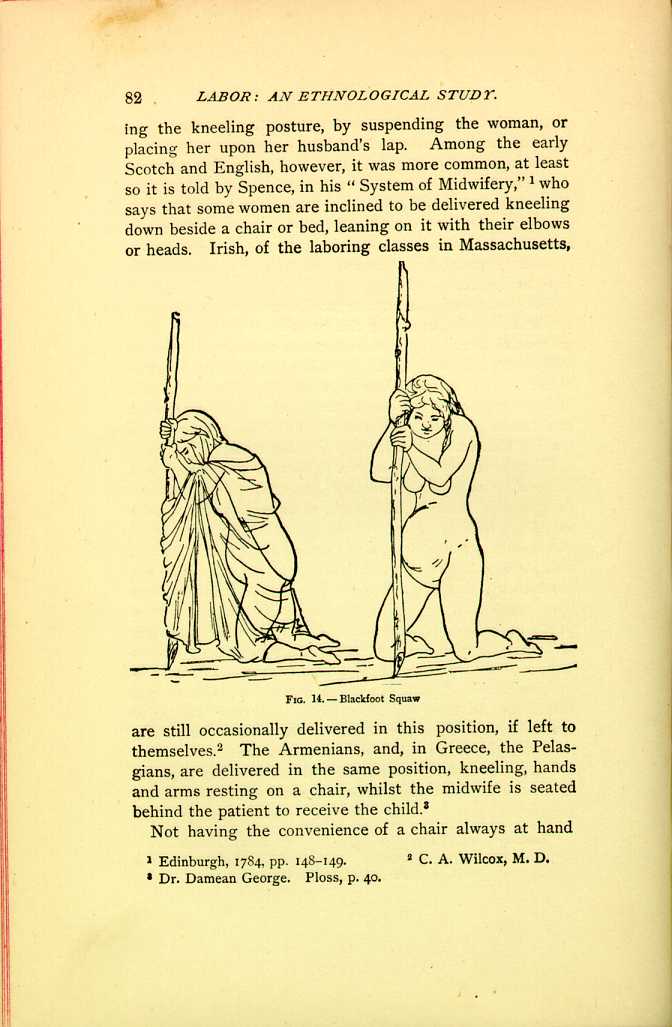
FIG. 14.—Blackfoot Squaw
[Description: Two pregnant women kneel, each supporting herself with a pole planted before her. Black and white illustration.]Not having the convenience of a chair always at hand
The same custom is observed among the Comanches and the Indians of the Uintah Valley, who, however, are not confined in their té-pee but in a temporary enclosure near by. The accompanying cut represents a Comanche squaw in labor, and in order that it may be fully understood I will give some of the details of this accouchement from the extremely interesting description of Major W. H. Forwood, Surgeon U. S. A., who was in attendance and kindly furnished the sketch: "A short distance outside the camp, and in the rear of the patient's family lodge, a shelter had been constructed of green boughs, six or seven feet high, by making holes in the hard ground with a wooden peg, and setting up brush or bushes, with the leaves on, around the circumference of a circle about eight feet in diameter. An
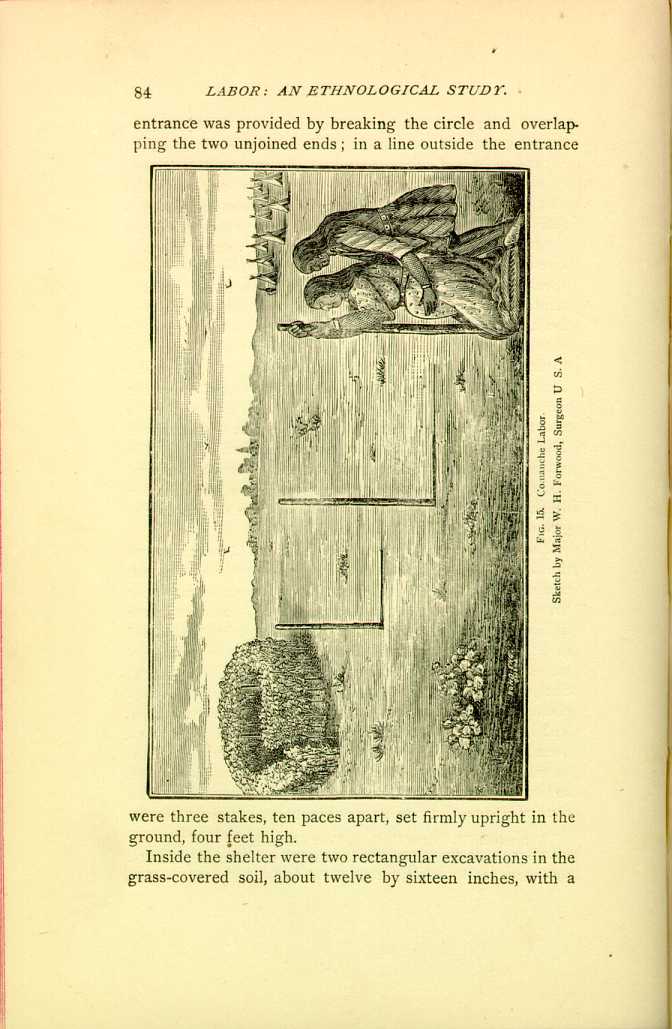
FIG. 15. Comanche Labor Sketch by Major W. H. Forwood, Surgeon U. S. A.
[Description: Pregnant woman kneels, supporting herself with stake planted before her, while another person stands behind her and presses against the sides of her abdomen. Circular brush shelter is nearby. Black and white illustration.]Inside the shelter were two rectangular excavations in the grass-covered soil, about twelve by sixteen inches, with a
I found my patient walking with her assistant, a female relative, up and down the line of stakes outside the shelter, stooping now and then to kneel at the nearest stake and grasping it with both hands during a pain; most of her time was spent in this way, outside the enclosure; occasionally she would enter to kneel over the hot stones or loose earth. During each pain she knelt down close to one of the stakes, bringing the front of her feet and legs against the ground and her knees a little apart, the body bent forward, face turned down, or sometimes up, at the severest part of the pain, and the hands, one above the other, grasping the stake on about a level with the head. The assistant stood behind, astride of or between the patient's feet, and stooping over, passed her arms around the body until her hands were brought over the front and lower part of the patient's abdomen; in this position she performed several manipulations with the palms of her hands and fingers, while the pain lasted, such as rubbing, kneading, etc., but most frequently a quick jerking or shaking upward movement, something like that of shaking a pillow into its case. The patient never assumed a recumbent position, and the moment the placenta escaped she sprang up, buckled on a stout leather belt, mingled with the crowd and soon disappeared, without apparently taking the slightest notice of her child.''
The Indians of the Uintah Valley Agency, Utah, observe the same customs with this exception, that they keep a kettle of hot water, boiling, within the enclosure or "Wick-e-up,'' of which the patient takes frequent and copious draughts during the labor, and as soon as the child is expelled she continues drinking freely of the hot water, rises to her feet, places a folded cloth to her abdomen, and
The natives of New Zealand kneel down upon a mat, the knees about two feet apart, the hands resting on a tree or stick, or clutching some hard substance, while if help is needed, the arms are twined about the knees of an assistant in order to press them against the fundus of the womb.[59]
The Dakota woman assumes a kneeling position during labor, unless extreme weakness prevents; she supports herself by a post driven into the ground, or any convenient means of support; the recumbent position, they think, retards the progress of labor.[60]
The rather vague information to be obtained from the Cheyennes, Arapahoes, and Eastern Apaches was to the effect that the parturient woman, as among so many of the Indian tribes, retires to the bush, where, if the labor is a normal one, she is delivered without any assistance, the position assumed being upon her knees, occasionally a reclining one. Dr. C. P. Allen writes me concerning the Chippewas, from the White Earth Indian Agency, that, if the parturient is of the wild or blanket Indians, a quantity of dry grass is spread on the ground in the té-pee, or house, if they have any; a pole six to ten feet long and three to four inches in diameter is placed on the backs of chairs or fixed across one corner of the room about the height of a chair, behind which, with it across her chest, the woman rests on her knees during the pains, sitting down in the interval. Those who are partly civilized assume a somewhat similar position but use straw overlaid by quilts or blankets.
I would here call attention to the fact that the Chippewa woman seems to draw horizontally upon this cross-bar and
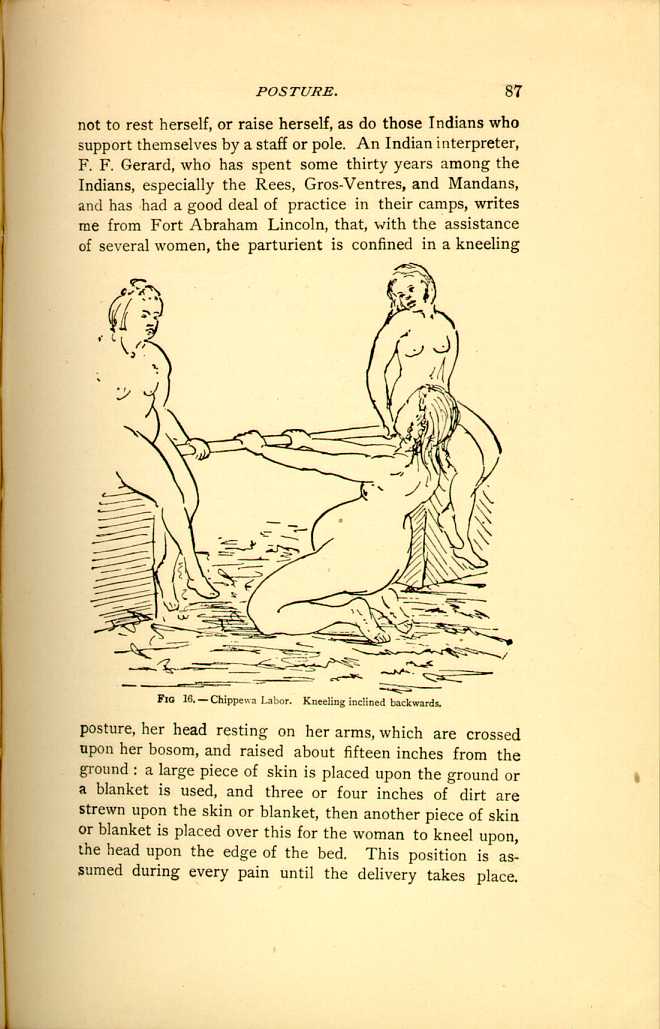
FIG 16.—Chippewa Labor. Kneeling inclined backwards.
[Description: Pregnant woman kneels and leans backward, grasping a horizontal pole held between two other woman. Black and white illustration.]From a very instructive letter, recently received from
Dr. N. Kauda, of Tokio, I see that the Japanese are not
unfrequently delivered in a kneeling posture; the description
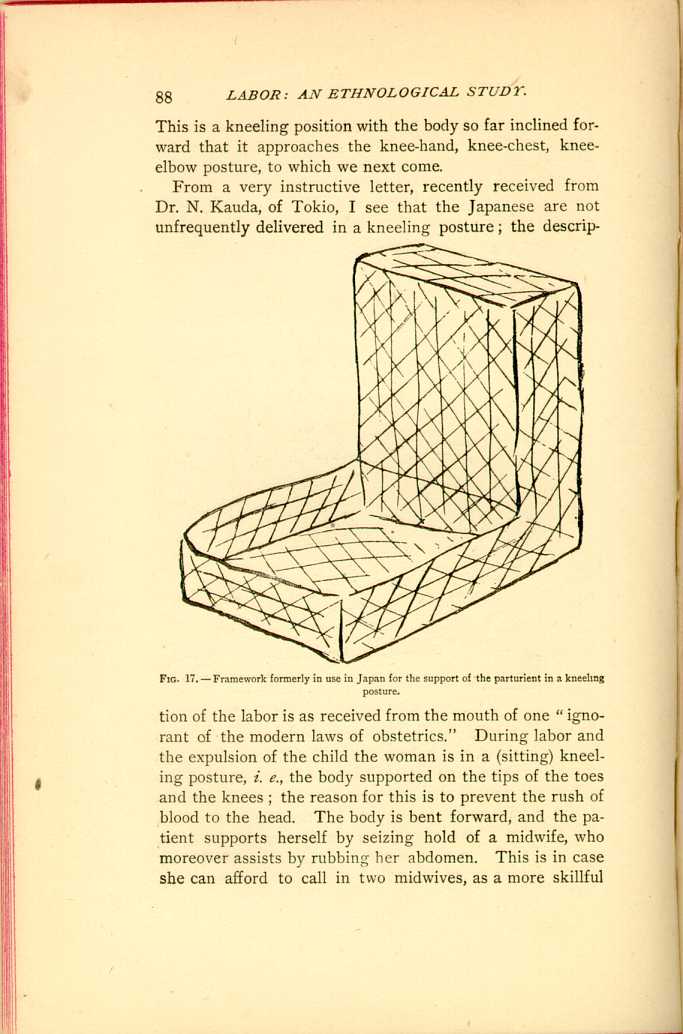
FIG. 17.—Framework formerly in use in Japan for the support
of the parturient in a kneeling posture.
[Description: Piece of furniture shaped like a chair
without legs, designed to support a woman in a kneeling posture. Black
and white illustration.]
Fifty years ago the patient was supported in her position
and the labor conducted in a framework (Fig. 17), but
now ordinary articles of bedding are piled up to support
the back (Fig. 18), as seen in the figure which represents
the posture just after delivery, and in this upright position
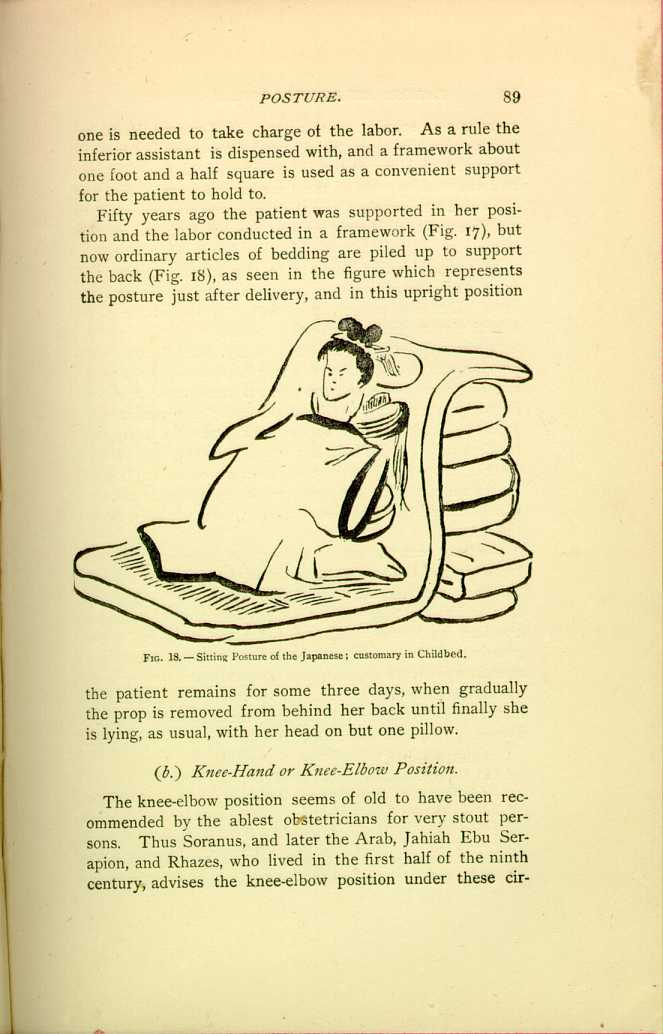
FIG. 18.—Sitting Posture of the Japanese; customary in
Childbed.
[Description: Woman sits on a blanket or thin mattress, and leans against a
pile of bedding. Black and white illustration.]
(b.) Knee-Hand or Knee-Elbow Position.
The knee-elbow position seems of old to have been recommended by the ablest obstetricians for very stout persons. Thus Soranus, and later the Arab, Jahiah Ebu Serapion, and Rhazes, who lived in the first half of the ninth century, advises the knee-elbow position under these circumstances;
In 1779, Hopkins objected to the lateral position and urged that the position on the hands and knees was the best.[64] Denman was of opinion that "this posture is instinctively sought by unassisted women.''[65] Whilst in 1791 that shrewd observer Charles White quoted Denman approvingly, and argued that the "knee-elbow position in natural labor prevented too great a pressure on the perineum.[66] According to Ramsbotham,[67] "the peasantry of Ireland placed themselves upon their hands and knees, and in Cornwall it is difficult to persuade the woman in labor to take any other posture than standing or on her knees.'' It is interesting to see how people carry these customs, which have been traditional among them for ages, across the seas.
