A CASE OF POSSESSION
BY DONALD FRASER, M. D., GLASGOW
THE Demonaic possession of the middle ages and of
times nearer to our own was largely hysterical in
character, and generally occurred in Epidemics.
It was associated with the more superstitious and
emotional side of religious beliefs, where a real Hell fire and a
personal Devil with attendant Angels or Demons were believed
in, and feared, much more intensely and widely than
they are today even amongst the ignorant and superstitious,
while suggestion and contagion played a large part in its
spread, as it did in that other and more hateful form of it
known as witchcraft.
Esquirol who wrote clearly about it in his "Maladies
Mentales" under the heading of
"Demonomania,"[1] spoke of
it as being propagated "by contagion, and by the force of
imitation." This was illustrated in the Epidemic of Loudun,
amongst others referred to by him. This epidemic spread
to neighbouring towns menaced all the high Languedoc, but
was arrested by the wisdom of a Bishop, who did this by
depriving the movement of its marvellous elements. In this
epidemic form it was in its bodily and mental manifestations
really hysteria with characteristic stigmata and convulsions.
An excellent example of this religious hysteria was presented
as recently as 1857 in an epidemic at Morzines in upper
Savoy. It began with two little girls, pious and precocious,
who had convulsive attacks. It spread to other children and
then to adults. Amongst the younger of those affected,
ecstasy, catalepsy, and somnambulism were seen, and later,
convulsions only; convulsive attacks returned several times
a day. An attack usually began with yawning, restless
movements, the aspects of fear passing into fury with violent
and impulsive movements, with vociferations and cries that
they were lost souls in hell, the mouth-piece of the devil,
etc. These attacks would last from ten minutes to half an
hour. A feature of this epidemic was the absence of coarse
and erotic speech or gestures. Between the convulsions the
victims were restless, idle and inattentive, being altered in
character for the worse. In our day such epidemics are
represented, though in tamer fashion, by Revivalism in its
more noisy and extravagant eruptions. At all times, even
when such manifestations are not much if at all out of harmony
with ordinary religious feeling and action, there is a
tendency to pathological conditions. Often its subjects, in
the words of Professor James
[2] "carry away a feeling of its
being a miracle rather than a natural process, voices are
often heard, lights seen, or visions witnessed; automatic
motor phenomena occur; and it always seems after the surrender
of the personal will as if an extraneous higher power
had flooded in and taken possession." These are some of
the more striking phenomena of mysticism, and are also
largely pathological being amongst the major symptoms of
hysteria. The history and course of our case illustrated
very well this mixed condition. It has been pointed out that
the ecstasies, trances, etc., of the mystic, while essentially
pathological, have the evil effects of such morbid manifestations
modified or largely neutralized by the idealism behind
them, by that measure of true religious faith and feeling
which dominates the whole process in the case at least of the
higher mystics. The ore may be rough and very mixed,
but the precious metal is there also, as it was in our patient,
though the divine influence for which she craved was perverted
into that of the "Evil one." In the individual cases
described by Esquirol we recognize a more profound mental
disturbance than is shown in the epidemic or hysterical
variety. We indeed see many similar cases in our asylums
though we generally speak of them as Religious Melancholics
rather than as Demonomaniacs. In such cases recovery is
slow or may not occur, the patient passing into a state of
chronic mania, or of Dementia. There are other cases where
the religious emotions and ideals are completely subordinated
to or become identified with feelings of fear or remorse, the
result of fixed ideas of a shameful, distressing or frightsome
character. A good example of this condition though essentially
hysterical in its nature, is detailed by Pierre
Janet.
[3] The patient, a neurotic, respectable business man
thirty-three years of age, a good husband and father, on his return from
a business journey of some weeks' duration is found to have become
depressed and taciturn, and as the days pass his melancholy deepens. At
first he would not speak, but soon when he wished to speak could not,
making vain attempts at articulation. Under the influence of medical
ideas suggested to him his symptoms simulate first Diabetes next Heart
disease and his prostration becomes profound. By and bye he passes into
a state only to be described as acute Demonomania marked by maniacal
outbreaks in which he cried out and blasphemed, lamenting in quieter
intervals his powerlessness to resist the Devil who was, he believed,
actually not figuratively within him, who spoke and blasphemed through
him, prevented him sleeping, etc. After some months he was sent to the
Salpetriere where he came under the observation of Charcot and Pierre
Janet. He was cured by means of suggestion by the latter, who also
ascertained by his methods that the illness was the result of remorse
for an offence committed during the business journey which preceded the
outbreak.
