| Massage and the Original Swedish Movements | ||
LATERAL CURVATURE OF THE SPINE
There are few affections in which the movement treatment has met with more signal success than in this. The aim should be to invigorate and develop the weakened and pathologically changed muscles of the convex side so as to restore the natural equilibrium of the two sides. There are but four known and acknowledged methods of developing muscles locally—viz., massage, movements, electricity and hydropathy. As the two latter do not come within the province of this manual we shall only describe the two first mentioned.
The main things to remember in treating lateral curvature of the spine are:
- 1. To elongate the spine by suspension.
- 2. To raise the lower shoulder.
- 3. To counteract rotation of the vertebrae.
- 4. Massage to stimulate the muscles.
160
- 5. Selected movements in carefully selected positions.
Massage of the back is very useful in most all cases of scoliosis, and the operator should pay special attention to the convex side, particularly in the early stages of the affection. The treatment should be applied also to the glutei the gluteus maximus in particular. Pinching is a very valuable manipulation, and when the patient becomes used to the massage apply it firmly, so as to reach the deeper layers of muscles. In older cases, it sometimes becomes necessary to treat also the muscles of the concave side, which from disuse have become atrophied. When the primary curve is high up, the cervical region should be faithfully attended to. Patient will often complain if too much pressure is used over the extreme convexity of the compensation curve—"the abrupt lower bend,'' as some patients style it.
We give here a list of the various Swedish movements used in the treatment of lateral curvature, and the operator who has been properly trained will experience no difficulty in selecting those which will prove the most beneficial to the individual case in question.
- 1. St. Bending to the (Convex) Side.—The patient stands
with hands clasped on the back of the head. The operator places one hand
on the highest point of the curvature and the other on the opposite hip,
the patient bending slowly about ten
times. It may also be used as a single active movement.161
- 2. St. Bending to the (Convex) Side.—Same movement as 1,
only the patient places the arm
corresponding to the lower shoulder-blade over his head as demonstrated in Fig. 118, the other hand on hip. Single active or duplicated active, in the latter case the operator placing his hands as in 1.
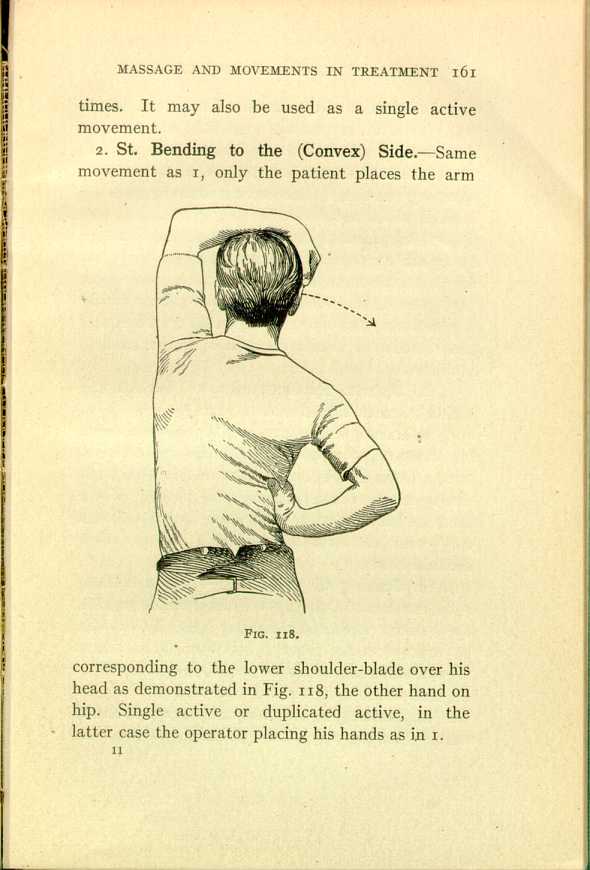
FIG. 118.
[Description: Drawing of a man from the back with his left arm curved over his head and his right hand at his waist. ]162 - 3. St. Rotation of the Arms.—The patient should stand as erect as possible with arms at sides; he should carry his arms slowly forward and upward, then backward and downward. A very useful respiratory exercise, besides acting strongly upon the muscles of the shoulders.
- 4. S. Separating and Closing of the Arms.— Described on page 85. It acts strongly upon the muscles of the chest, but also upon those of the upper part of the back. Kellgren says that if this exercise is performed with one arm at a time, correction of the rotation in lateral curvatures of the spine is produced.
- 5. St. Flexion and Extension of the Arms.— This movement is described on page 82.
- 6. St. Raising of the Arms.—The patient is standing with thighs supported; the arms are extended outward and raised upward by the patient, while the operator resists, grasping the wrists. If one shoulder-blade is much lower than the other, work only with the arm corresponding to the lower shoulder-blade.