We have seen the southern Negroes following the African ways, and the same may be observed among the Welsh, the Irish, and Germans; thus, Dr. H. C. Yarrow tells me that he had a patient once, a Welsh woman, who insisted on crawling on hands and knees while the pains were progressing, and who informed him that in Wales women frequently assumed this position or were delivered sitting upon the laps of their husbands. Irish women, who, as I am informed by several correspondents,[68] are in this country delivered in the hand and knee position, assert that this is
Major Charles R. Greenleaf, surgeon U. S. A., informs me that the Nez-Percés and Gros-Ventres women, who in ordinary labor are confined in a stooping posture, in cases where labor is protracted assume the knee-elbow position, whilst the patient's abdomen is encircled by a broad belt, upon which force is exerted by assistants, placed on either side of the patient, who scrupulously direct this force backwards and downwards during pains. The doctor himself witnessed such a case of protracted labor in a Gros-Ventre squaw, a primipara, who assumed the ordinary knee-elbow position and about whose abdomen a belt, often called the "squaw-belt,'' was placed.
The pressure exercised by the "squaw-belt'' among the Gros Ventre Indians is supplied by the pillow among the Creeks, and the encircling arms of an assistant among the Kootenais, whose labors are conducted in a most peculiar fashion, the parturient taking the knee-elbow position; she is on her knees, the face touching the ground; hands, one above the other, grasping a pole planted in the ground,
The Modocs, who as yet have assumed but few of the
customs of civilized life, are always delivered in this position;
their method is as peculiar as it is instructive, and is
worthy our most careful consideration; they maintain a
curved position, lying on the side, until the labor is nearly
completed, when they assume the position on their knees
and hands, which is continued until the child is
born.[71]
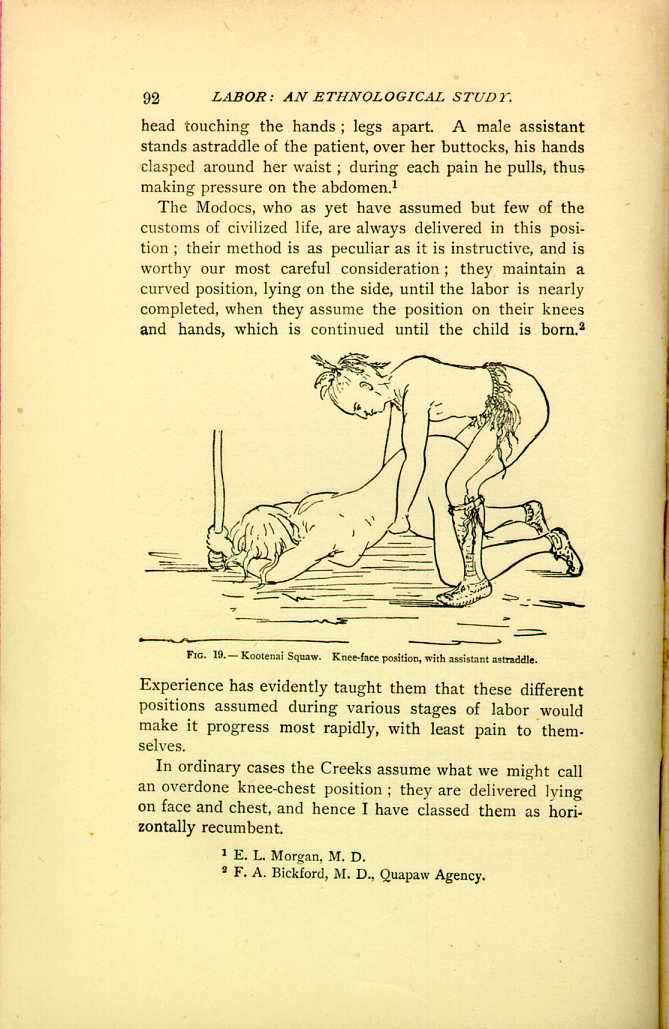
FIG. 19.—Kootenai Squaw. Knee-face position, with assistant
astraddle.
[Description: Woman kneels face down, gripping upright pole. Assistant
stands astride her with his hands just above her abdomen. Black and
white illustration]
In ordinary cases the Creeks assume what we might call an overdone knee-chest position; they are delivered lying on face and chest, and hence I have classed them as horizontally recumbent.
The natives of the Micronesian[72] and surrounding islands, like the Modocs, are delivered upon their hands and knees, sometimes in a recumbent position; certain of their old women act as midwives.
They roll about as they please until the very last stage the expulsion of the child, when they take this position, upon the hands and knees, and retain it usually until the placenta is expelled. They have no peculiar ceremonies, but apply to their ghost workers for intercession in their behalf in case of difficult labor or sickness. Massage and expression are used, especially for the expulsion of the placenta and after labor, to hasten the contractions of the womb, when the woman lies upon her back and her belly is kneaded. Difficult labor occurs seldom; and during thirty years' residence among the natives on the Micronesian Islands Mr. Sturgis, my informant, has never known of a single case of death of the mother in labor.
(b.)1.) Inverse Knee-Elbow Position.
This peculiar, and apparently strained, position has, like the knee-elbow position itself, been recommended for the relief of fat women in labor, more particularly by early Italian and German authorities. Thus Melli,[73] who however credits it to Mercurio,[74] "e prima di lui gli antichi maestri.'' The advantages assigned for this rather difficult position are, that the pressure of intestines and fat is thus removed; but as by the kindness of Drs. Fletcher and Yarrow, of the Surgeon General's Library in Washington, photographs of the original illustrations have been furnished me, they will be best explained in the words of Melli, p. 288, as follows:
"How a pregnant woman, who is very fat and corpulent, is to be placed and managed during labor.
"Difficult labor, caused by excessive corpulency, may be facilitated not only by the ordinary remedies prescribed before,
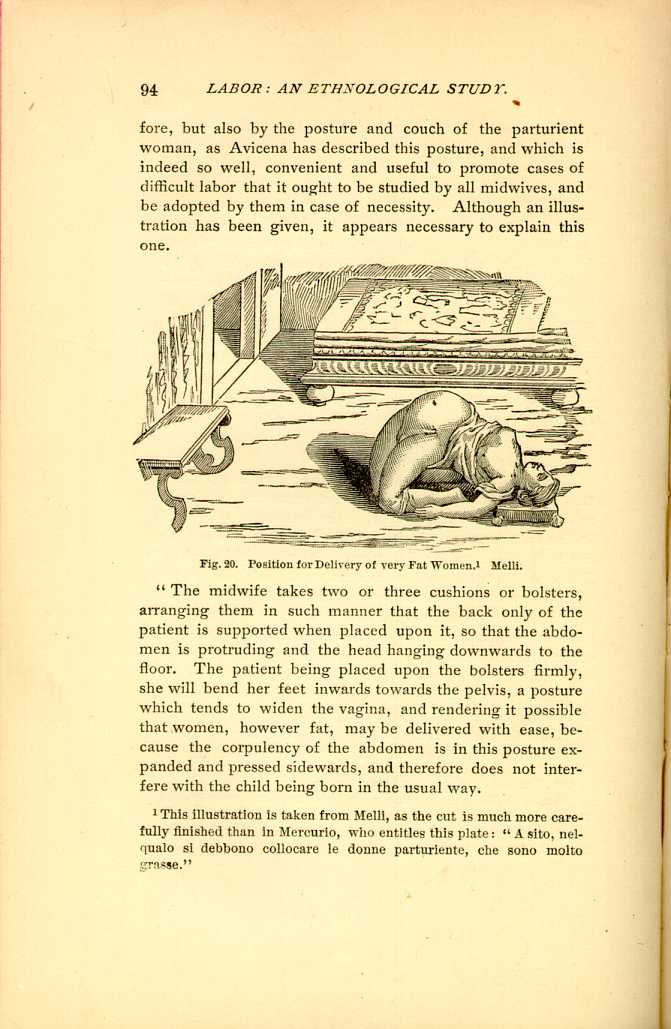
Fig.20. Position for Delivery of very Fat Women.[75] Melli.
[Description: Woman lies on her back, with her knees folded under her and her back arched. Black and white illustration.]"The midwife takes two or three cushions or bolsters, arranging them in such manner that the back only of the patient is supported when placed upon it, so that the abdomen is protruding and the head hanging downwards to the floor. The patient being placed upon the bolsters firmly, she will bend her feet inwards towards the pelvis, a posture which tends to widen the vagina, and rendering it possible that women, however fat, may be delivered with ease, because the corpulency of the abdomen is in this posture expanded and pressed sidewards, and therefore does not interfere with the child being born in the usual way.
"This posture and support is much more convenient, and
better in such a case than the best obstetric chair; for when a
parturient patient is sitting in an obstetric chair, her
abdomen, corpulency and intestines press upon the womb and
and fœtus, preventing its delivery and exit.''
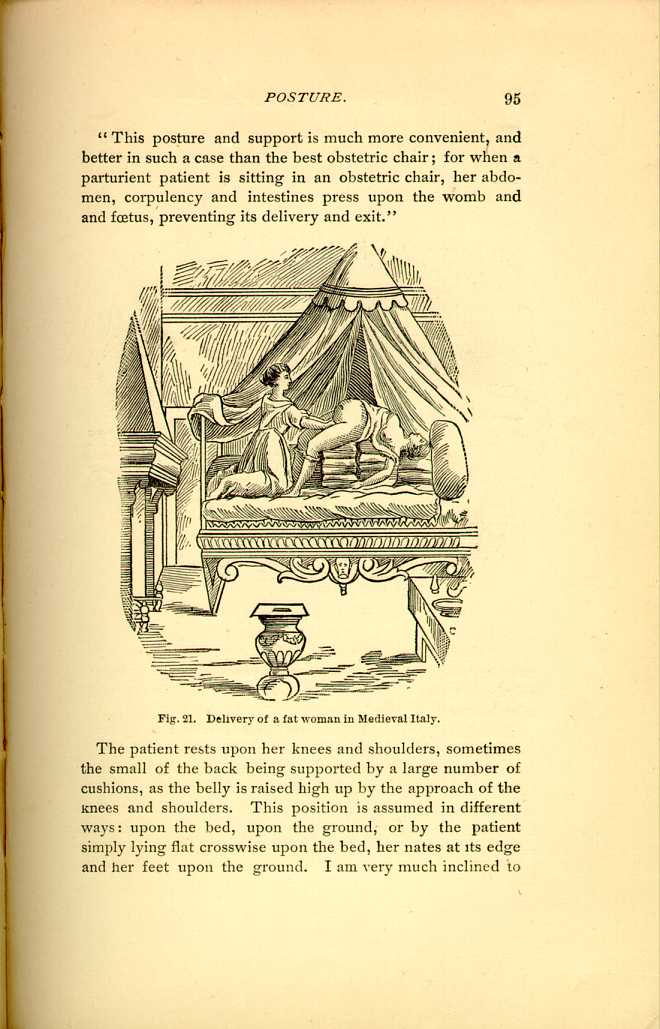
Fig. 21. Delivery of a fat woman in Medieval Italy.
[Description: Pregnant woman lies upon a bed, her back and head elevated upon
stacks of bedding. Another woman attends her.]
The patient rests upon her knees and shoulders, sometimes the small of the back being supported by a large number of cushions, as the belly is raised high up by the approach of the knees and shoulders. This position is assumed in different ways: upon the bed, upon the ground, or by the patient simply lying flat crosswise upon the bed, her nates at its edge and her feet upon the ground. I am very much inclined to
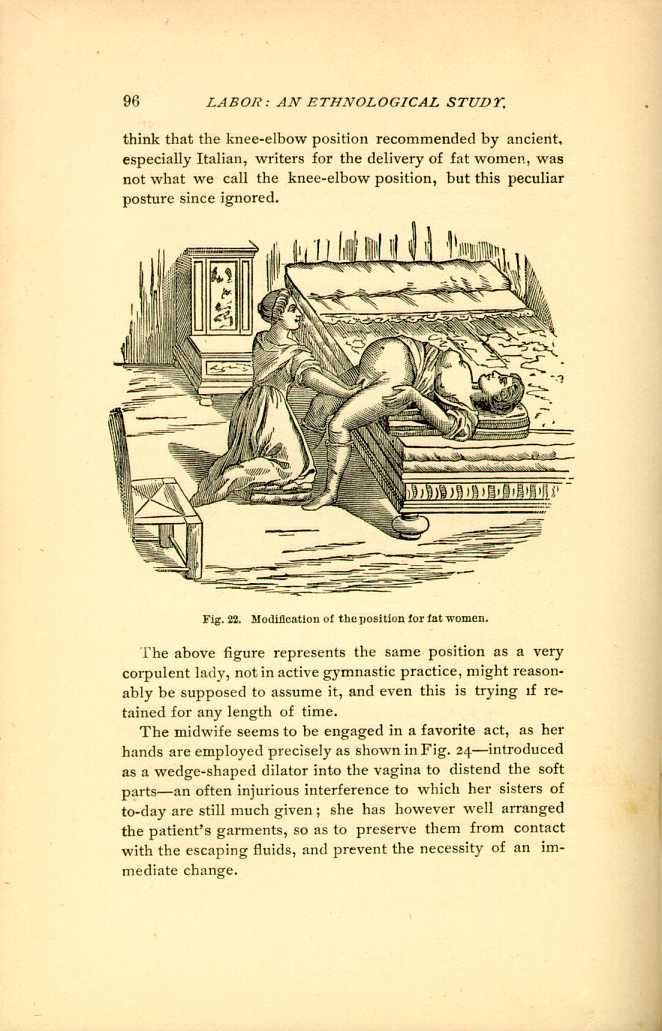
Fig. 22. Modification of the position for fat women.
[Description: Pregnant woman lies across bed, with her feet on the floor. Another woman kneels at bedside to deliver her. Black and white illustration.]The above figure represents the same position as a very corpulent lady, not in active gymnastic practice, might reasonably be supposed to assume it, and even this is trying if retained for any length of time.
The midwife seems to be engaged in a favorite act, as her hands are employed precisely as shown in Fig. 24—introduced as a wedge-shaped dilator into the vagina to distend the soft parts—an often injurious interference to which her sisters of to-day are still much given; she has however well arranged the patient's garments, so as to preserve them from contact with the escaping fluids, and prevent the necessity of an immediate change.
(c.) Kneeling, with the body erect, inclined backward, or partially suspended.
This, like other of those apparently peculiar positions which are fast yielding to the westward march of civilization and scientific medicine, was at one time not unusual in our States, and I will cite the early experience of Dr. Reamy in Ohio as characteristic of the practice thirty years ago; he says: "I have found in my practice ten or twelve different women, who had frequently borne children, before, who insisted, with a perseverance and determination that I dared not resist, in being out upon the floor, down upon their knees, leaning backward so that the buttocks almost touched the heels. The husband knelt behind the wife, with his arms around her, his broad strong hands acting as a pad for the abdomen, and making pressure during pains—à la Crédé—her shoulders resting against the man's chest. These women insisted that this was the only position in which they could be comfortably and successfully delivered.'' The same position, practically, is found among the Papagos. Among these Indians, "the position of the squaw, from the time the labor pains commence until the expulsion of the fetus and placenta, is a kneeling one, with the knees sufficiently spread to furnish comfortable lateral support to the body, which is erect. In the interval between the pains she is allowed to move about according to her inclination. In ordinary labors two women assist her. One of them places herself in a kneeling position behind the parturient woman, and with one knee pressing firmly in the lumbar region, she grasps with both hands the body of the patient immediately under the ribs in front. The other assistant places herself in a kneeling position in front of the woman, and with the palms of both hands rubs the abdominal wall down from the spine of the ilium to the pubes. It is interesting to note that they seem to appreciate the necessity and advisability of time and patience with primiparæ, as they do not resort to the same degree of pressure and friction which they employ in assisting multiparæ.[76]
The Yuma Indians vary this position somewhat.[77] The parturient woman is assisted by two others of long experience in the business. One of these kneels behind her, supporting her body in nearly an upright position, her arms passing under those of the patient and pressing or smoothing down the abdomen. The other assistant squats in front, between the feet of the patient, with her ankles crossed, and her shins pressed against those of the parturient woman, whilst she holds her by the hands or wrists. The posture of the patient is, therefore, with the shoulders high, the legs and thighs strongly flexed and abducted, which position is retained until the expulsion of the placenta. No bandage is used.