In many ways our case differs from cases of this type.
An important difference was in the intermittent character
of the symptoms. For a period of two years the patient
alternated between a condition of acute misery from the
delusion that the evil one had entered into her body, and one
of apparent sanity. At the end of two years she was dismissed
cured, and has remained well for several years. She
differed also in the absence of blasphemous, extravagant or
obscene speech or action. The Devil never at any time
used her as the mouthpiece for devilish words or thoughts.
He was there, and as she insisted, in bodily form within her,
making her intensely miserable by his presence, and with the
feeling that she was cast away from "grace" and the privileges
of the religious life. Nor were there, as in the case
above referred to shameful or remorseful complexes at the
root of her mental condition. In presenting the facts of the
case, names and special marks of identification have been
altered.
Mrs. A., a widow, aged fifty-two years, was admitted
to the Paisley District Asylum in 1910 with a history of
having suffered for a month previously from mental depression
said to be due to distressing delusions of a religious
character such as that she was lost, was past forgiveness
and dominating and originating all such thoughts was the
belief that she was possessed by Satan or an evil spirit, who
was in bodily form within her. This delusion caused her
acute misery, and so absorbed her thoughts that she had
ceased to take any interest in her household affairs, and had
even talked of suicide.
Her condition on admission and for two years subsequently
was that of recurring states of this acute mental
distress, when she would rock to and fro, moaning and crying
out, often with tears over her lost and dreadful state, and
the presence in her inside of Satan or the "Evil one"
whom she said she felt within her, and who made her
"repulsive." This condition was varied with intervals of
usually from one to three days of apparently complete sanity,
when though quiet and somewhat reserved in manner, she
was quite cheerful. When questioned at such times as to
her delusion, she would admit its absurdity, but refer to an
uneasy sensation in the region of the left hypochondrium,
which, as she put it, surely meant that there was something
wrong there. She would be occasionally normal in this way
for a week or more, and on more than one occasion was so
well as to be allowed out on parole, but had often to be
brought back next day as depressed and delusive as ever.
She was always worse in the mornings, and often improved
as the day went on. She was a stout, pleasant featured and
intelligent woman, somewhat anaemic, and with a slight
bluish tinge of lips, though beyond a lack of tone in sounds,
the heart was normal. Her anaemic condition was accounted
for by her having suffered from menorrhagia for the greater
part of two years, which only stopped a few months before
her admission to the Asylum. It had during its continuance
brought on breathlessness on exertion, and what she called
spasms or "grippings at the heart," no doubt the basis of her