- 7. St. Raising of the Arms.—This movement is the same as No. 6, only it is single active; that is, the patient performs it himself. He should raise his arms from the sides to above his head with a deep inhalation, afterward lower them slowly to original position, and exhale while doing so.
- 8. St. Bending of the Body Forward and Backward.—(See
Fig. 82.) The patient should place his
hands on his hips or clasp them on the back of his head. Another form of this exercise is performed in the following way: The patient stands with his limbs separated and his arms stretched straight up; he should bend slowly forward until the tips of the fingers touch the floor (see Fig. 83).163
- 9. L. Extension of the Back.—The patient is lying with legs on couch, the trunk extending; the operator supports the feet; the patient bends his body upward as far as possible. This is a very effective movement and must be given with care. At first it is safest to have some one to aid in holding the patient. He may place his hands on his hips, or clasp them on the back of the head; after he grows stronger he may keep them extended straight forward parallel with the ears.
- 10. L. on the Side, Bending the Trunk.—The patient is lying with legs on couch and trunk extended in side position, the convex side up and the feet supported. The bending should be performed slowly.
- 11. S. Raising of the Body.—The patient sitting on a stool or a turned chair with hands on back of head, bends forward, the operator resisting him when he resumes the original position. The lower shoulder may be raised up, as the operator has perfect control of the trunk by his firm grasp of the back.
- 12. St. Raising of the Body.—The patient, standing
with thighs supported against a couch or table
and hands clasped on the back of the head, bends forward as far as possible. The operator, standing behind and supporting the feet with his turned foot, places one hand on each side of the spine. The patient raises his body while the operator resists.164
- 13. L. Raising of the Body.—See page 146.
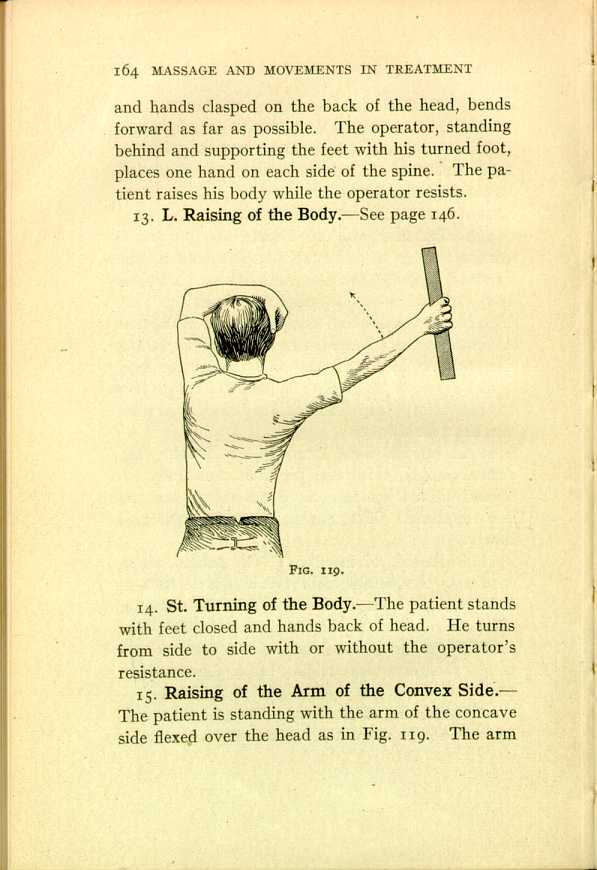
FIG. 119.
[Description: Drawing of a man from the back, with his left arm curved over his head and his right extended to the side. ] - 14. St. Turning of the Body.—The patient stands with feet closed and hands back of head. He turns from side to side with or without the operator's resistance.
- 15. Raising of the Arm of the Convex Side.— The
patient is standing with the arm of the concave side flexed over the
head as in Fig. 119. The arm
of the convex side is raised from the side to the head. A weight is generally used. Careful instructions in regard to respiration should be given.165
- 16. St. Bending of the Knees; Book on Head ("Deep
Knee-Bend''). The hands are placed on the hips with fingers in
front; the patient bends
slowly downward, counting: (1) raising on the tiptoes; (2) bending down as far as possible; (3) resuming tiptoes position; (4) back to original standing position (see Fig. 120). The effort of keeping the body erect in balancing makes this a very useful exercise in the earlier stages of curvatures.