The Upper Klamath and nearly related Modocs of Oregon are usually delivered in a small lodge some distance away from the other houses. The parturient also assumes a kneeling position, supported by one old squaw, whilst another keeps kneading and rubbing her abdomen. Sometimes she varies her posture by sitting and pressing her feet against some support, while she bears down. If labor is tedious, they often sit over warm stones moistened with water, or, in other words, take a steam bath to relax the system. They also steam themselves occasionally for several days after the birth of the child.[78]
Precisely this same position is found among many of the Mongolians, especially the Tartars, if we may accept the authority of Hureau de Villeneuve.[79] The parturient moves about during the early pains, sometimes standing with her hands above her head, but as soon as the bearing-down pains begin she assumes the kneeling position last described, almost erect, supporting her body upon the hands, which rest upon the separated knees or thighs; the assistant behind supports her by seizing her under the arms, whilst the midwife rests upon one knee in front of the patient.
My attention once called to the subject, I examined my own collection, and found in it two images representing a woman in the erect kneeling posture, the knees somewhat separated, the hands resting upon the knees or thighs in precisely the same position as that assumed by the Mongolians, and probably the Yumas. It is not unlikely that these figures represent parturient women, and it is highly probable that the mythical Mound Builders, be they predecessors of our Indians, or older tribes of the same stock,
The kneeling, partially suspended, position is found among
the Indians and lower classes of Mexicans in the neighborhood
of San Luis Potosi. The labor is conducted in the
following way: a round stick of pine wood, eighteen or
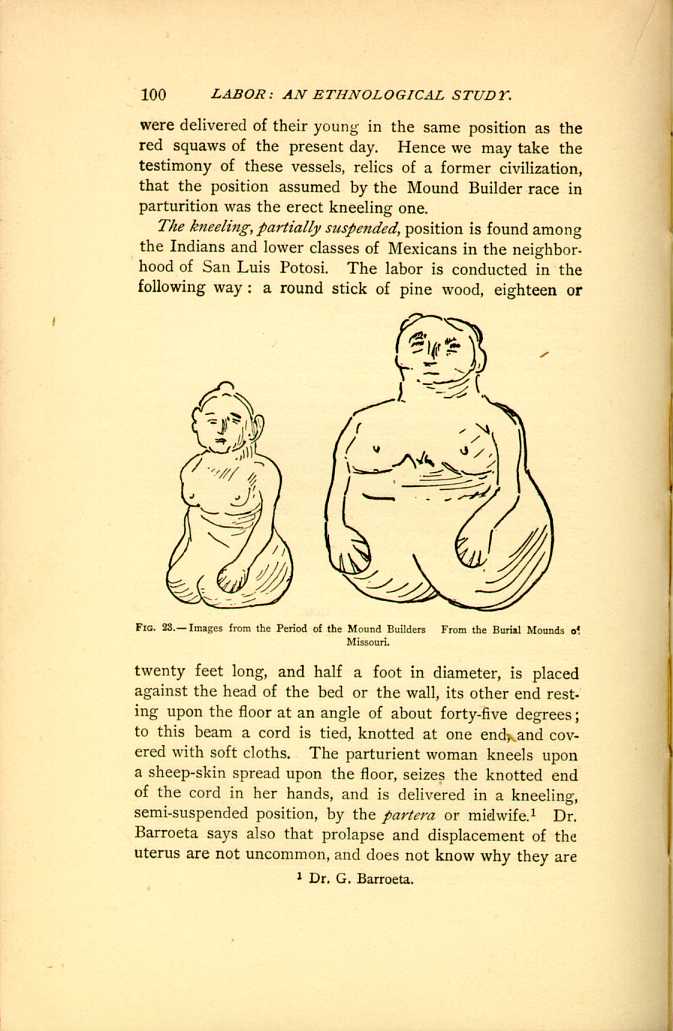
Fig. 23.—Images from the Period of the Mound Builders
From the Burial Mounds of
Missouri.
[Description: Two female figures in erect kneeling posture. Black and white
illustration.]
The lower classes of Northern Mexico speak the Spanish
language and profess the Catholic faith, but in all other
respects are Indians, and retain many Aztec customs; so
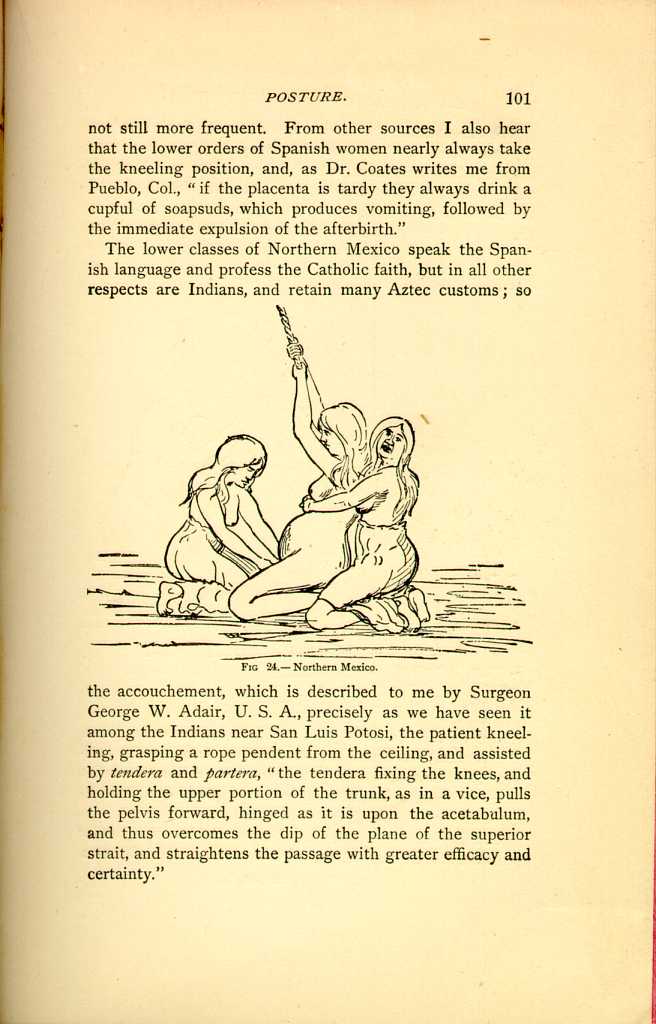
FIG 24.—Northern Mexico.
[Description: Pregnant woman kneels, holding onto a rope suspended overhead.
One woman kneels behind her, her hands clapsed above the abdomen, while
another woman kneels before her to assist delivery]
The American Indians on the frontier of Mexico follow
the same traditional method of delivery, hanging on a rope
suspended from a rafter, with the knees bent and just off
the ground. The rope, which is wrapped with cloths or
towels so as to make it softer, usually hangs at the edge of
the bed, so that the patient can stand on her feet or sit or
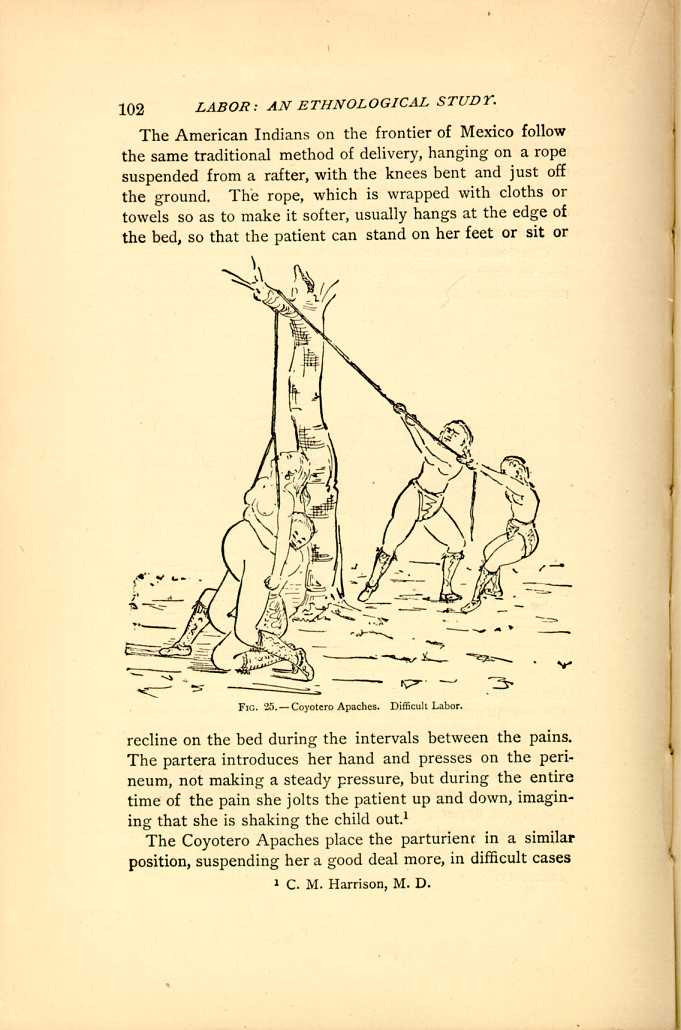
FIG. 25.—Coyotero Apaches. Difficult Labor.
[Description: Pregnant woman is supported by a loop of rope which has been
thrown over a tree branch in a pulley arrangement. Two assistants hold
the other end of the rope, while a third assistant hangs upon the
pregnant woman, placing pressure upon her abdomen.]
The Coyotero Apaches place the parturient in a similar position, suspending her a good deal more, in difficult cases
The Santee Indians are almost invariably delivered in a kneeling posture on the floor, with a bench or chair in front of them upon which they rest their arms, while sometimes they have a rope attached above by which they partially suspend themselves, just as the Mexican Indians and half-breeds do.[84]
(d.) Kneeling Postures, where Precise Description is Lacking.
Unfortunately, Dr. Ploss, in his valuable and interesting work, has failed to define precisely the positions assumed, and, as I have been unable to refer to the authorities myself, I will take the liberty of stating in a general way, upon the authority of Dr. Ploss, that the kneeling posture is assumed occasionally, at least, by women in labor in Nicaragua,[85] in Finland,[86] in modern Greece,[87] in Kamtschatka, in eastern Asia; and, if we go back to the Middle Ages, among the Abyssinians,[88] a people who originally came from Asia, where, as we have already said, among the yellow races the kneeling posture is a common one; also, under certain circumstances, in Rome; among the Arabs and Germans in the Middle Ages. Finally, in ancient times, among the Pelasgians, if some Greek authors are correctly translated.
If I may be permitted to refer to the somewhat vague
4. SEMI-RECUMBENT.
The semi-recumbent positions are by far the most frequent among the ancients, especially among the more civilized people of olden times, and among the savage races of the present day. The same position of the body is assumed by various races in very different ways, there being apparently no resemblance in the method of delivery, whilst it appears, upon more careful study, that the position of the body, the inclination of the trunk and the pelvic axis, together with the relaxed position of the thighs, is almost identical, the same end being accomplished in ways very different, peculiar to each people, and in keeping with their surroundings. Thus, the simplest of the semi-recumbent positions, which is upon a par with the customs of the rudest African races, is sitting upon the ground, upon a stone or rude cushion, with the body inclined backward, leaning against an assistant, a tree, or some other object. A marked progress is achieved, when we find the parturient woman seated in the lap of an assistant reclining against his chest, a position which reaches its greatest perfection in the obstetric chair. As the next step, I regard the dorsal decubitus, a position modified according to the circumstances of the people. In the wilds of Africa, and in the interior of our western country, the patient finds her couch upon the floor, propped up against some staves of wood or a pile of grass, whilst in the lying-in chamber of the civilized people
(a.) Sitting Semi-recumbent on the Ground, upon a Stone, or Stool.
Among our Indians we find that the Otoes, Missouris, Omahas, Iowas, and nearly related tribes assume the sitting posture, the legs widely separated; but as the crisis supervenes, the patient raises herself somewhat by a rope suspended above, thus attaining an inclined, semi-recumbent position.[90] The Wakah squaw assumes a sitting posture, on the floor of the lodge, with nothing but an Indian mat under her. As soon as the labor pains come on her feet are drawn up close to the buttocks, and the legs flexed; this position is maintained until after the birth of the child and the expulsion of the placenta.[91]
The women of the Skokomish Agency, W. T., sit down with a pillow or roll of blankets resting against the perineum; one squaw supports the back, while another receives the child. This position is a slightly recumbent one, the buttocks resting on the pillow or roll of blankets.[92] The Confederated tribes of the Flatheads, Pend d'Oreilles, and Kootenais, follow a similar custom: a small box, or a piece of wood, six or eight inches high, covered with old pieces of blanket or buffalo robes, is the seat upon which the sick woman is placed; her legs are separated and flexed so that the heels almost come in contact with the seat. She is retained in that position by two assistants who hold her by the arms, and sometimes a third one stands behind and presses upon her shoulders, and in this position the child is expelled.[93]
Though apparently uncomfortable and inconvenient, and rare among the American Indians, the Kaffirs universally
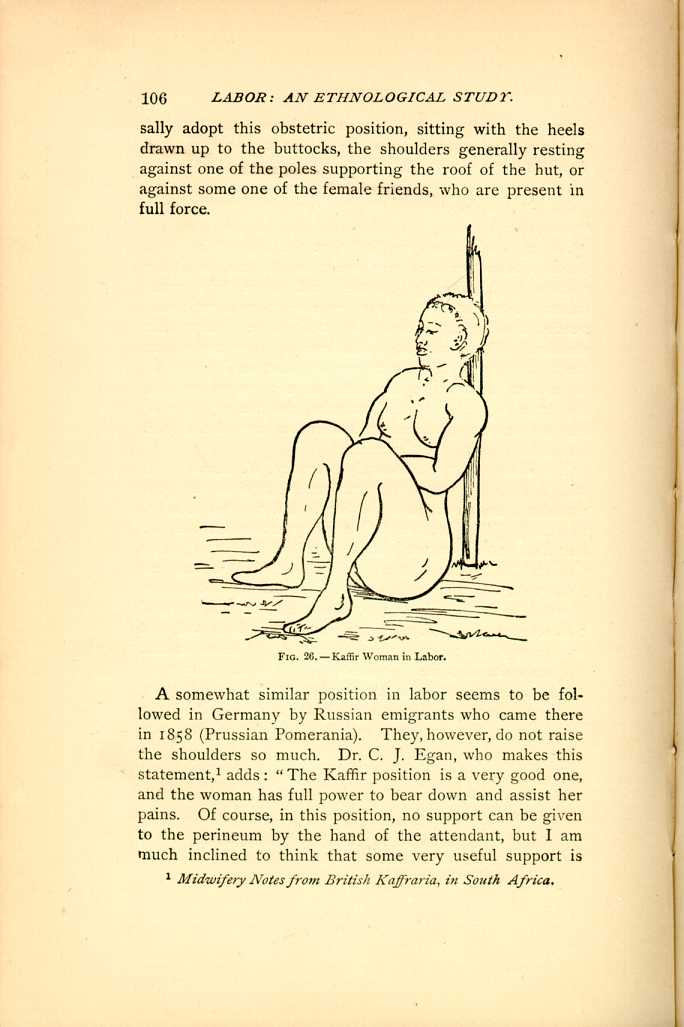
FIG. 26.—Kaffir Woman in Labor.
[Description: Woman sits with her knees up, leaning against a pole. Black and white illustration.]A somewhat similar position in labor seems to be followed in Germany by Russian emigrants who came there in 1858 (Prussian Pomerania). They, however, do not raise the shoulders so much. Dr. C. J. Egan, who makes this statement,[94] adds: "The Kaffir position is a very good one, and the woman has full power to bear down and assist her pains. Of course, in this position, no support can be given to the perineum by the hand of the attendant, but I am much inclined to think that some very useful support is
The Kaffir and the Indian woman sit upon the ground, whilst the somewhat more advanced half-breed, as she is often found in Southern California and New Mexico, seats herself upon a chair, and during the pains, in the same way as her Indian sister, grasps a rope suspended from the ceiling above; but, when tired out in this position, she is often found kneeling upon the ground.[95] A white sister involuntarily testifies to the efficiency of this position, at least under certain conditions,—a primipara who had been in labor for two days and was confined on the third, in a sitting posture, the pains ceasing entirely whenever she assumed a recumbent position; of this the observing attendant, Dr. Von Mansfelde, of Ashland, Neb., assured himself. In order to satisfy himself that it was not the whim of a parturient woman, he placed her on the bed, on her side and back, several times, but the hand placed upon the fundus showed complete relaxation; no sign of contraction. When replaced in the sitting posture the pains readily returned, and were very effective, the woman being delivered within two hours after dilatation of the os.