uneasy feelings in left hypochondrium. There was a slight
enlargement of the thyroid gland, but no symptoms referable
to it. None of these physical conditions beyond the
"grippings at the heart" it maybe, appeared to have any
appreciable influence on her mental condition, which as has
been noted above was normal until a month before her admission.
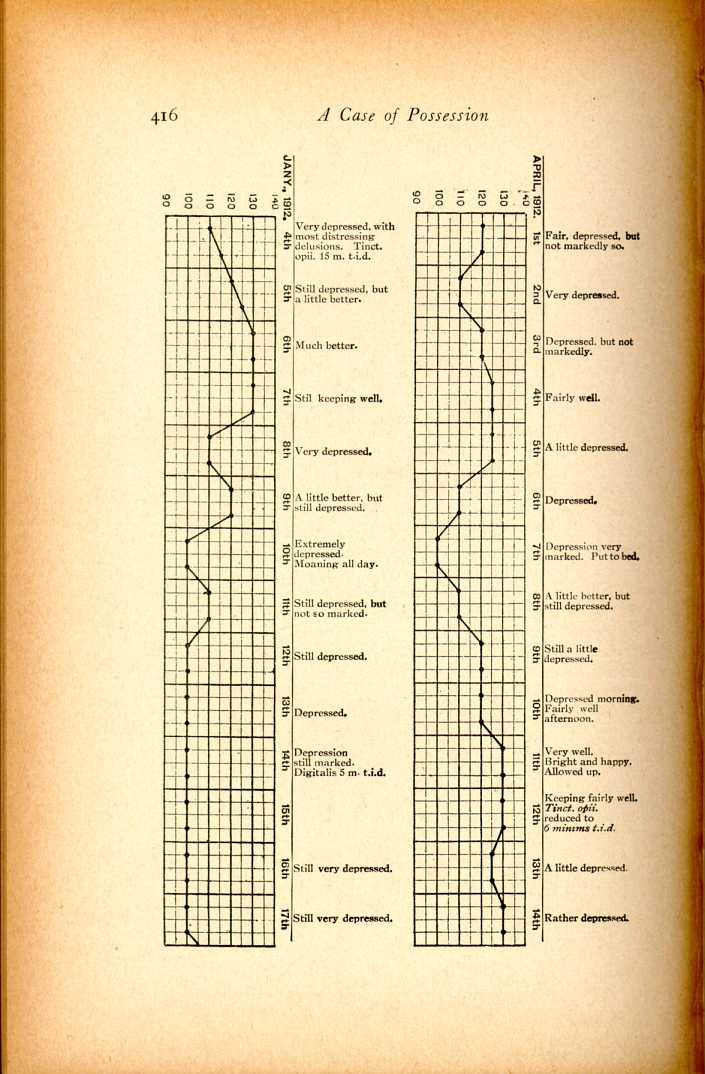
An interesting feature of the case was the relation
between her blood pressure and her varying mental states.
Her blood pressure was taken with a Riva Rocci Sphygmomanometer
morning and evening, sometimes oftener, during
the greater part of 1912-13, and it was noted that her depressed
or delusional states were marked by a low pressure,
while a high or relatively high pressure marked her sane and
cheerful states, contrary to what is usually observed in melancholia,
though similar to what is seen in agitated melancholia
and mania.
[4] Thus at a pressure of 130"H
G, she was
generally very well; at or about 120"H
G she was often well; at
110"H
G or 100"H
G she was always ill. When recovering, and
few weeks before dismissal there was a fairly steady pressure
of 118"H
G to 120"H
G day after day. It had been also noted
throughout, that during a continuous period of depression, or
of well-being, the pressure kept steadily high or low day after
day according to the mental condition. There was obviously
then a constant and close relationship between her blood
pressure and her mental states. At first sight it looked as
though those states were directly affected by the varying
pressure as it may have influenced the nutrition and therefore
the functions of the brain, and on physiological grounds
it is difficult to exclude such an influence altogether, even
though we come to the conclusion as we did that the variations
followed the emotional conditions, and did not precede
or cause them. The broad general statement has been made
that "each pleasurable emotion raises the general blood
pressure and increases the blood flow through the brain and
each painful emotion: brings about the opposite
result."
[5]
It cannot be said, however, that increased blood pressure
will give pleasurable emotion. The splanchnic area can be
acted on so as to raise the blood pressure without influencing
the emotions. We know also that when it is raised in melancholia
the increased pressure is associated with the reverse of
pleasurable emotion. Still on therapeutical as well as on other
grounds it appeared to us important to determine what, if
any, influence the raising of her blood pressure by drugs or
otherwise would have on her mental state. We did this by
baths, by abdominal pressure by means of a large sand-bag
laid over the abdomen, and by such drugs as adrenalin and
pituitrin. The results were disappointing so far as therapy
was concerned though of interest otherwise. The pressure
was raised by all these measures without any improvement
following such as occurred when it rose naturally. The rise
by abdominal pressure was marked and occurred quickly,
but without any apparent effect on her mental condition.