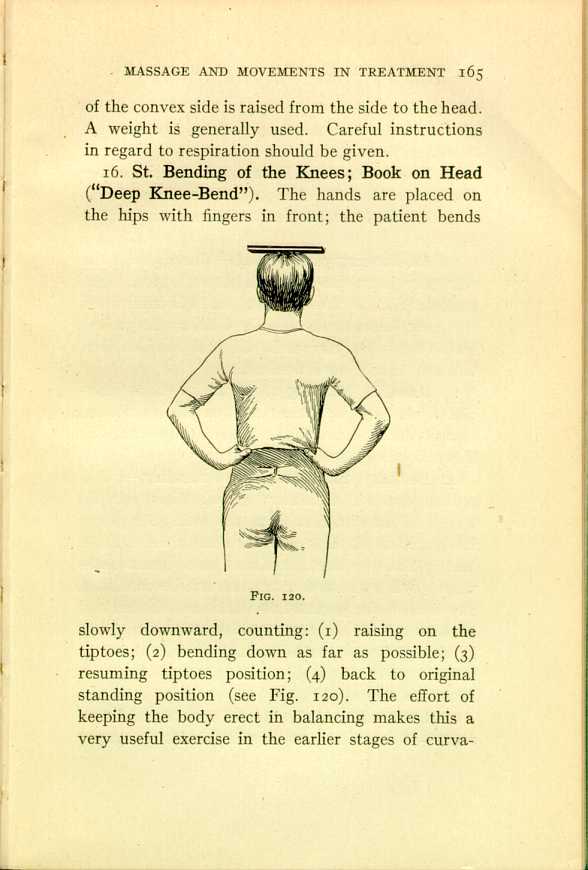
FIG. 120.
[Description: Drawing of a man from the back, balancing a flat object on his head. ]The operator should watch the patient carefully to see that the proper position is maintained from start to finish.166 - 17. Stretch-standing Bending of the knees.— Similar to 16, only the patient stands with his arms stretched upward close to his ears, as shown in Fig. 54
- 18. St. Bending of the Body.—The right (if the convexity is on the right side) foot forward; right hand on hip; left arm raised up and left hand down the back, between the shoulder-blades; the patient should bend slowly forward. Generally single active, but may also be duplicated active.
- 19. Kneeling Bending of the Body.—Same exercise as 18, only the patient rests on the knee of the concave side and places the foot of the convexside forward. Single active.
- 20. Bending Backward; Free-standing.—"The patient stands at a distance somewhat less than the length of his own foot from the wall. He places his hands on his hips with his elbows well thrown back. Then he stretches himself and bends backward. When the movement can not be continued any farther, the patient falls back until the back of his head touches the wall by which he stands. Then he slowly rises up on his toes, and while doing so draws a deep inspiration and goes slowly down again'' (Kellgren).
- 21. St. Bending of the Head Forward and
Backward.—The patient stands with his hands against
the wall and with his feet about twenty inches from the wall; the operator places his hand on the back of the patient's head and resists in the movement. This movement is very effective, and the author suggests that the reader have it applied to himself so as to personally feel its effect upon the different muscles of the back.167
- 22. St. Stretching of the Vertebral Column.— This is a new movement, recommended by the well-known Mr. H. Kellgren, of London. The patient stands as straight as possible; the operator stands in front of him and places one hand on the patient's head, and with the other he steadies him by placing it over the sternum or abdomen; he presses firmly down with the hand on the head, while the patient is told to stretch upward as far as possible. Be careful to see that it does not become only a simple raising of the shoulders. We want a stretching of the whole spinal column.
- 23. Susp. Bending of the Head.—The patient is suspended a few inches from the floor. The operator, standing at his side, places one hand on the forehead, the other on the back of his head. The patient moves the head forward and backward, the operator resisting, according to the strength.
- 24. Susp. Separating and Closing of Legs.— If the
patient is weak, make the movement active at first, while the operator
supports the sides. Afterward make it concentric, the operator grasping
around the ankles.
168
- 25. Susp. Flexion of Legs upon the Abdomen.— The patient is suspended and flexes his extended limbs upon the abdomen. This is a very strong movement and should be used only when the patient's strength allows.
It is very important to watch the patient in regard to his position for each movement. A rest should be given after every exercise, and it may be well to mention that the most complete rest is obtained when the patient lies flat on his abdomen with pillows under chest and stomach. Measure the patient's height; also curvature itself. This is best done by putting the end of the tape-measure on the vertebra corresponding to the extreme point of the convexity; carry it forward over the highest point of the convexity to the sternum or a fixed point of the sternum; then measure the concave side in the same manner and you will know from time to time how your patient improves. Always have a set rule to measure either before or after taking the movements. It becomes the operator's absolute duty to explain to the patient the tedious process of the treatment and the patient's own responsibility in regard to the final result. Exercise should be taken every morning and evening in the patient's own home. The results are remarkably good if proper judgment is used in the selection of movements. This treatment for curvature of the spine is very little known in America, but if given a fair trial, and the movements properly
A few cases of Pott's disease have been treated by the author. Massage of back and chest with respiratory movements were given with good results. Of course it will be understood that there was no inflammatory process going on in the spinal column at the time of treatment. By the use of the pneumauxetor the author fully convinced himself of the increased respiratory capacity. The patients would invariably express themselves as feeling more able to hold the head and thorax erect and the increased respiratory power was always a great relief in this very trying deformity.
| Massage and the Original Swedish Movements | ||