The Arab woman is seated on two flat stones, or, more properly, her buttocks are slightly supported upon two flat stones, whilst during each pain she partially raises herself by a rope which is suspended from the centre-pole of the tent. Two assistants seize the parturient woman under the shoulders, and she herself, during the pain, raises herself by the rope; they aid this motion, partially suspend her, shaking her well, as the miller does his sack of flour when he empties it, and then, as the pains cease, they drop her back upon the stones. This, at least, was the practice witnessed in several cases in 1858 by Dr. Goguel,[96] in one instance,
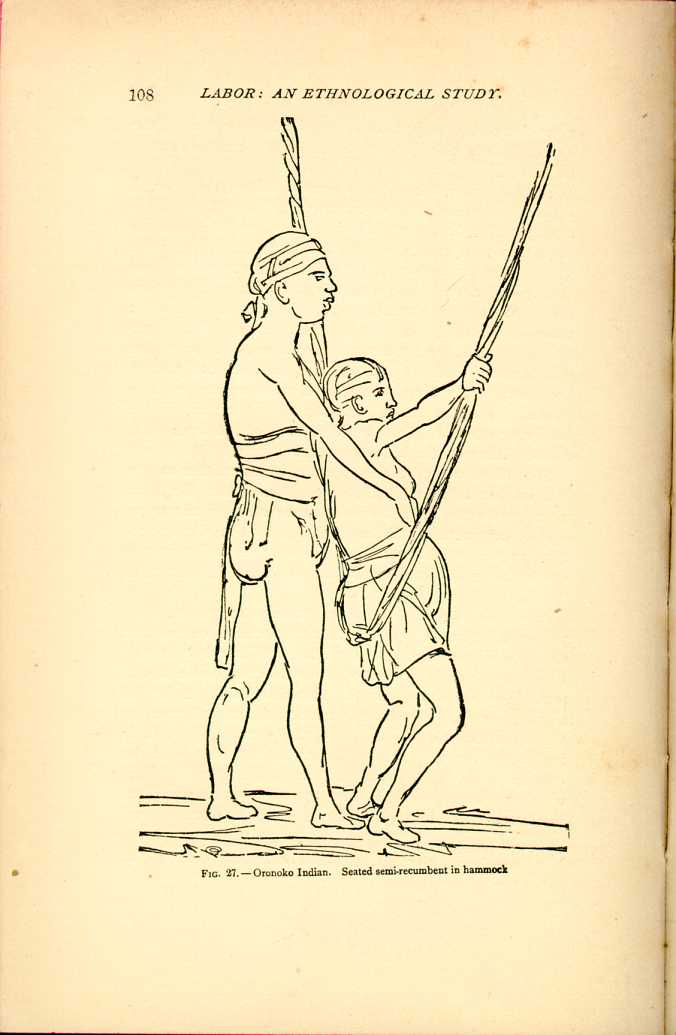
FIG. 27.—Oronoko Indian. Seated semi-recumbent in hammock.
[Description: Pregnant woman sits in a hammock resembling a looped rope, while an assistant stands behind her with hands on her abdomen.]A most admirable position, typically semi-recumbent, was customary in Greece and her provinces 2,200 years ago, as is proven by that interesting group, representing a labor just completed, which was discovered by General di Cesnola during his researches in Cyprus; we, moreover, have the same undeniable evidence that this marble group faithfully represents the obstetric position in Cyprus twenty-two centuries ago as we have of the correctness of the Peruvian posture at the time of the Inkas, as pictured upon the funeral urn. The native Peruvians of the present day are still confined whilst seated upon the husband's lap; and the Cypriote midwife of to-day still places her patient in the semi-recumbent position upon a low stool which she carries about with her.
In response to my inquiries, General di Cesnola kindly furnished me with the following most valuable information. He says: "The group was found among the déris of the temple at Golgoi, in 1871, and is of the best Greek epoch, say 400 B. C. The chair on which the woman is reclining, is Cypriote, and was probably used also in Greece at that period; the modern Cypriote midwives possess similar low chairs, which they carry with them when going to attend a child-birth, and I have myself seen the circumstances as shown in that group, which faithfully represents the parturition
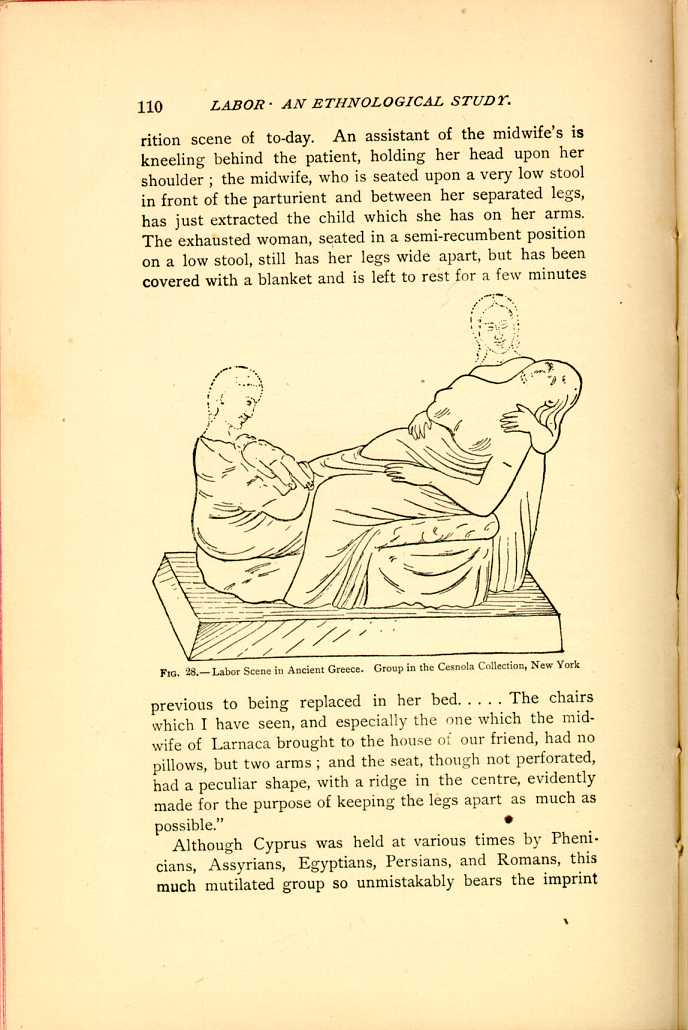
FIG. 28,—Labor Scene in Ancient Greece. Group in the Cesnola Collection, New York
[Description: Woman gives birth, assisted by two ghostly figures.]Although Cyprus was held at various times by Phenicians, Assyrians, Egyptians, Persians, and Romans, this much mutilated group so unmistakably bears the imprint
FIG. 29.—Modern Cypriote Midwife's Chair.
[Description: Low midwife's chair, without legs and with arm rails. Black and white illustration.]In southern India the patient walks about during the earlier stages of labor, then sits upon the ground with the thighs well separated, the back supported by an assistant, whilst the delivery itself is finally accomplished while lying upon the ground.[99]
(b.) Sitting on the Lap or between the Thighs of an Assistant who is seated on a Chair or on the Floor.
I look upon this position as identical with that on the obstretric chair, although more simple and more ancient; and I believe that it will be apparent to every one, if the relative positions are considered, that the obstetric chair is merely an imitation of the more pliable and sensitive support afforded by the husband or assistant, who is himself made to suffer whilst holding the parturient woman during
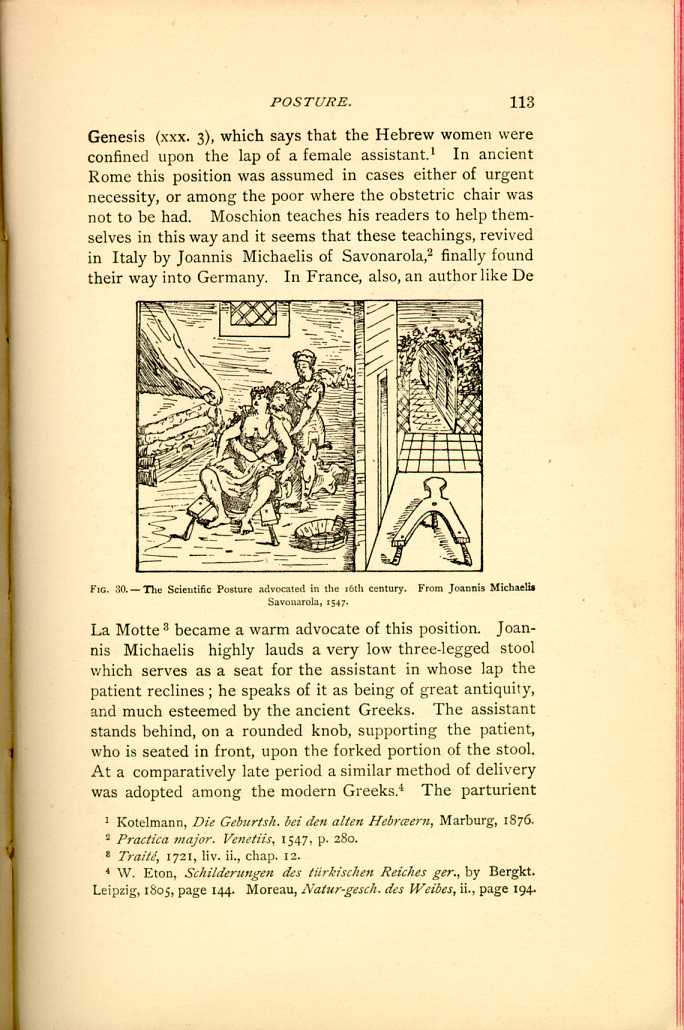
FIG. 30.—The Scientific Posture advocated in the 16th century. From Joannis Michaelis Savonarola, 1547.
[Description: Woman seated on low y-shaped stool, with assistants behind her. Black and white illustration.]We have seen how the modern Peruvians still follow the ways of the Incas, and so the descendants of these Germans, Welsh, or Scotch have not forgotten the habits of their ancestors, although they have crossed the seas and have mingled with a more enlightened civilization. It may surprise some of our city practitioners of to-day, who see little of the country population, and especially those who have not practiced in rural districts years ago, that in our
A graphic description of obstetric practice in the rural
districts of Ohio is given me by Dr. E. B. Stevens of Lebanon,
Ohio, and embodies all that has been written me from
other States. To quote his own words: "When I commenced
to practice, a good many years ago, the almost universal
habit of confinement throughout the regions of southern
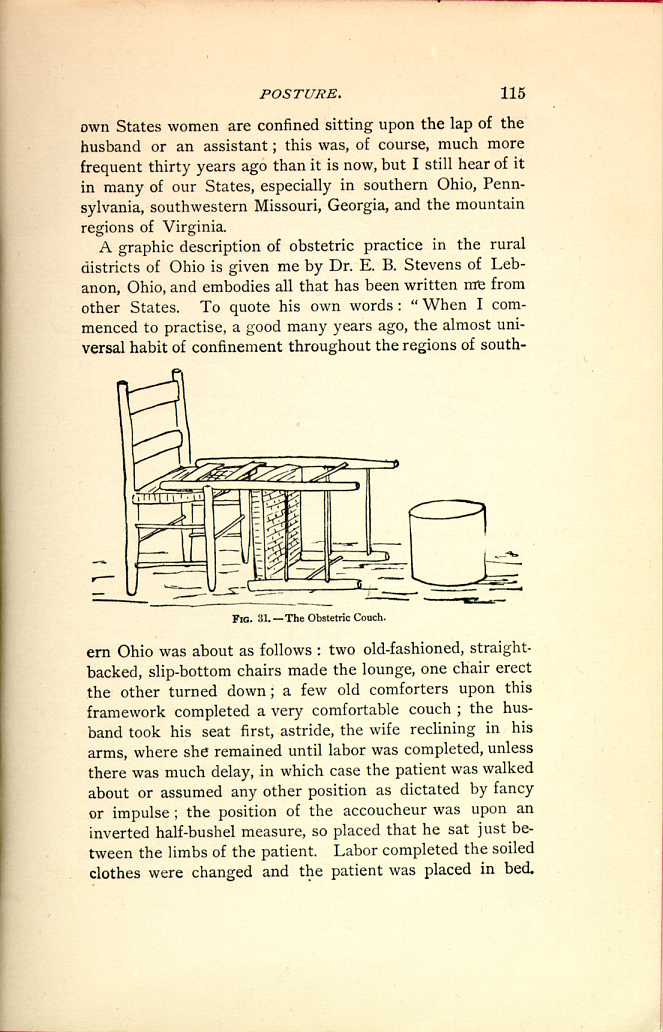
FIG. 31.—The Obstetric Couch.
[Description: One straight-backed chair upright, with a second overturned so
that its back rails rest upon the seat of the first chair. Black and
white illustration.]
I have been told of this position in so many different
parts of this country that it would be superfluous to refer
to individual statements; it is found in Pennsylvania, and
among Pennsylvania emigrants in southwestern Missouri,
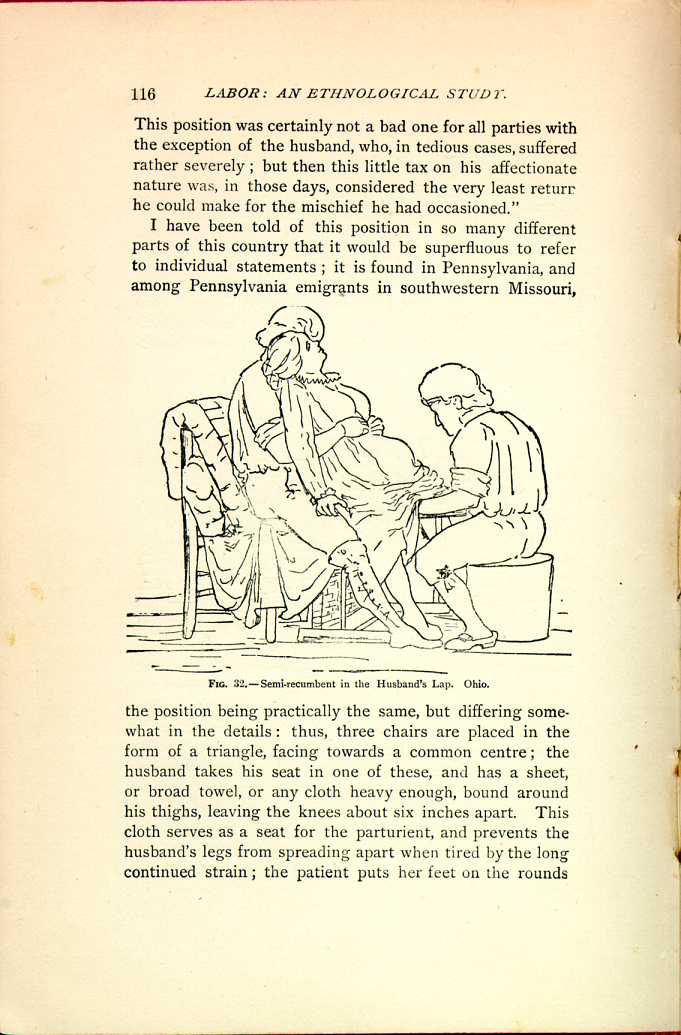
FIG. 32.—Semi-recumbent in the Husband's Lap. Ohio.
[Description: Wife reclines in husband's lap, while another person assists in
the delivery. Black and white illustration.]
A professional friend in this State, who, like many other
practitioners, tells me that the first patient he ever delivered
was confined in this position, says that since then he
has delivered quite a number of women in this way, and
thinks it a great help in cases where the head constantly
retreats after the pain ceases; in the rural districts of
Georgia both negro and white women, now and then, still
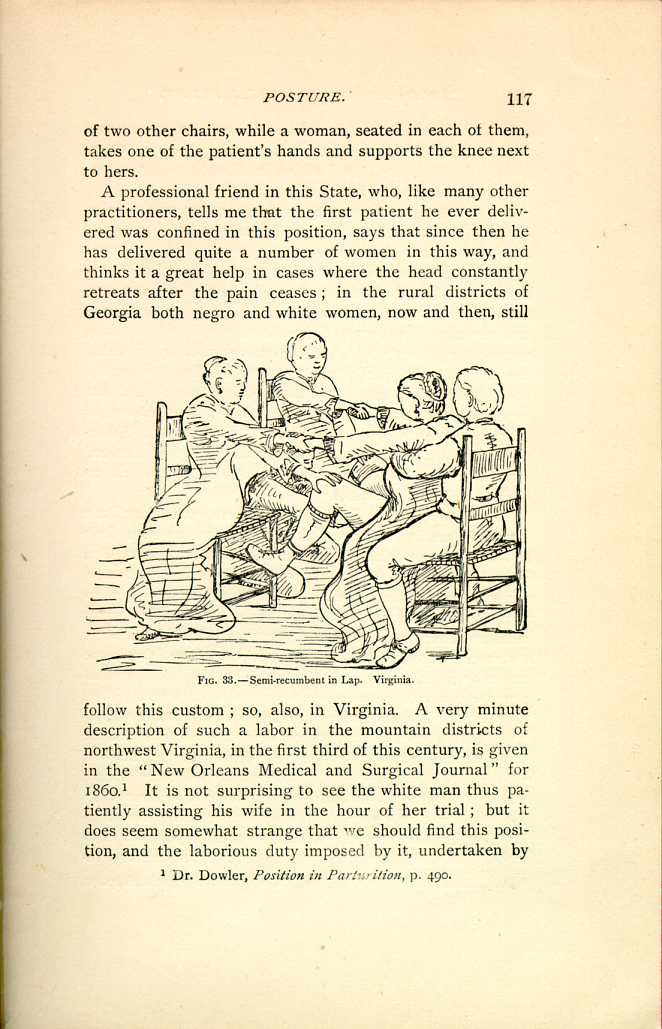
FIG. 33.—Semi-recumbent in Lap. Virginia.