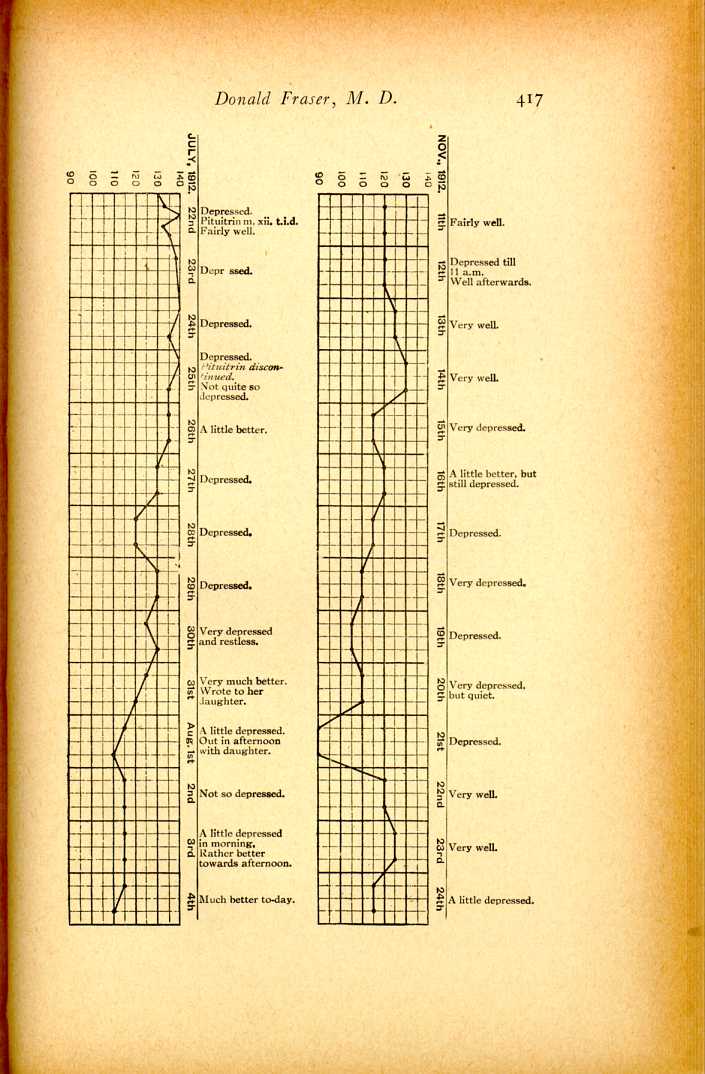
When it was raised to 140"H
G under the influence of pituitrin
there was marked depression as is shown in the chart for
July, 1912. Pituitrin given in m. v. hypodermically three
times a day, and after some days in larger doses by the
mouth, kept the pressure between 125"H
G and 130"H
G, but
with no corresponding mental improvement. For some days
after the pituitrin was stopped its influence seemed to persist
as the pressure kept high while the mental condition was low.
One of her longest spells of continuous mental depression
which lasted for twenty-seven days, occurred while her
pressure was high under the influence of adrenalin. Digitalis,
by the way, had no influence in any way on either her blood
pressure or her mental condition. The only drug we found
of any value was tinctopii in moderate doses three times a
day, but it gradually ceased to do any good.
Four charts from a very large number are given which
illustrate the above points.
It must be understood that these experiments while
accurate so far as they go, and carefully conducted under
my supervision by a competent assistant, were not made in
a well appointed laboratory, but were clinical observations
made in the crowded ward of a hospital for the insane. The
central disturbance here was the result of shock from sudden
and excessive fear acting on a highly sensitive subject as will
appear later. It has been shown by Cannon
[6] that such
major emotions as fear, rage, or pain acting upon the adrenal
glands through the autonomic nervous system are accompanied
by an increased discharge of adrenalin into the blood,
and by a passing of stored glycogen from the liver for circulation
through the body as dextrose, the object of which is the
increasing and liberation of muscular energy for the animal's
successful flight or fight. This discharge takes place very
quickly, and we are told that fright exhausts the adrenal
glands, a somewhat puzzling statement at first sight, but
borne out by the experience of our case where a fall of pressure
occurred under the paralyzing effect of extreme fear
and distress continued not merely for minutes but for hours
at a time. By and bye as her distress lessened and her expression
of it became more and more automatic, there was a
return to the normal adrenal discharge and consequent normal
rise in pressure. It is possible, of course, that there may
be another explanation in the inhibition of metabolism
caused by fear. Most of us have experienced the arrest of
salivation and digestion under the influence of fear or rage.
This inhibition would affect the products upon which the
adrenal secretion depends, but the more likely cause is where
this fear, in this case really a recurring representation of the
original shock, acts through the autonomic nervous system
on the adrenal glands. The emotional disturbance here then
was primarily of central origin, and was certainly not originated
by circulatory or visceral changes which were secondary
to it, and the facts do not support the James, Lange
theory of the emotions as it is generally understood. In
this connection we may refer very briefly to the laboratory
experiments of Sherrington
[7] and
Bechterew.
[8] The former
by spinal and vagal transection in a dog removed "completely
the sensation of the viscera, of all the skin and muscle
behind the shoulder. The procedure at the same time cuts
from connection with the organs of consciousness the whole
of the circulatory apparatus of the body. Yet the dog exhibited
rage, fear, disgust, etc., under appropriate stimuli as
a normal dog might do." The conclusion reached after
admitting possible objections to them is that, "the vasomotor
theory of the production of emotion becomes, I think
untenable, also that visceral presentations are necessary to
emotion." Bechterew, discussing this question as to whether
the vascular changes are anterior to the other processes,
which determine the alterations of the neuropsychic tone
according to the James, Lange theory, states that the experiments
in his laboratory by Dr. Serenewsky, appear to lead
to an opposite conclusion having shown that under the effects
of fear the alteration of the neuropsychic tone is produced
before the appearance of the cardiovascular phenomena.
There are no doubt objections to accepting laboratory
experiments upon inferior animals as conclusive where the
psychic part of the process in question is after all the
dominant one, nor must we forget that biochemical changes may
be as important as the integrity of nerves. We have however
referred to these experiments because of their bearing
on the conclusions to be drawn from the above described
clinical facts which so far as the initiation of the emotional
process is concerned confirm them; though we feel that the
bodily concomitants of the emotion are essential to its full
development, and that we owe much to James's presentation
of his theory even admitting its "slap dash"
[9] character to
use his own phrase. It was to be expected that the artificially
raised blood pressure would have had some effect in
improving the patient's mental condition, and in the case of
adrenalin, at any rate, some such effect should have occurred
if we are to accept the recently published conclusions of
Crilel
[10] to the effect that "adrenalin causes increased brain
action," "that brain and adrenalin action go hand in hand,
that is, that the adrenal secretion activates the brain, and
that the brain activates the adrenals." More in harmony
with the clinical experiences here is the fact according to
Biedl
[11] "that the adrenalin affects the intracranial and the
pulmonary vessels only slightly if at all." We presume that
what is true of adrenalin in this respect will be true of all
drugs which increase blood pressure. And while the rise of
the arterial pressure generally will accelerate the flow of
blood through the brain, yet we know that the cerebral
circulation is in "all physiological conditions, but slightly
variable."
[12] Besides, while that increased flow must necessarily
lead to increased cerebral activity, that activity may
be pathological as well as physiological, as in our patient,
who was quite uninfluenced mentally by the rise of blood
pressure which followed the administration of those drugs.
The nature and genesis of the emotional disturbance in this
case may be understood from the following history and
observations.
She had married happily at the age of nineteen years,
had a family of eight children, but had been a widow for
about twenty years. Her husband died suddenly abroad,
where she had lived with her family for two years after his
death, and acting on the advice of her friends, she came
back to this country bringing all her children with her.
This involved her in years of struggle and anxiety to bring
them up creditably, which she managed to do. During all
these years of widowhood and stress she was mentally well,
and latterly she described her life as a happy one surrounded
as she was by an affectionate and well doing family. She
had been brought up in a puritan household. Her father
and her husband had been deeply and consistently religious
though strict in their belief and observance of the letter.
This upbringing favoured a natural tendency towards religious
mysticism which was also promoted by the creed of
the church to which she latterly belonged, and of which she
was a deaconess. In this church the "gift of tongues" and
of "prophesying" was recognized as a part of its heritage,
and as she informed me in one of her normal times, she
occasionally spoke or prophesied in the public assemblies of
the congregation. I gathered that her utterances were generally
but a word or two of exhortation or pious aspiration,
given expression to in a moment of exaltation. From her
description of her state at such times, she was carried out of
herself, was oblivious for the moment of the presence and
actions of those about her, was in short in a state of ecstasy
when she "prophesied." A natural tendency to self-depreciation,
and to ideas of unworthiness asserted themselves
outside of those periods of exaltation, which were generally
followed by doubts as to her fitness to take part in such work,
and by the feeling as she expressed it "that she had presumed
as she was unworthy," and that God would be angry with
her for her presumption. Throughout her religious life she
had been always lacking in "assurance." Latterly this
feeling had grown in her and was evidently part of a deeper
feeling of mental depression, as she began to think often,
and with a feeling of dread that she had been surely too
happy these later years which stood in such contrast to the
poverty, struggles and disappointments of the early years of
her widowhood. This was her mental condition for some
little time before her attack of acute mental disturbance
which began one night a month before admission to the
asylum. She went to bed feeling ill and shivering as if from
a chill. In the middle of the night she woke up in a fright
from a vivid dream the contents of which merged in a strong
sensation as of a hand being pressed on her shoulder. She
described the sensation as being that of a positive feeling of
pressure, and with it came a feeling of dread, and the conviction
that it was the hand of Satan, so that she cried out
aloud to him to go out of the house, as it was blessed, referring
to the fact, as is the custom in her church that the minister
had blessed the house when she went to live in it. She
thought of calling to her daughter who was asleep near her,
but did not, and after a time fell asleep again being "comforted
by the feeling that the Lord would take care of her."