[Description: Pregnant woman sits in husband's lap while two friends sit
facing them in straight-backed chairs, each supporting one of her knees
and holding one of her hands. Black and white illustration.]
The Indians, and lower class of Mexicans in the vicinity of San Luis Potosi, are confined either in a kneeling position partially suspended, or sitting upon the floor. If confined in the latter position, the accouchée sits on a sheepskin on the floor, between the legs of one of the assistants, the tenedora, or holder, who is seated on a little cushion, and serves as a support to the patient, her thighs pressing against the patient's hips, and her arms encircling her waist, the hands clasped just above the fundus of the distended uterus, so that she can follow the child in its descent, and exert a gradual but strong compression; the partera, of course, takes her position in front of the patient. Sometimes, in a tedious labor, this awkward posture is retained for one or two days, with not a little suffering to the tenedora as well as the patient.[108]
The custom of the Sandwich Islanders varies very little from this, and it is a matter of some interest to note their habits, as these islands, two thousand miles west of San Francisco, were entirely unknown one hundred years ago, and even fifty years ago were perfectly barbarous; it is important to us, more especially as they still retain, in a great measure, their crude ideas and practices. Very interesting statements as to the obstetric practices in these islands are made by Dr. Charles H. Wetmore,[109] who has had a professional experience of twenty-two years upon Hawaii. When the labor is fairly commencing, the patient assumes a sitting posture upon a hard pillow or stone, her husband, or some intimate male or female friend, kneeling behind her, whose duty it is to clasp her above the abdomen in such a way that he can press down with considerable force upon the uterus and its contents, never relaxing this grasp to allow the fetus to recede. The accoucheur's position is in front; she has little to do but to receive the child. Precisely
I have repeatedly had occasion to refer to the nomadic
and barbarous tribes of Asia, as they have so successfully
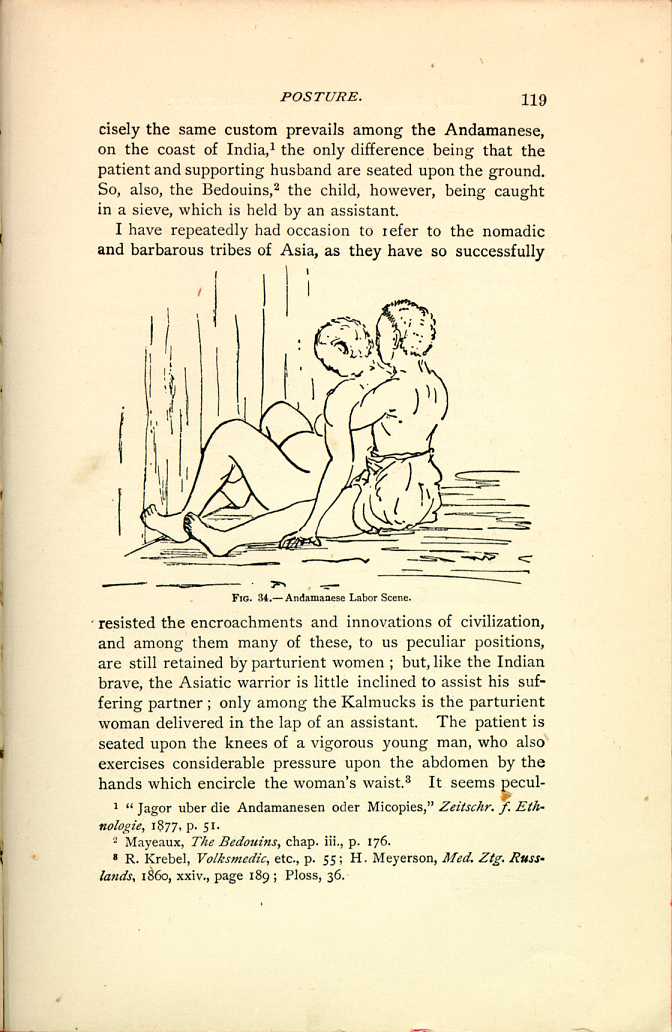
FIG. 34.—Andamanese Labor Scene.
[Description: Pregnant woman sits on floor, facing wall, while assistant sits
behind her with legs spread, supporting her. Black and white
illustration.]
(c). The Obstetric Chair.
The positions we have so far considered have been almost
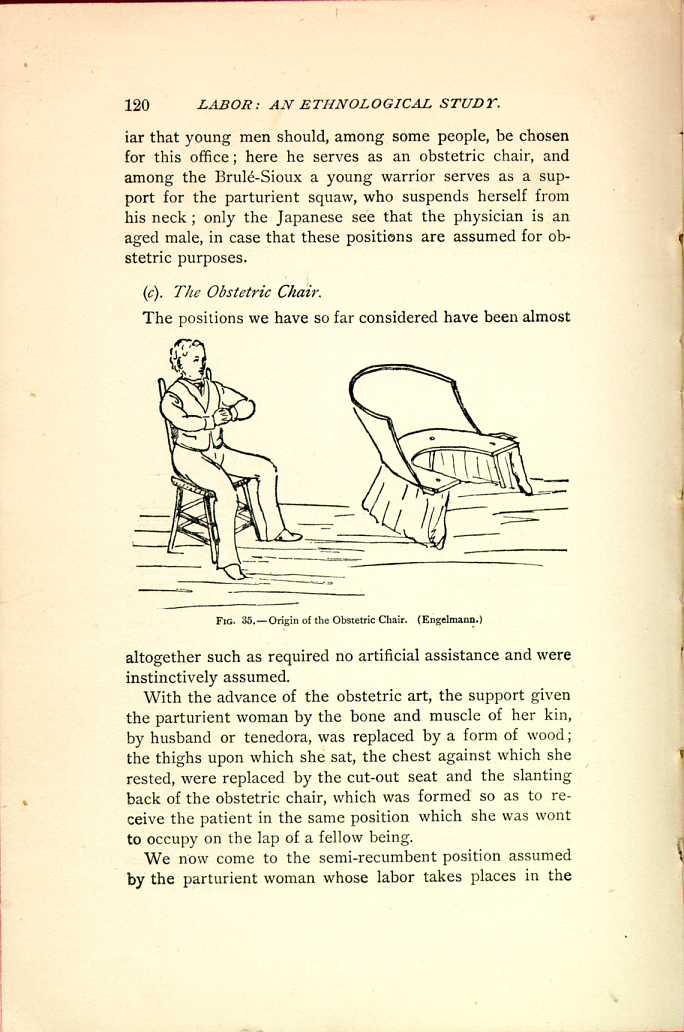
FIG. 35.—Origin of the Obstetric Chair. (Engelmann.)
[Description: Man sitting in chair with legs spread; obstetric chair with
U-shaped seat, providing similar support for back and legs. Black and
white illustration.]
With the advance of the obstetric art, the support given the parturient woman by the bone and muscle of her kin, by husband or tenedora, was replaced by a form of wood; the thighs upon which she sat, the chest against which she rested, were replaced by the cut-out seat and the slanting back of the obstetric chair, which was formed so as to receive the patient in the same position which she was wont to occupy on the lap of a fellow being.
We now come to the semi-recumbent position assumed by the parturient woman whose labor takes places in the
The obstetric chair marks a decided era in the history of
the art; but I must consider that period as a whole, and in
speaking of the chair I have reference to its more characteristic
features, to those points which are common to all obstetric
chairs, as it is not my purpose here to describe the
various obstetric chairs which were in use at different times,
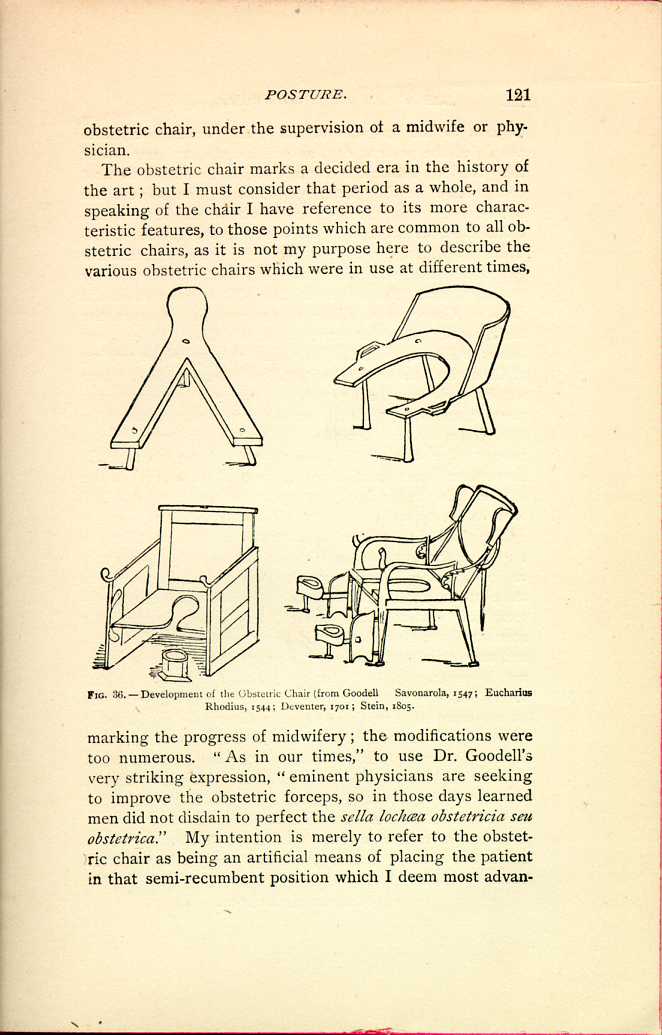
FIG. 36.—Development of the Obstetric Chair
(from Goodell Savonarola, 1547; Eucharius
Rhodius, 1544; Deventer, 1701; Stein, 1805.
[Description: Four different varieties of obstetric chairs are depicted.
Black and white illustration.]
The chair is mentioned by Albertus Magnus in the thirteenth century, and in the German translation of this work, under date of 1589, an illustration is given which resembles the obstetric chair of Soranus and Moschion. In the seventeenth and earlier part of the eighteenth century the chair seems to have flourished in Germany, and also in England, and numerous modifications were introduced. Its supremacy, however, was not of long duration, and it soon yielded to the modern recumbent position, and was only retained by the more conservative people in the rural districts, who follow but slowly in the wake of any advance. Smellie[113] says: "In remote parts of England the patient sat upon a stool made in the form of a semicircle.'' This, of course, was during the time of the decline of the chair, when the dorsal and lateral decubitus had become popular.
In the seventeenth century it was to be found in the centres of medical learning, and had not yet been forced back into the rural wilds.
As a matter of curiosity. I will cite the title of a work published in 1637, in which it was warmly advocated, and I will add a brief description of the chair, in the quaint language of the book, kindly furnished me by Dr. Wise, of the Surgeon-general's Library, and it will answer for this as well as all other chairs, and will serve to show the importance attached to its various features.
"The Expert Midwife: or, an Excellent and most necessary Treatise of the Generation and Birth of Man. Wherein is contained many very Notable and Necessary Particulars requisite to be knowne and practiced: with Divers Apt and Useful Figures appropriated to this Worke. Also the Causes, signes, and Various Cures, of the most Principall Maladies and Infirmities incident to Women. Six Books compiled in Latine by the Industry of James Rueff, a Learned and Expert Chirurgion: and now translated into English for the Generall Good and Benefit of this Nation.''
"Let the stoole be made compassewise, under-propped with foure feet, the stay of it behind bending backward, hollow in the midst, covered with a blacke cloth underneath, hanging downe to the ground, by that meanes that the labouring woman may be covered, and other women sometimes apply their hands in any place, if necessity require. Let the stoole be furnished and covered with many cloths and clouts at the back and other parts, that the labouring woman receive no hurt, or the infant anywhere, strongly kicking and striving because of the paines, stirrings and motions of the mother. And after the labouring woman shall be set in her chaire about to be delivered, the midwife shall place one woman behind her back which may gently hold the labouring woman, taking her by both the armes, and if need be, the pains waxing grievous, and the woman labouring, may stroke and presse downe the wombe, and may somewhat drive and depress the infant downward. But let her place other two by her sides, which may both, with good words, encourage and comfort the labouring woman, and also may be ready to helpe and put to their hand at any time. This being done, let the midwife herselfe sit
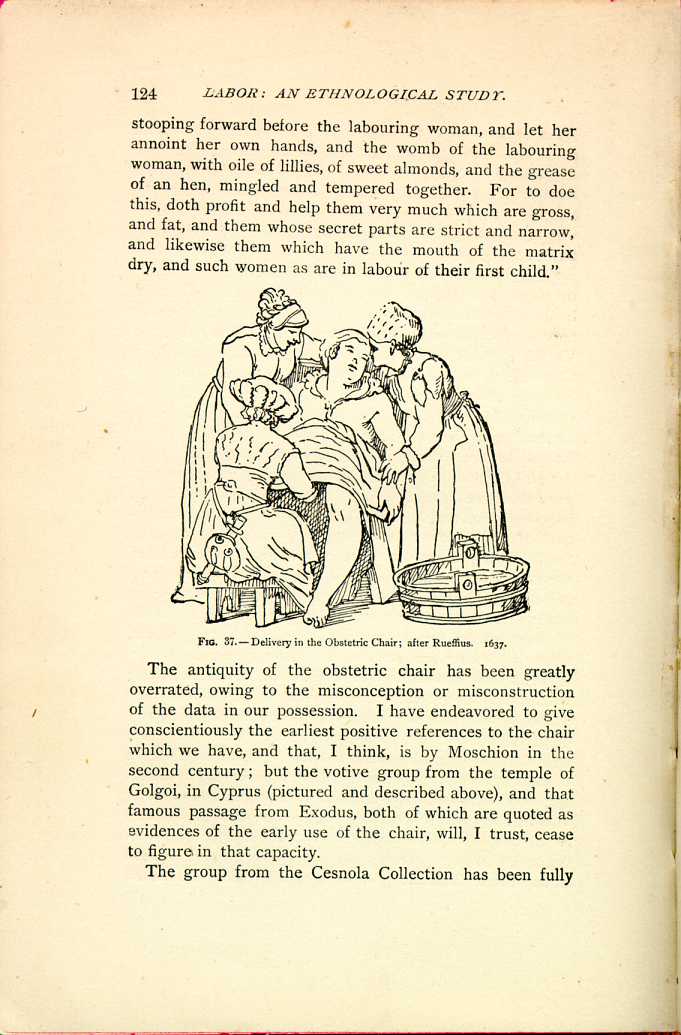
FIG. 37.—Delivery in the Obstetric Chair; after Ruegius. 1637.
[Description: Pregnant woman reclines in an obstetric chair, while a midwife and two friends attend her. Black and white illustration.]The antiquity of the obstetric chair has been greatly overrated, owing to the misconception or misconstruction of the data in our possession. I have endeavored to give conscientiously the earliest positive references to the chair which we have, and that, I think, is by Moschion in the second century; but the votive group from the temple of Golgoi, in Cyprus (pictured and described above), and that famous passage from Exodus, both of which are quoted as evidences of the early use of the chair, will, I trust, cease to figure in that capacity.