Next morning the effects of the "chill" had passed off, but
there was left a more or less constant feeling of vague dread
and fear of death, and with this a haunting idea born of this
strongly felt hallucination of external touch that Satan was
within her. The feelings of dread and fear grew steadily
and became too strong for her faith in the Lord taking care
of her, and very quickly her obsession as to possession by
Satan, became the definite delusion it was on admission to
the asylum. Hallucinations of what might be termed internal
touch leading to this idea of possession, are not unknown
in the annals of mysticism of the more morbid types of it.
Indeed the more ecstatic the mystic becomes, the more he
merges himself in his feelings and tends to develop hallucinatory
sensations. He is possessed, and desires to be possessed,
fortunately for him, by the Divine and not the evil spirit.
Hallucinations of external touch are as might be expected
more rare, though not uncommon we understand in the more
abnormal types, and occur in people supposed to be normal.
Havelock Ellis tells of a "Farmer's daughter who dreamt
that she saw a brother, dead some years, with blood streaming
from his fingers. She awoke in a fright and was comforting
herself with the thought that it was only a dream
when she felt a hand grip her shoulder three times in succession.
There was no one in the room, the door was locked
and no explanation seemed possible to her. She was very
frightened, got up at once, dressed, and spent the rest of that
night downstairs working. She was so convinced that a
real hand had touched her, that although it seemed impossible,
she asked her brothers if they had not been playing a
trick on her. The nervous shock was considerable, and she
was unable to sleep well for some weeks afterwards." The
writer's
[13] explanation is:—"it is well recognized that
involuntary muscular twitches may occur in the shoulder, especially
after it has become subject to pressure, and that in some cases
such contractions may simulate a touch." In illustration
of this he quotes from the Psychical Society's Report on the
"Census of Hallucination" the case of an overworked, and
overworried man who, a few minutes after leaving a car,
had the vivid feeling that someone had touched him on the
shoulder, though on turning round he had found no one near.
He then remembered that on the car he had been leaning on
an iron bolt, and therefore what he had experienced was
doubtless a spontaneous muscular contraction excited by the
pressure. Touches felt on awakening in correspondence
with a dream are not so very uncommon. We think as to
this likely enough explanation, that whatever the local
sensation may have been, or however slight, as it probably
was, it could only give rise to an hallucination of having
been touched by some external personality when it was
absorbed into, and became a part of a considerable emotional
disturbance as in the case of the girl above referred to, and
of my patient, in both cases associated with a frightsome
dream. The illness of the latter began with a dream, and
its continuance was in our opinion, largely due to dreams of
a painful character. During the whole period of her residence
it was noted that she dreamt a great deal, and that
they were terrifying or alarming dreams, and that her bad
days were generally preceded by a bad dream. Notes of her
dreams were regularly made, at one time for ten consecutive
nights, and only three of them were so far as she remembered
free from dreams. All of her dreams she described as "awful."
Many of them were of being mixed up with objectionable
people who behaved roughly and used profane language,
but, and of this she was very certain, who never talked or
acted obscenely. She frequently dreamt of being on high
precipitous places from which she was either falling, or could
not get away from. She described one vivid dream during
which she suffered great misery, and awoke from in great
distress. She dreamt that she was listening to a preacher
with open Bible in his hand, that he spoke about Peter whom
he was accusing of disobedience; a number of people were
present but she saw particularly only one man who looked
very happy; the sermon ended, and she awoke in "agony,"
this feeling being due, she said, to the conviction present with
her, that the sermon, and the man's happiness were intended
to show her how much she had lost since she was cut off from
"grace" by Satan dwelling in her body. Again she dreamt
of a near relative whom she heard singing, "And they all
speak in tongues to magnify the Lord." This brought
sorrow to her of which she was conscious during the dream
and after she awoke as she thought Satan was putting this
before her to show her what she had lost. In another dream
she saw three unpleasant looking men talking together. The
worst looking of them of Jewish appearance, came close to
her face, and argued with her about the evil spirit. She
said "he was in her body," and he answered "away with
him." She fell asleep and dreamt the same dream again.
These dreams were obviously governed by her dread and
fear as to her religious position. The following one is somewhat
different:—"A big brown beast came up to her and
pressed against her face; she slept again and dreamt she was
in a big ship sailing in black and dirty water; that she tried
hard to get out of the ship, but could not, and awoke in great
distress." We presume Freudians would find in the latent
content of all these dreams, particularly in this last one,
evidence in favour of their positions, though to us they
reveal only, in the blurred and broken way dreams do, the
prevailing trend of thoughts governed by morbid religious
fears and garbed in the phraseology and symbolism of a
judaic faith. The sameness of their ending and meaning to
her being obviously due to their relation to the dream which
ushered in her illness to which indeed most of them were
closely related in geneses and content. No doubt Freudian
psychoanalysis would be able to carry her memory back into
the region of long forgotten infantile or early sex memories
where, as in every normal human being they lie, the shadowy
outlines of instinctive feelings whose roots are in a far away,
phylogenetic past, having apart from suggestion no role as
factors in the production of morbid fears or fancies. The
fantastical and too often repulsive dream interpretations of
this school forcibly remind us of the words of Lord Bacon,
"With regard to the interpretation of natural dreams it is a
thing that has been laboriously handled by many writers,
but it is full of follies." All kinds of trivial incidents of
childhood and early youth are stored up by all of us, and are
recalled in sudden and unexpected ways, but not because of
any relaxation of a supposed "censor," nor necessarily because
of any content of a sex nature, but because they are
more often than not associated with fear, chief of the coarser
emotions, and a more primitive and more enduring emotion
than any of those connected with reproduction, and more
alien to the organism than sex memories even of a perverse
order, their resurrection being due to some subtle association
between the present and the past, generally a sensory one,
visual or auditory most frequently. In our own case the
earliest recollections of childhood are so associated and
recollected. Sunshine amongst trees, and birds singing
bring back to us at very long intervals a country scene
where as a child we were frightened by threats of a "bogie
man." The only childish incidents which unexpectedly
recur with us were associated with childish fears and
disappointments of a usual and ordinary character never
with morbid elements or emotional complexes which were
repressed or censored in the Freudian sense, and in this we
are not singular.
Again and again, association tests, as prescribed by
Jung, and repeated examinations of a psychological character
were made without our being able to obtain the slightest
indication of their being erotic or similar influences of the
slightest value as factors in the causation of her mental
disturbance. The chief value of Jung's Tests we have found to
be the suggestion of lines of inquiry or the confirmation of
evidence obtained in other ways. The results here were
negative and in that confirmed what we knew from the
history and character of our patient as a pure minded
woman of blameless life. She was constitutionally timid,
and all her life liable to doubts and fears of a morbid type.
As an instance of this she told us that when twelve years of
age while influenced by the death of her step-mother, which
had just taken place, one morning early her father went out
to his work leaving her in bed, and alone in the house.
Immediately after he left she heard or more likely thought
she heard, someone lift the latch of the door, as if to come in,
but though no one came in she was left in a state of great
fear, so marked that for long afterwards she dreaded being
left alone, and still remembers vividly her feelings during
that experience. This temperament she carried into her
religious life which as we have seen was marked by fears and
doubts. "No one will deny that fear is the type of asthenic
manifestations. Yet is it not the mother of phantoms of
numberless superstitions, of altogether irrational and chimerical
religious practices."[14] The strength and character of
her beliefs as well as the religious teachings and influences
to which she had been subjected from her earliest years, all
tended to develop the mystical in a temperament ready for
the dissociation necessary to enable the mystic to attain to
that ecstasy or absorption in something outside and beyond
the self which is the essence of that state. Why the ecstasy
which she knew and desired should pass into its opposite is
not difficult to understand when the above history is considered.