The group from the Cesnola Collection has been fully
I have already called attention to the fact that those nations
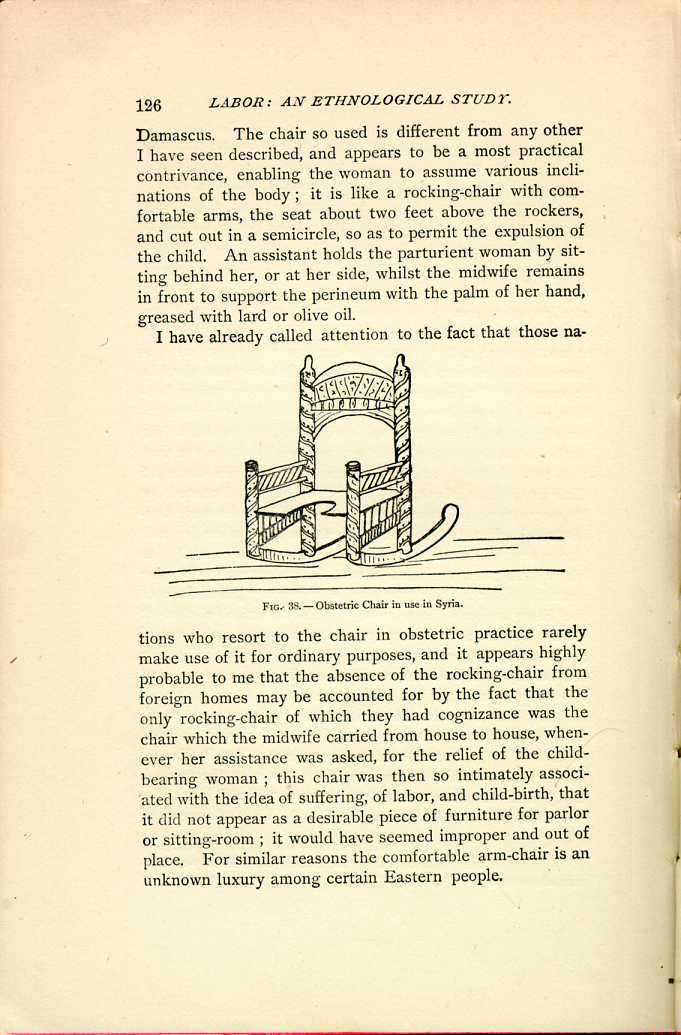
FIG. 38.—Obstetric Chair in use in Syria.
[Description: Obstetric chair designed like a rocking chair, with U-shaped
seat. Black and white illustration.]
It is only within late years that the American rocking-chair has found its way across the ocean, and the increased facilities for intercourse, and the spread of a leveling civilization, will soon do away with these remnants of former times which still linger here and there. Amongst the modern Egyptians, the midwife makes use of a chair, "Kursee El-Wiladeh,'' which is covered with a shawl, or an embroidered napkin, and some flowers of the henna tree, or some roses, are tied with an embroidered handkerchief to each of the upper corners of the back; thus ornamented, the chair is conveyed before the midwife to the house. In the houses of the rich, the parturient is placed on a bed after delivery, and usually remains there from three to six days, whilst the poor women resume their ordinary occupation in a day or two.[116] I will add that Lane, like almost every other author, refers to that passage, Exodus i. 16, intending to compare the custom of using the chair among the Egyptians with that of the ancient Hebrews. In Palestine, the obstetric chair is still an honored institution, but much simplified in form, being sometimes nothing more than an old-fashioned arm-chair.
(d.) Semi-recumbent Position, Strictly Speaking.
Although I have grouped as semi-recumbent all the positions last spoken of, I will, in this subdivision, confine the use of the expression more closely, and will class as semi-recumbent, strictly speaking, only those positions in which the patient assumes the dorsal decubitus with the head and shoulders raised, the axis of the body inclined at an angle of about forty-five degrees.
Like many other of these curious positions, this one is found in our own States, but seems to have come to us from the French settlers in the north. In Vermont, some thirty years ago, a semi-recumbent position was customary, which may either be looked upon as a rude imitation of the obstetric chair, or as a semi-recumbent position, strictly
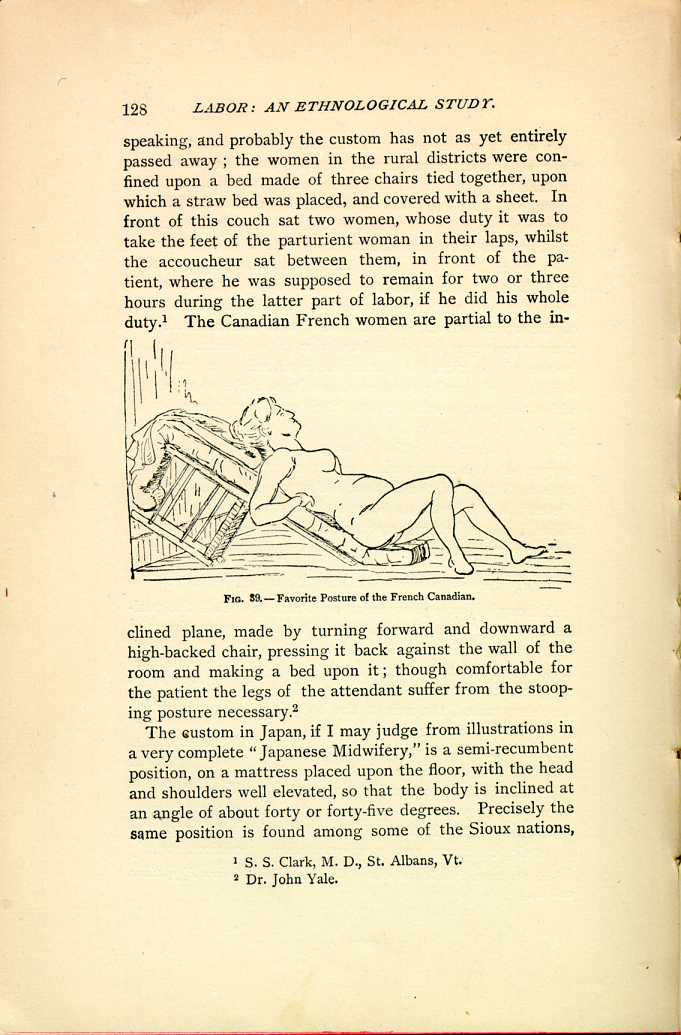
FIG. 59.—Favorite Posture of the French Canadian.
[Description: Pregnant woman reclines on an inclined surface created by propping an overturned chair against the wall and covering it with bedding.]The custom in Japan, if I may judge from illustrations in a very complete "Japanese Midwifery,'' is a semi-recumbent position, on a mattress placed upon the floor, with the head and shoulders well elevated, so that the body is inclined at an angle of about forty or forty-five degrees. Precisely the same position is found among some of the Sioux nations,
The Ute, Comanche, Apache, Navajoe, and Nez-Percés
woman is also confined in the semi-recumbent dorsal position,
the head and shoulders of the patient being frequently
supported in the lap of an attendant, while the patient has
access to a rope or brace placed within
reach.[119]
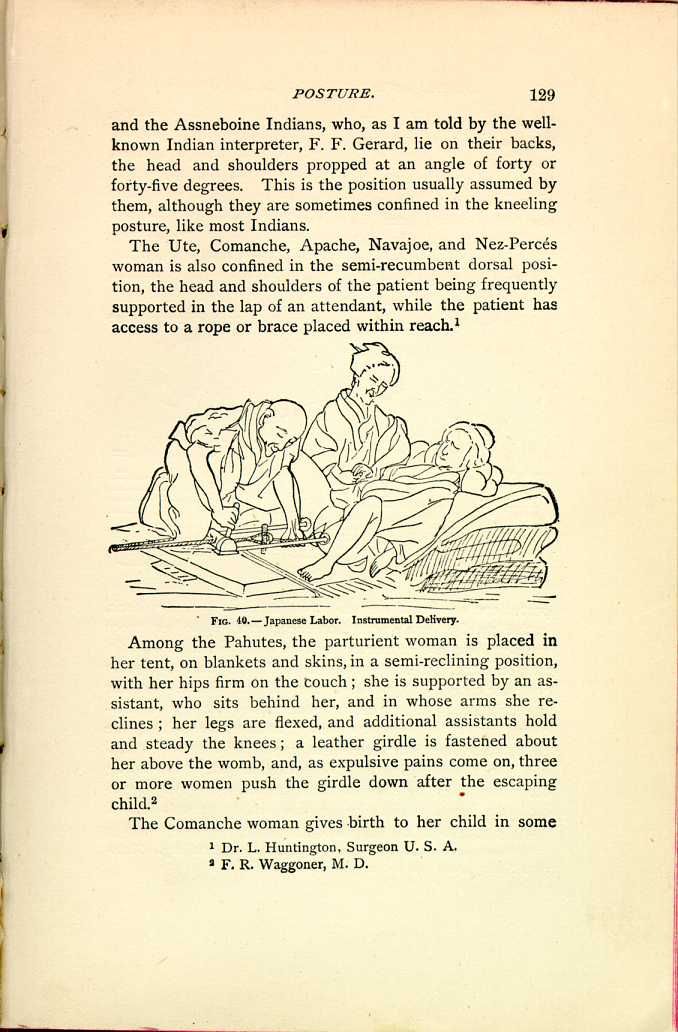
FIG. 40.—Japanese Labor. Instrumental Delivery.
[Description: Woman reclines on floor, with upper body elevated by bedding.
One person works with instruments designed to assist delivery while
another person sits nearby. Black and white illustration.]
Among the Pahutes, the parturient woman is placed in her tent, on blankets and skins, in a semi-reclining position, with her hips firm on the couch; she is supported by an assistant, who sits behind her, and in whose arms she reclines; her legs are flexed, and additional assistants hold and steady the knees; a leather girdle is fastened about her above the womb, and, as expulsive pains come on, three or more women push the girdle down after the escaping child.[120]
The Comanche woman gives birth to her child in some
The Hindoos seem to find the position convenient, as the
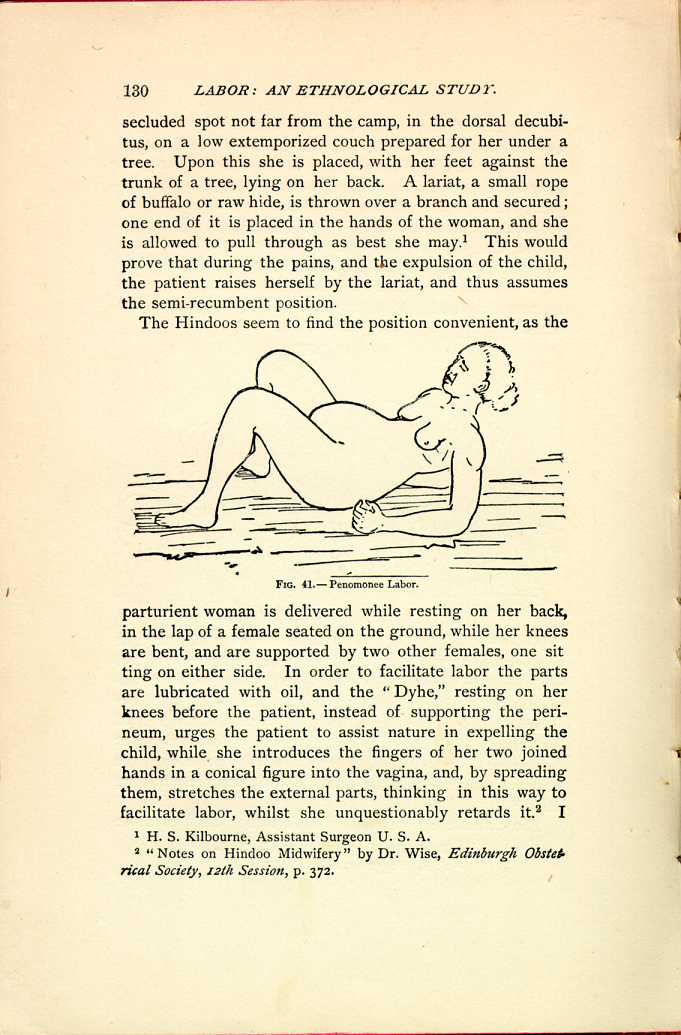
FIG. 41.—Penomonee Labor.
[Description: Woman reclines on floor, her upper body propped up on her
elbows, her knees bent and legs spread.
Black and white illustration.]
The dorsal decubitus, with the body at an angle of forty
or forty-five degrees, was common among the Romans.
Moschion describes it. Celsius[123]
and Paul of Ægina[124]
recommend
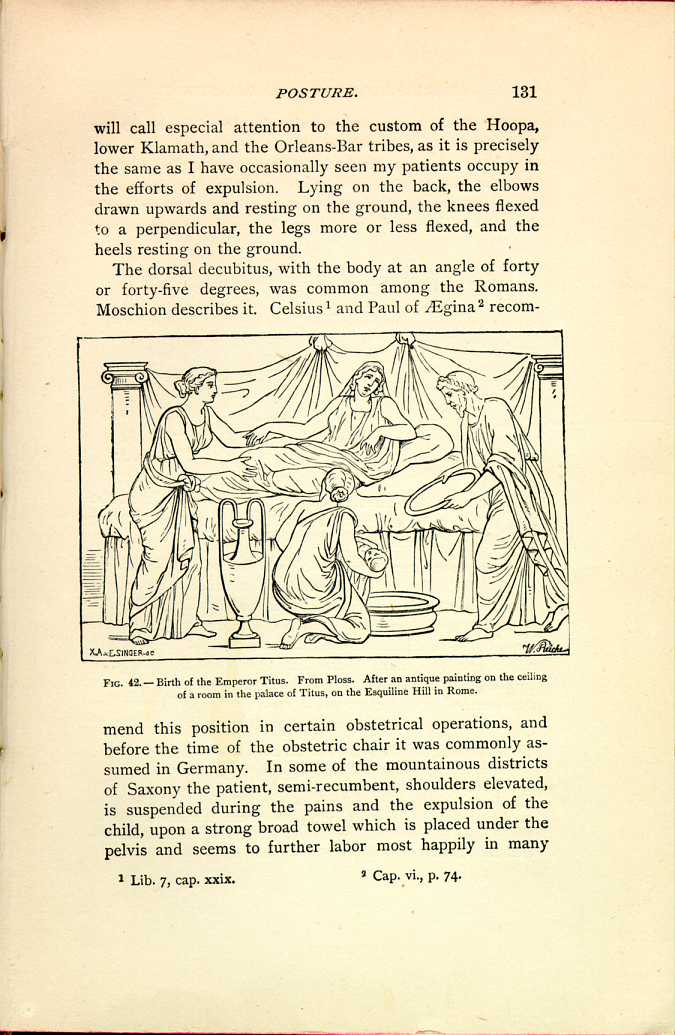
FIG. 42.—Birth of the Emperor Titus.
From Ploss. After an antique painting on the
ceiling of a room in the palace of Titus,
on the Esquiline Hill in Rome.
[Description: Woman reclines in bed as three other persons attend her, one
kneeling beside the bed with the newborn baby.]
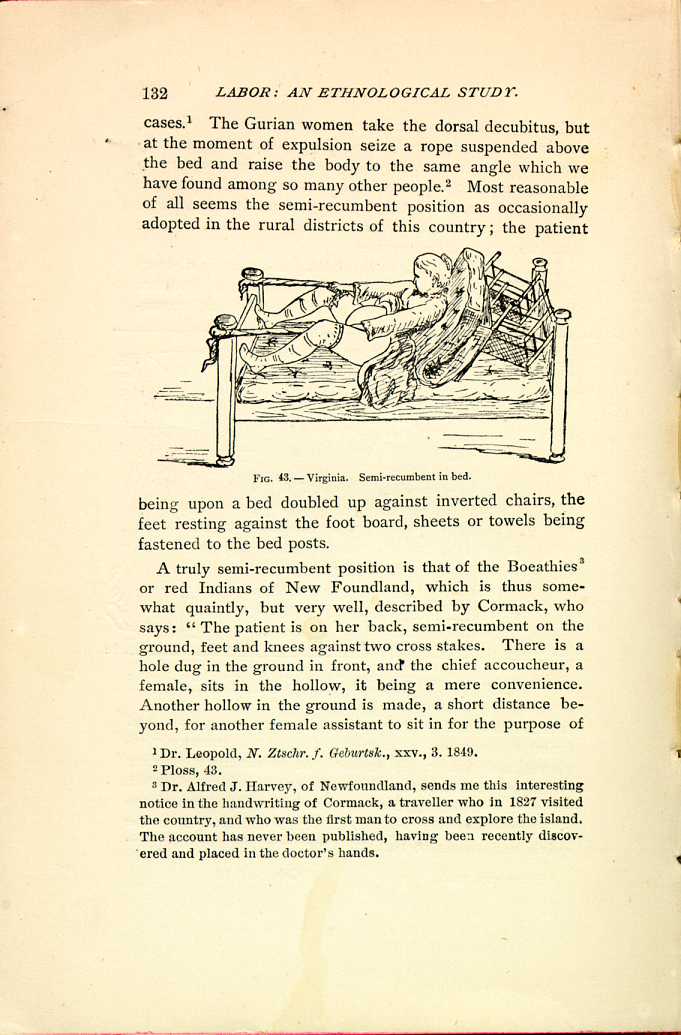
FIG. 43.—Virginia. Semi-recumbent in bed.