The shock which originated the attack gave form and
reality to fears and doubts which had been assailing her
for some time, and to the influence of which she was specially
liable at this time by the lowered physiological tension, the
result of her previous menorrhagia, and by the fact that the
comparative ease and comfort of her later life had given
her opportunities for introspection absent during her previous
life of struggle for and interest in others. She was then
scrupulous, timid and superstitious, a mystical, a psychopathic
temperament, taking her place all the same with
John Bunyan and other chief of sinners whose self-depreciation
and absorption in the struggle for salvation from sin
and the power of the Devil, though morbid in character was
not pathological. But when Satan became not merely a
spirit influencing her, but had entered bodily into her, the
border was crossed, and she was to herself literally possessed,
and became filled with fear, a fear pathological in action,
dominating her mentally and physically during her dissociated
states. Once initiated it is not difficult to see how
these dissociated states which recurred so regularly and
persisted so long were kept up by her temperament, and her
constantly recurring dreams of a terrifying or depressing
character, which were, as we have already indicated, but
representations of the original shock. The following quotation
applies closely to her case. "On this view an intense,
sudden painful experience, especially if the significance
of it can be dimly felt, but not understood, may persist long
and latently unassimilated by the central consciousness and
without fusion with it, almost as if it were a foreign body
in the psychic system."[15] Professor James has termed the
pathological emotion an objectless emotion, but as Professor
Dewey puts it "from its own standpoint it is not objectless;
it goes on at once to supply itself with an object, with a
rational excuse for being."
[16] Here the sensations in the
left hypochondrium which she had described as "grippings
at the heart," became the object which, under the influence
of the initial shock with its unusual and alarming sensations
and feelings, she interpreted as she did.
Her recovery was very gradual and marked by many
relapses. In her treatment as in our ideas as to the causation
of the disorder, we put the accent on the psychic rather than
on the physical factors. We did not however underrate
the latter but constantly sought to improve her bodily
health and condition. When at her worst in 1911 her
weight, taken monthly, was round about one hundred and
sixty pounds. In 1912 it went up from one hundred and
sixty-six to one hundred and eighty-eight pounds and averaged
one hundred and seventy-six pounds. But as in the
case of her blood pressure, the rise was due largely to her
mental improvement. It may be of interest to note here
that during and after a somewhat severe attack of diarrhoea
with hemorrhage from the bowels, her mental condition was
better than usual, as might even have been expected considering
the mental distraction the attack involved.
We were satisfied that we could have shortened materially
the duration of her illness—two years,—by hypnotic
suggestion, but unfortunately her friends objected to this
mode of treatment. Suggestion in the waking state had
been abundantly used, but with little apparent effect of an
immediate kind.
[[1]]
For a detailed account of it see the "Dictionary of Psychological Medicine"
under the heading "Demonomania."
[[2]]
The Varieties of Religious Experience; William James
p. 228.
[[3]]
"Nevroses et Idées Fixes" Vol. I, p.
377.
[[4]]
Maurice Craig, Lancet June 25, 1898.
[[5]]
Leonard Hill, "Cerebral Circulation" p. 74.
[[6]]
The interrelations of emotion as suggested by W. B.
Cannon. Recent physiological researches, The American Journal of
Psychology, April, 1914.
[[7]]
The Integration of the Nervous
System—Sherrington.
[[8]]
Bechterew "La psychologic objective," p. 312.
[[9]]
Psychological Review, Vol. I, where Prof. James admits
the defective presentation of his theory and uses the above words to
express it. He gives all due importance to the associated memories, and
ideas to which are related the incoming currents as well as all pleasure
and pain tone connected with them, etc.
[[10]]
S. W. Crile, "The Origin and Nature of the
Emotions," 1915.
[[11]]
Biedl innere secretion—Quoted by Cannon, 2 ed.
1913.
[[12]]
Leonard Hill—The Cerebral Circulation.
[[13]]
"The World of Dreams," p. 182.
[[14]]
Ribot "The Creative Imagination." p 34
[[15]]
Stanley Hall on Fear—The American Journal of
Psychology, April 1914.
[[16]]
Psychological Review, Vol. I, page 562.
 [Description: Image of a chart showing dates, states of depression, and blood
pressure.]
[Description: Image of a chart showing dates, states of depression, and blood
pressure.]
 [Description: Image of a chart showing dates, states of depression, and blood
pressure.]
[Description: Image of a chart showing dates, states of depression, and blood
pressure.]