[Description: Woman reclines in bed, her upper body propped up by an overturned chair covered with bedding. In each hand, she holds a rope tied to a bedpost at the foot of the bed. Black and white illustration.]A truly semi-recumbent position is that of the Boeathies[127] or red Indians of New Foundland, which is thus somewhat quaintly, but very well, described by Cormack, who says: "The patient is on her back, semi-recumbent on the ground, feet and knees against two cross stakes. There is a hole dug in the ground in front, and the chief accoucheur, a female, sits in the hollow, it being a mere convenience. Another hollow in the ground is made, a short distance beyond, for another female assistant to sit in for the purpose of
Among the Turks, also, the semi-recumbent position prevails, but more erect, seated on ground, stool or chair.[128] Their customs are extremely interesting, as in many of the interior provinces they still cling to their primitive ways.
During the fifth or sixth month of pregnancy the abdomen is compressed by a firm bandage, and this pressure is kept up until full term to prevent the child from growing too large. Abortion is frequent, and is produced by breaking the membranes and allowing the water to escape. Delivery is always accomplished on the lap of an assistant, or seated in a semi-recumbent position on a bed or low stool, or even on the ground, leaning against the stump of a tree or the wall of a house, or some other convenient point. Thus we may say that it is always a sitting posture, either upon the lap of an assistant, upon the ground, or upon the obstetric chair.
Until recently, and even now in distant villages, it is still the custom for the midwife to carry with her the obstetric chair. This, according to my informant, is of a peculiar kind; a large, wooden seat, back chair with a circular opening cut into the front part of the seat, in this differing from all known forms of the obstetric chair, which consist of a mere semi-circular excavation in the seat, this, however, being a complete circle. This carrying about of the chair is the same custom which we have referred to in Syria and other Eastern countries, although the shape of the chair is different. In difficult labor the patient is placed upon a blanket held by four or six persons, and upon this she is rolled about, not tossed up and down as we have seen it customary in other countries.
During the earlier stages the patient lies at will, usually on her back, on a mattress placed on the ground; as labor advances, and the pains increase, one of the stronger of the women present takes the parturient on her lap, compresses the abdomen by her encircling arms, and urges the sufferer to bear down with all her weight. Various other methods are resorted to for the purpose of increasing the pains: thus the bent knees of the patient are constantly and severely jarred, or cold water is forcibly thrown upon the abdomen.
Their midwives are very fond of endeavoring to hasten labor by prematurely rupturing the membranes, cutting them with a sharp piece of salt—often cutting into the scalp as well.
The root of the Alizari (rubia tinctoria) is considered as an emenagogue by the nomadic Turucks, and during childbed the same remedy is resorted to to call forth the lochia when once checked.
In former times bleeding during pregnancy was resorted to with a view of preventing convulsions of the new-born, but is now pretty well given up.
C. HORIZONTAL, OR RECUMBENT.
We finally come to the horizontal or recumbent position, and by this I mean especially, 1. The Dorsal Decubitus, the obstetric position of the present day on the continent of Europe and in America, the head merely elevated by the ordinary pillow; 2. The Position on the Side, as customary in England; and 3. Horizontal, Prone on the Chest and Stomach.
1. The Dorsal Decubitus.
The semi-recumbent position held sway in Europe before the time of the obstetric chair, and after a period of great popularity soon disappeared, although its traces remained, especially in the slowly progressing country districts, until
The Chinese women are frequently confined in bed.[129]
Although this is the position which is taught by the laws of modern obstetrics, so perfect in all other respects, nature does not seem to have designed that woman should in this way free herself from her burden; at least it appears very strange that instinct, the correct guide of uncivilized people, should so rarely lead them to adopt the recumbent position; and it appears strange that, notwithstanding the most careful inquiry as to the position adopted by the savages, and notwithstanding the information I have received from surgeons who have come in contact with all of our Indian tribes, I have found scarcely any who assume a strictly recumbent position. Among some the women are confined in the dorsal decubitus, but rarely in the horizontal position. Among the Cheyennes and Arapahoes we sometimes find the dorsal decubitus in simple labors.[130] The Oregon Indians on the Siletz Reservation are invariably confined on the back with the feet drawn up. I am also told that others of the tribes on the Pacific coast follow this custom, especially those of the Grand Ronde Agency, Oregon; the parturient usually keeps on her feet during the first stage of labor, but when the expulsion pains set in she lies on her back, her head very slightly elevated (her bed always on the floor), her thighs well flexed on the abdomen; an assistant supports each knee and foot; the patient presses her hands against her thighs, or, when the pains become severe, she presses
The Nez-Percés and Gros-Ventre squaw assumes the stooping posture during the earlier stages of labor, with an assistant at her back, who clasps her body with her arms, and locking the fingers, brings the palms of the hands over the base of the uterus, making steady pressure backwards and downwards during the pains; in some instances, during the stage of expulsion, however, the patient lies down indifferently on either side or on the back, while if on the side, pressure by the hands of the assistant is kept up continuously, if on the back, the assistant remains by the side of the patient and keeps up the pressure in the before-mentioned directions.
Upon the Antilles the recumbent position is also assumed, though we have seen that other postures are equally common there. Among one of the African tribes, the Wanika, the parturient woman lies flat upon her back, and this is perhaps the only instance where the horizontal position is so decidedly described.[132] Of the Indian women, Susruta says, page 368, "When the child is to be born, let the woman be placed with the back upon a carefully spread couch, giving her a pillow, let the thighs be flexed, and let her be delivered by four steady, aged, and knowing midwives whose nails are well trimmed.''
In Southern India we find a similar custom to that observed among the Nez-Percés; the patient walks about in the earlier stages, then sits down with the legs stretched, her back supported by an assistant, whilst in the moment of expulsion she is placed upon her back.[133]
In Siam the patient is placed upon her back with a woman seated upon either side; these two assistants begin by forcibly pressing the abdomen downward and backward, the pressing of which is continued from three to five hours. If by that time it has failed to expel the fetus, one attendant
The Burmese practice is to strip the patient naked and
to compel her to run about the room, while half a dozen
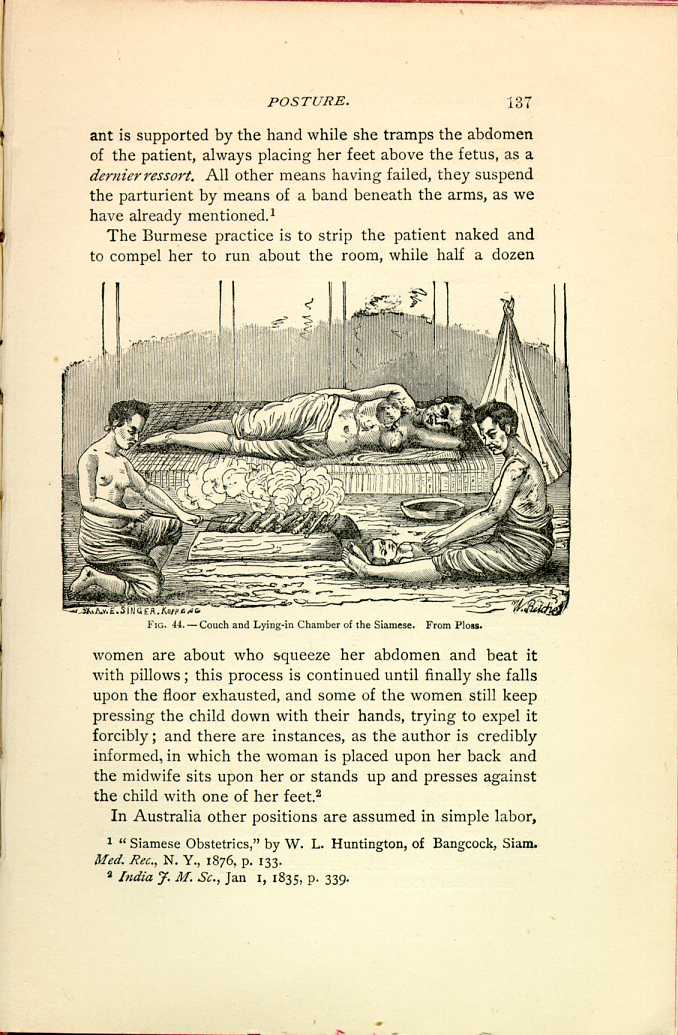
FIG. 44.—Couch and Lying-in Chamber of the Siamese. From
Ploss.
[Description: Woman reclines on her side on a bed. One attendant keeps a
fire burning nearby, while a second attends the newborn child. Black
and white illustration.]
In Australia other positions are assumed in simple labor,
In Astrakhan the Russian women are made to walk about unceasingly during the earlier stages, and only at the very last moment are permitted to lie down.
In Sumatra, if we may judge from a single case,[137] the patient is also confined in the recumbent position; and in Brazil, according to an old authority cited by Ploss,[138] the native women were confined upon the ground. Several other such vague authorities are cited, but they are hardly sufficiently reliable for our purpose.
2. The Lateral Decubitus.
The position upon the side seems almost entirely a product of modern civilization, and, I must say, of prudery rather than science; it is not adopted as the obstetric position by any of those people who still lead a natural life, though assumed, in a few rare instances, in certain stages of labor. The Nez-Percés squaws squat in the earlier stages, and lie upon the side or back during the expulsion of the child. The Modocs, on the contrary, first lie upon the side, and at the last moment take the knee-hand position. The women of the Laguna Pueblo, New Mexico, who follow their own inclination almost altogether in the position which they assume, stand or walk about in the early stages, but are confined standing, suspended in a half squatting position, or, if tired, on the back or side, with pillows between the knees; this latter position is also occasionally found among the Kootenai Indians, of Washington Territory; as Dr. Morgan writes, the woman is placed on her left side, under
With the exception of these few data, I can find no other reference to this position.
3. Prone upon the Stomach.
This peculiar position has but few adherents; in fact, I
can find no traces of it elsewhere than among the Creeks,
who assume an over-done knee-chest position; i. e., prone
upon chest and stomach, in ordinary cases. "When the
fetus is about to be expelled the mother straps the belt
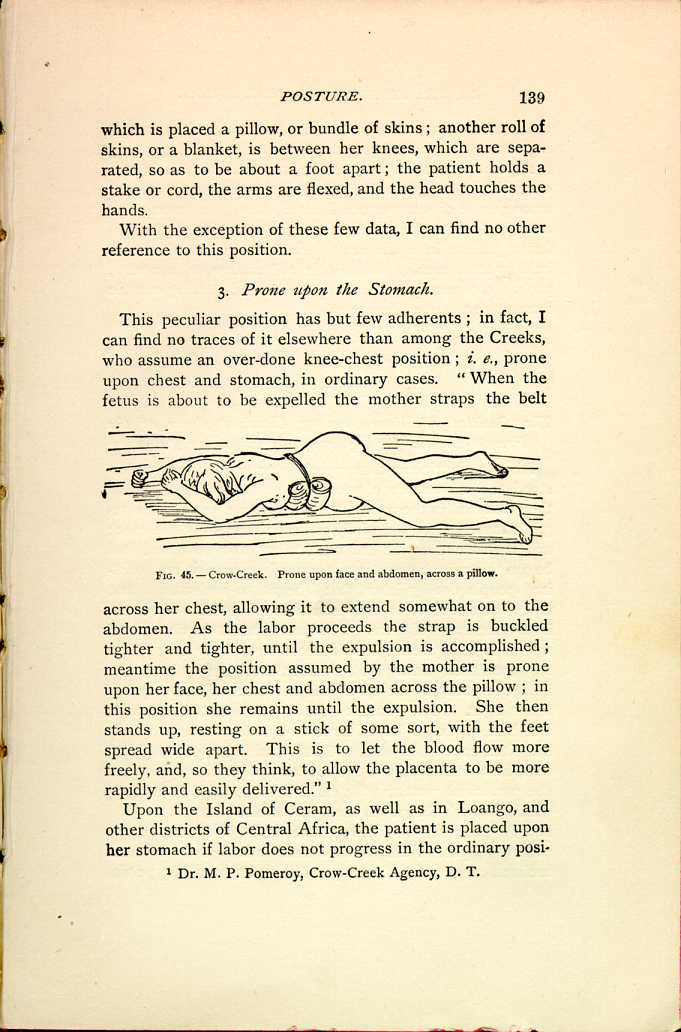
FIG. 45.—Crow-Creek. Prone upon face and abdomen, across a
pillow.
[Description: Woman lies face-down on the floor with her hands above her
head. A bundled cloth is bound above her abdomen. Black and white
illustration.]
Upon the Island of Ceram, as well as in Loango, and other districts of Central Africa, the patient is placed upon her stomach if labor does not progress in the ordinary position,
A peculiar custom may yet be mentioned which is still observed, to the great discomfort of the parturient woman, among some of our western Indians, as well as among the more civilized natives of Syria; and that is, to toss the suffering patient in a blanket, the four corners of which are held by stout men, so that she is well shaken, with a view, probably, of rectifying the malposition, and shaking out the fetus from the unwilling womb.
2. PART II.
The Position of Women among Civilized Races of the Present Day in the Agony of the Expulsive Pains.
Abler obstetricians than myself have undoubtedly understood the movements of women, and the positions which they assumed in the agony of the expulsive pains. As regards myself, I must candidly confess this was not the case; and it was not until I had undertaken this work, and had begun to study the positions assumed by savage and civilized people during labor, that I began to understand that there was a method in the instinctive movements of women in the last stage of labor. I had seen them toss about, and sought to quiet them; I bade them have patience, and lie still upon their backs; but, since entering upon this study, I have learned to look upon their movements in a very different light. I have watched them with interest and profit, and believe that I have learned to understand them. It has often appeared to me, as I sat watching a tedious labor case, how unnatural was the ordinary obstetric position for one parturient woman; the child is forced, I may say, upwards through the pelvic canal in the face of gravity, which acts in the intervals between the pains, and permits the presenting part of the child to sink back again, down the inclined canal. If we look upon the structure of the pelvis,
The contractions of the previously inactive and rested abdominal muscles are a powerful adjunct to the tired uterine fibre, in the last prolonged and decisive expulsory effort, and in the dorsal decubitus they are somewhat hampered; they act to the best advantage in the inclined positions, semi-recumbent, kneeling, or squatting. We know that the squatting position is the one naturally assumed if an effort is required to expel the contents of the pelvic viscera; we, moreover, all know how difficult, even impossible, it is for many to perform those functions recumbent in bed, and mainly because they have not sufficient control of the abdominal muscles in that position. Much more is this the case in the expulsion of the child; but the recumbent position is sanctioned by custom; it is pointed out as apparently convenient; it is imperatively demanded by prudery, and by a false modesty which hides from view the patient's body beneath the bed-clothes; and above all it is dictated by modern laws of obstetrics, the justice of which I have never dared question; we have all been taught their correctness, and we all thoughtlessly follow their dictates. There is no reason for assuming this position, though we are taught it; it is not reason, or obstetric science, but obstetric fashion which guides us,—guides us through our patients; and blindly do we, like all fashion's votaries, follow in the wake.
We have seen in the first part of this paper that the recumbent position is one but rarely taken by women among savage tribes, or among people who still follow their instinct and not the dictates of the latest obstetric fashion. Now what does civilized woman in the hands of the modern obstetrician do when in the intense agony of the last expulsive pains? She loses control of herself, forgets the admonition of her physician, and gives way to her own instinct.
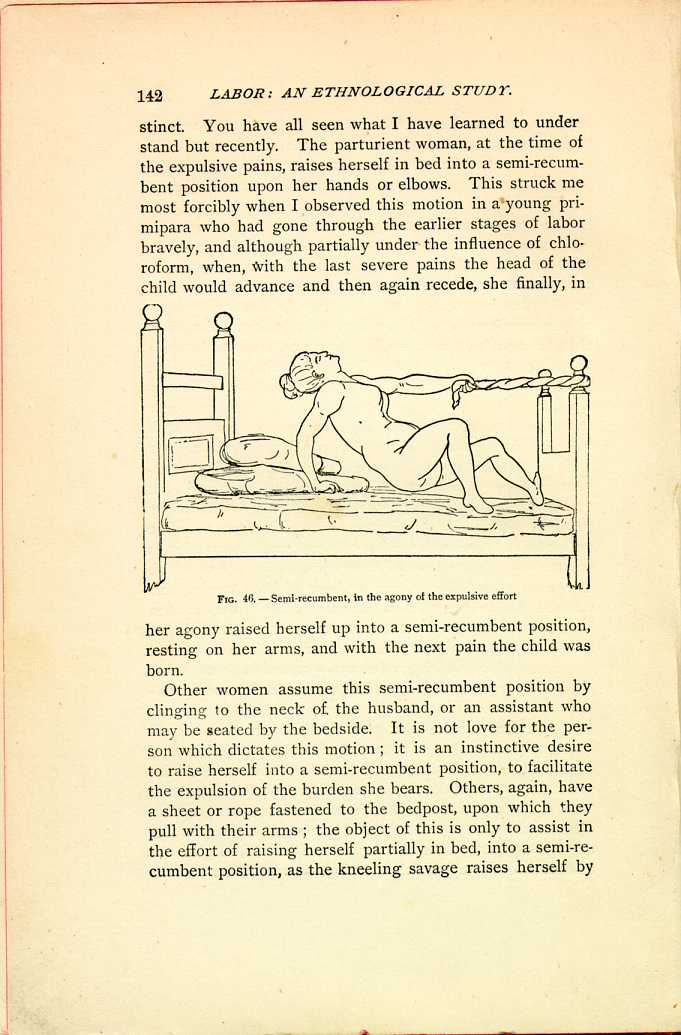
FIG. 46.—Semi-recumbent, in the agony of the expulsive effort
[Description: Woman on bed holds herself up with one arm while using the other to hold onto a rope tied to a bedpost at the foot of the bed. Black and white illustration.]Other women assume this semi-recumbent position by clinging to the neck of the husband, or an assistant who may be seated by the bedside. It is not love for the person which dictates this motion; it is an instinctive desire to raise herself into a semi-recumbent position, to facilitate the expulsion of the burden she bears. Others, again, have a sheet or rope fastened to the bedpost, upon which they pull with their arms; the object of this is only to assist in the effort of raising herself partially in bed, into a semi-recumbent position, as the kneeling savage raises herself by
I need hardly continue this evidence, as every one of the members is aware how frequently, in the last moments, a
RÉSUMÉ AND CONCLUSIONS.
I WILL briefly recall the more striking and important features elicited in the inquiries I have made in regard to the posture of women in labor.
I. The women of the various tribes and races are delivered according to customs, and in positions, which are peculiar to their people, whenever they are free to follow their own instincts.
(a.) These positions are now adopted as customary and traditional, but in the first place they were assumed because they had proved the safest and best; delivery, in simple cases, being thus accomplished in the shortest possible time with the least possible suffering.
(b.) So great do the advantages of posture in childbirth seem to be, that people cling to this custom more firmly than to any other of their traditions, as we have seen by the chair of the Cypriote midwife, who to-day reënacts the labor scene of 2,300 years ago; and of the native Peruvian woman, who is still confined as were her ancestors at the time of the Incas.
II. The positions assumed in civilised communities, by the advice of learned authorities, have varied greatly with the change in obstetric science, and with the demands of comfort and of modesty; thus, in the days of Greece and Rome, in the early centuries of the Christian era, a semi-recumbent position was advocated, either upon a low stool or in bed; later came the obstetric chair, and toward the end of the last century the dorsal decubitus, which has retained its supremacy, yielding, however, to the position on the side in the British Isles, and to the dictates of Nature in the agonies of the expulsive pains, when women will occasionally
III. The same woman often assumes various position in the course of a natural labor; usually, she is more at her ease in the early stages, and not until the pains become more regular, rapid, and severe, does she take the position in which she is confined.
Thus, the Coyotero-Apache squaw occupies any position she pleases, generally standing or walking about until bearing-down pains supervene (which, in fact, is almost universal among the North American Indians), then she assumes the squatting posture. The squaws of the Laguno Pueblo stand with their hands on their knees, much as they urinate, in the earlier stages; later, they stand up erect, supported by assistants or clinging to a rope. The Modocs maintain a curved position, lying on the side, until the labor is nearly completed, when they assume a position on their knees and hands, which is continued until the child is born.
Among the Nez-Percés and Gros-Ventres the parturient is in a stooping posture during the first two stages of labor, the buttocks resting on the heels, whilst during the expulsion of the child she lies down, on either side, or on the back.
IV. In the last stages of ordinary labor, those positions which I have classified as inclined are most frequently resorted to; most common of all is the kneeling position which we mainly find among the Tartars, Mongolians, and North American Indians: the squatting posture is also at home among our Indians, and among the Malays, the Australian and African negroes; equally frequent are the semi-recumbent positions, which, although resorted to by savage nations, are more closely connected with the progress of civilization. The ruder methods. such as the semi-recumbent position in the lap of an assistant, or on the ground, answer the same purpose as the more comfortable and refined posture in the obstetric chair or in bed.
Least frequent are the recumbent or horizontal, and the standing or erect postures.
V. In all positions, whether the patient is swinging by the limb of a tree, whether she is kneeling by a stake, or semi-recumbent in bed, there is a decided change in the axis of the body during the pain, and in the interval of rest; and usually the patient has a support of some kind within reach, a rope, a stake, or an assistant, by means of which she can change the axis of the body, and intensify the contractions of voluntary and involuntary muscles during the pains.
The pelvis itself is usually steadied, whilst the upper portion of the trunk sways to and fro.
Some of our Indians
walk about in
the interval, and
kneel down, clinging
to the stake during
the pain; for this
purpose the Comanches,
for instance,
have a number
of stakes planted
in the ground at the
place of confinement,
in order that the patient
may walk about,
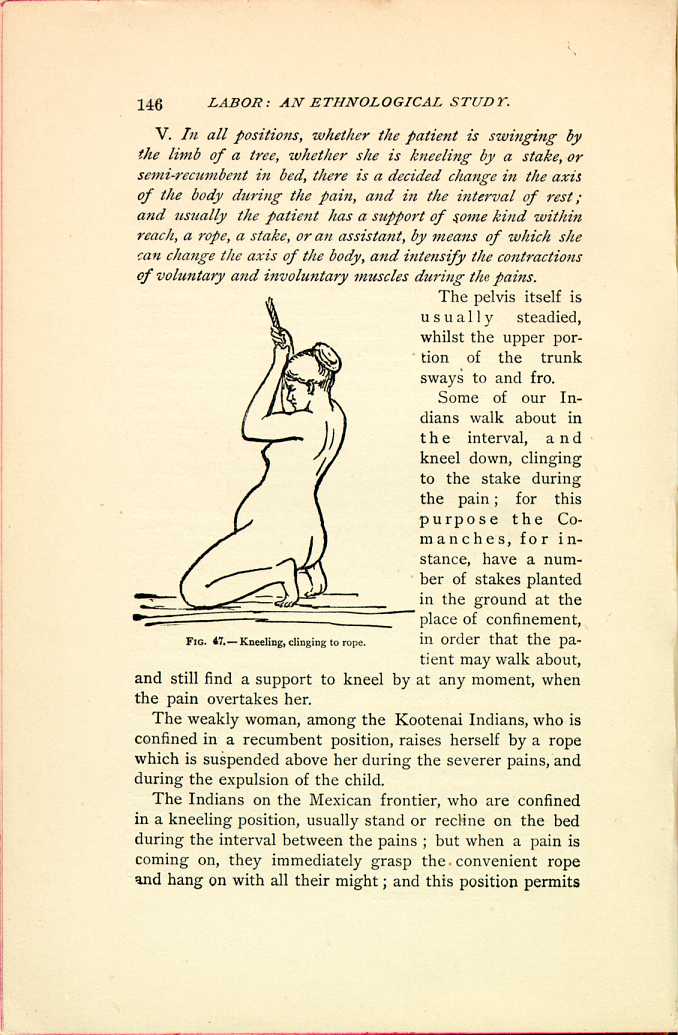
FIG. 67.—Kneeling, clinging to rope.
[Description: Woman kneels on the floor, holding onto a rope suspended
overhead. Black and white illustration.]
The weakly woman, among the Kootenai Indians, who is confined in a recumbent position, raises herself by a rope which is suspended above her during the severer pains, and during the expulsion of the child.
The Indians on the Mexican frontier, who are confined in a kneeling position, usually stand or recline on the bed during the interval between the pains; but when a pain is coming on, they immediately grasp the convenient rope and hang on with all their might; and this position permits
The native Mexican is often confined kneeling on the floor; in the interval between the pains she lets herself down, her buttocks resting upon her heels, whilst during the pain she raises the body, throwing it backward or forward, according to circumstances, and clings to a rope, an assistant, or the neck of the midwife.
Surgeon George W. Adair, U. S. A., justly characterizes the difference in the methods pursued by various people. He says: "The English midwife exhorts the patient to lean forward; in America, the feet are fixed, and the patient is given a rope by which she raises herself during the pain; the Mexican midwife fixes the knees and holds the upper portion of the trunk as in a vice, and pulls the pelvis forward, hinged, as it were, upon the acetabulum, and thus overcomes the dip of the plane of the superior strait, and straightens the passage with greater efficiency and certainty.''
Dr. Campbell closely observed the negro woman whom he saw confined in a kneeling posture, her arms resting upon a low chair, and saw that during the pain her body would move backwards so that her buttocks would rest between her heels, while in the intervals she would glide forward again, so that the thighs became perpendicular and the body horizontal.
VI. In tedious cases, when delivery is retarded and labor will not advance, a change is usually made in the posture of the patient, and massage is freely resorted to; thus, the Cheyennes, Arapahoes, Nez-Percés, and Gros Ventres, who assume the dorsal decubitus in ordinary labor cases, raising themselves into a semi-recumbent position during the expulsion of the child, resort to the knee-elbow position in difficult cases.
The Siamese, who usually assume the recumbent position, and our Coyotero-Apaches, who squat in ordinary cases, both suspend the parturient by bands about the
Upon the Pacific slope, where the dorsal decubitus is the rule in ordinary cases, the patient is partially suspended in a kneeling or squatting position in difficult cases; the Syrians, who usually permit their patients the comforts of the obstetric rocking-chair, toss them in a blanket to shake the child out, or turn it, if the labor becomes tedious.
Instinct and experience teach the savage that by a change of position, labor may be hastened or retarded, and involuntarily they change the axis of the body in a way most favorable to a natural and safe delivery, hastening labor as much as is compatible with the safety of mother and child; all the inclined positions, especially the kneeling and squatting, clinging to a rope, are such that the direction of the pelvic axis can be readily changed. It remains for the scientific observer to demonstrate with precision the positions which are the most favorable under given conditions.
Herr von Ludwig, the speculative and theoretical writer, who has been condemned and ignored by practical obstetricians, describes the knee-elbow position as the one which retards the expulsion, making it slower and safer in difficult cases, saving the perineum, and the kneeling position, with the body inclined forward, as the one which retards expulsion but moderately, with proper care of the perineum.
Although it is not within the scope of this study to discuss the question as to the best position for women in labor, we may well look to the ethnological facts cited for a solution of this puzzling and highly important problem, and I will outline the more important conclusions which have developed.
I. In the ordinary labor case, which is a purely mechanical process, the patient should be given greater liberty and should be permitted to follow the dictates of her instinct
II. In the earlier stages of labor the parturient must be guided in her actions, and in the position assumed, by her own comfort and by the dictates of her instinct; not only is this the invariable rule among savage races, but it was also warmly advocated by the shrewd and observing obstetricians of the past, and by those eminently practical and successful midwives of old.
III. The care with which the parturient women of uncivilized people avoid the dorsal decubitus, the modern obstetric position, at the termination of labor, is sufficient evidence that it is a most undesirable position for ordinary cases of confinement; and I am convinced that the thinking obstetrician will soon confirm the statement not unfrequently made by the ignorant but observing savage, by Negro and Indian, that the recumbent position retards labor and is inimical to easy, safe and rapid delivery.
Several of the most esteemed of my colleagues have already given me a very decided expression of their opinion, taking the same grounds practically and theoretically. Dr. Campbell, of Georgia, says that a careful study of the actions of parturient woman in her natural state will force us to permit our patients, sometimes, at least, to obey their own impulses, and to assume a squatting, kneeling, or sitting posture, in their attempts to deliver themselves; and this, he adds, "would, in my opinion, often do away with the necessity of resorting to the forceps, which, though a great blessing, too often become the reverse in the hands of eager obstetricians, who are inclined to use them on the least occasion, or without any real occasion at all.'' He has given me the history of a number of cases, most of which I have already cited, in which labor was retarded, progress had entirely ceased, and the propriety of the forceps was under consideration, when a speedy and unaided delivery followed a change of position from the routine dorsal decubitus to the squatting, sitting, or kneeling posture, as the instinct of the patient prompted; but be it remembered, the same patient,
The cases related by Dr. Campbell are as striking as the one told me by Dr. V. Mansfelde, of Kansas: the patient being in great distress, labor having continued for several days, entire cessation of pains in the usual obstetric position, their sudden recurrence upon assumption of an inclined position, their disappearance, with the certainty of a chemical experiment, upon a return to the dorsal decubitus, and final speedy delivery in the position of the patient's choice.
Dr. Wilcox, of Massachusetts, and others have related similar cases, most of which I have already given, but I cannot close without again referring to the views of my friend, Dr. Campbell: "I will say that I regard what may be called the Obstetric position, as generally practiced in this country, recumbent on the back, as not only the most unnatural, but the most disadvantageous and therefore the most unphilosophical; it is the position which, above all others, deprives the woman in labor of the advantages which gravity would give us in promoting expulsion; there the position almost nullifies the power of the abdominal muscles, leaving the almost unassisted uterine muscle to effect expulsion. The English method, on the side with the body bent forward and the thighs drawn up, is much more advantageous in so far as the abdominal muscles can act better.''
IV. In ordinary labor cases the expulsion of the child should be expected in an inclined position: Kneeling, squatting or semi-recumbent, in bed, on the chair or lap, as is done by the great majority of uncivilized people, and for the following reasons:—
a. These positions permit the free use of the abdominal muscles.
b. The force of gravity does not counteract the expulsive effort as in the recumbent position, nor does it unite with it too freely, and hasten labor unduly, as in the erect posture.
c. With the assistance of a rope, stake, or other support the parturient can vary the inclination of the body and correct the labor, hasten or retard the descent of the child, and relieve the
d. Injury to the soft parts is less liable to occur in these positions, if we may accept the rapid getting up, and freedom of our Indian squaw from all uterine diseases, as proof of this statement.
V. Of these positions the semi-recumbent is the most serviceable, and should be adopted as the obstetric position in all ordinary labor cases; it is preferable to the kneeling or squatting.
a. As more convenient and comfortable, not exposing the person, and not being objectionable to the modesty of the patient.
b. As affording more rest and not being tiresome, which is a serious objection to the kneeling and squatting position as applicable to the tender female of our civilization.
c. The semi-recumbent position in bed, the body at an angle of forty-five degrees, the hips resting on a hard mattress, thighs well flexed, is the easiest, most comfortable, and appears to afford the greatest relief, and the greatest freedom from pain, coupled with the greatest effect of the uterine contractions, relaxation of all the parts, and free play of the abdominal muscles.
d. The pelvis is more readily fixed in this position.
e. The perineum has a certain support which does away with the questionable proceeding of supporting the perineum during expulsion of the head and shoulders, by which more harm than good is usually done.
J. M. Hildebrandt, "Ethnographische Notizen über Wakamba und ihre Nachbaren,'' Ztschr. f. Ethn., Berl., 1878, vol. x., page 394.
Dr. W. J. Hoffmann, Miscellaneous Ethnological Observations among the Indians in Nevada, Colorado, and Arizona, p. 471. Haydens's Survey, 1876.
Herr N. von Miklucko-Macklay, "Anthropologishe Notizen gesammelt auf einer Reise in West Mikronesien und Nord Milanesien,'' Ztschr. f. Ethn, 1876, p. 126.
Bernouilli, Schweiz. Ztschr. f. Heilk., Bern, 1864, i. and ii., p. 100. Ploss, Die Lage und Stellung der Frau während der Geburt, Leipzig, 1872, p. 20.
Dr. L. L. McCabe, Physician to the Kiowa, Comanche, and Wachita Agency; Maj. M. Barber, U. S. A.
Brit. and For. Med.-chir. Rev, Lond, 1855, vol. xv., page 525. Hooker, Journal of the Ethnological Society, of London, 1569, page 69. Goodell, page 674.
This illustration is taken from Melli, as the cut is much more carefully finished than in Merourio, who entitles this plate: "A sito, nelqualo si debbono collocare le donne parturiente, che sono molto grasse.''
This position is advocated by Herr V. Ludwig as the most favorable one for the first stage of labor.
W. Eton, Schilderungen des türkischen Reiches ger., by Bergkt. Leipzig, 1805, page 144. Moreau, Natur-gesch. des Weibes, ii., page 194
R. Krebel, Volksmedic, etc., p. 55; H. Meyerson, Med. Ztg. Russlands, 1860, xxiv., page 189; Ploss, 36.
"Notes on Hindoo Midwifery'' by Dr. Wise, Edinburgh Obstetrical Society, 12th Session, p. 372.
Dr. Alfred J. Harvey, of Newfoundland, sends me this interesting notice in the handwriting of Cormack, a traveller who in 1827 visited the country, and who was the first man to cross and explore the island. The account has never been published, having been recently discovered and placed in the doctor's hands.
| CHAPTER II.
POSTURE IN LABOR. Labor Among Primitive Peoples | ||